Open Access
Research Article
Max Screen
Copyright: © 2020 Tajima F. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Objectives: Previous studies reported that the paraspinal muscles of adolescents with severe idiopathic scoliosis scheduled for surgery contain higher proportion of type Ⅰ fibers on the convex side. However, the muscle properties are unknown in mild adolescent idiopathic scoliosis. The objective of this study was to evaluate the differences among the convex, concave and control sides of the paraspinal muscles in patients with mild AIS and healthy individuals and to help in the treatment of mild AIS patients.
Methods: Eleven women with mild adolescent idiopathic scoliosis (AIS group: mean Cobb angle=21.1±5.8, range =11-30) and 10 healthy women of similar anthropometric characteristics (control group) participated in this study. All subjects performed the unsupported trunk holding test until exhaustion. The results of surface electromyographic power spectral analysis were compared between the test and control groups. The median frequency (MF) was derived from the raw surface electromyographic signal of the erector spinae and multifidus during trunk holding test using Fast Fourier Transform spectrum analysis. The rates of changes in MF were calculated.
Results: No significant differences in endurance time were found between the AIS and control groups. The MF slopes of the erector spinae and multifidus were similar among the convex, concave and control sides.
Conclusions: The results showed that the composition of paraspinal muscle fibers does not change unless the Cobb angle is greater than 30 degrees. Therefore, some kind of conservative treatment, such as bracing and/or physical therapy, should be considered at early stage
Keywords: Adolescent idiopathic scoliosis; Electromyography; Muscle fatigue; Muscle fiber composition; Erector spinae; Multifidus
List of abbreviations: AIS: Adolescent Idiopathic Scoliosis; MF: Median Frequency; SEMG: Surface Electromyographic; LBP: Low Back Pain; MVC: Isometric Maximum Voluntary Contraction Force; SD: Standard Deviation
Scoliosis is defined as a heterogeneous group of conditions consisting in changes in the shape and position of the spine and trunk. Adolescent idiopathic scoliosis (AIS) is the most common form of scoliosis, being present in approximately 2% of Japanese adolescents, with higher incidence in females [1,2]. Scoliosis is diagnosed as lateral curvature of the spine greater than 10o as measured by the Cobb method on a standing radiograph [3]. The decision to treat such patients is conventionally based on the degree of the curvature. Depending on the individual case, Cobb angle of 20 to 40o is a mild AIS and should be treated conservatively, such as bracing and/or physical therapy. However, surgery is usually recommended for severe cases of AIS (Cobbangle of >40o) [4,5].
While the exact cause of AIS remains elusive, several theories have been proposed, such as hormonal, metabolic, neuromuscular, growth, and genetic abnormalities [5]. Still, so far no single causal theory for AIS has prevailed and it is still a conundrum and regarded as a multifactorial disease [6,7]. Muscle imbalance has also long been recognized as a possible etiological factor in AIS [6,8- 10]. Histopathological studies of paraspinal muscles of patients with severe scoliosis scheduled for surgery showed predominance f type I fiber on the convex side (and the respective lower proportion of type I fibers on the concave side) of the scoliotic curve [11-13]. On the other hand, similar data are not available on mild AIS since muscle biopsy is an invasive procedure. Thus, whether asymmetry of paraspinal muscles is the cause of AIS remains a matter of debate. In addition, the knowledge of bilateral changes to the fiber type in mild AIS could provide valuable information for understanding the cause of AIS and potentially improving AIS treatment approaches to maintain/recover the function of the side that may be affected.
The trunk holding test also known as “Sørensen back endurance test” with surface electromyographic (SEMG) power spectral analysis is a reliable method for measuring the fatigue rate of paraspinal muscles and identifying differences in the muscle fiber type by the slope of the median frequency (MF) [14-19]. Furthermore, this test is widely used by clinicians.
The aim of this study was to evaluate the differences in paraspinal muscles among the convex, concave and control sides in subjects with mild AIS and healthy individuals using SEMG power spectral analysis.
Eleven low back pain (LBP)-free women with mild AIS (AIS group: mean Cobb angle=21.1±5.8, range =11-30) and 10 LBP-free healthy women of similar anthropometric characteristics (control group) participated in this study. Table 1 lists the anthropometric characteristics of each group. All subjects of the AIS group had no history of surgery. All subjects were checked clinically by an orthopedic surgeon and underwent plain X-ray examination of the spinal column. The exclusion criteria were acute or chronic LBP, cardiovascular, respiratory, neurological, and endocrine diseases. The present study was approved by the Human Ethics Committee and written informed consent was obtained from all subjects and from the parents of each under 18-year-old volunteer before participation. This study followed the same test protocol as the previous studies [17-19].
Trunk extensor muscle strength was measured with a hand-held dynamometer (ANIMA; μTas F-1). After resting for 15 minutes, the subject was positioned prone over two treatment tables that could be lowered; the upper body rested over the table, while the anterior superior iliac spines were positioned on the edge of the other table, supporting the lower body. Three straps were used to stabilize the hips, knees, and ankles.
MVC was measured with the subject in the prone position, while the hands were placed behind the head and elbows out to the sides, head mid-line. The end piece of the dynamometer was applied to the inferior angle of the scapulae on the center of the back between the shoulder blades (Figure 1). The subject was asked to take 1 to 2 seconds to achieve maximum effort. The test was performed three times with a 30 second interval and the maximum force was recorded.
After a 30-min rest, the subject was positioned prone over two treatment tables; the upper body was rested over the table while the anterior superior iliac spines were positioned on the edge of the other table, supporting the lower body. Three straps were used to stabilize the hips, knees, and ankles. The upper table was lowered, and the subject was instructed to keep the upper body in a horizontal position in relation to the lower body. Specifically, while the subject performed the trunk holding test, she was instructed at the beginning of the test to lift the upper trunk clear of the table. The subject was then instructed to place the hands behind their head and their elbows out to the sides and maintain the unsupported upper body in a horizontal plane as long as possible (until exhaustion). The horizontal position during the test was controlled by a small sack (hanging from the ceiling), which was placed between the scapulae (Figure 2). The test was terminated when the subject could no longer maintain the upper body in the horizontal plane (defined as >2 cm reduction in height for two seconds) despite strong verbal encouragement. The endurance time was recorded using a stopwatch and was taken as an indicator of back extensor muscle isometric endurance.
The SEMG activity was monitored during the trunk holding test. For this purpose, the skin was cleaned with an alcohol swab before attaching the electrodes, and a pair of silver-silver chloride surface electrodes was placed over each erector spinae at L1 level, located 3 cm lateral from the midline, and each multifidus at L5 level, located parallel to the line between the caudal tip posterior spina iliaca superior and the L1-L2 interspinous space. The diameter of the recording electrode was 10 mm, and the bipolar electrodes were 2 cm apart. The signal was bandpass filtered (8-500 Hz), amplified using MQ 16 (MQ16; Marq-Medical of Denmark), digitized using an A/D converter (Vital Recorder2; Kissei Comtec) and stored on a computer at a sampling rate of 2000 Hz. The MF indices were derived from the raw SEMG signal as described above and plotted against time during the test using the Kinema Tracer Fast Fourier Transform spectrum analysis program (Kissei Comtec). Linear regression analysis was applied to MF time series (MF as a function of time) to calculate the MF slope. To allow comparisons between individuals, values during each test were expressed as a percentage of baseline.
Data were expressed as mean±standard deviation (SD). Differences in MVC and endurance time between AIS and control groups were analyzed using the Student t test. Differences in the MF slope of erector spina and multidus between the left and right sides were further analyzed in the control group using the paired t test. The results showed no differences in each muscle. Therefore, we adopted the left side as the control side, as described in previous studies [18,20]. The results of MF slope were analyzed using the Kruskal-Wallis test for differences among the convex, concave and control sides. A p value < 0.05 denoted the presence of statistically significant difference. Statistical analysis was performed using The Statistical Package for Social Sciences software, version 20.0.0, for Windows (SPSS; IBM Inc).
There were no differences in MVC and endurance time between the AIS and control groups (MVC: 152.2±33.5 vs 157.3±38.0 Nm, p=0.75; endurance time: 145.4±62.4 vs 122.8±29.3 sec, p=0.31).
The MF values of the erector spinae (L1 level) and multifidus (L5 level) decreased linearly with time in all subjects (p< 0.001) (Figure 3). The MF slopes of the erector spinae during the trunk holding test were -18.1±6.9, -18.1±6.8 and -16.8±3.4 %/min on the convex, concave and control sides, respectively. On the other hand, the MF slopes of the multifidus during the trunk holding test were -23.1±10.7, -21.1±9.7, and -19.0±8.2 %/min on the convex, concave and control sides, respectively. There were no differences in MF slopes of erector spinae and multifidus among the convex, concave and control sides (erector spinae: p=0.91; multifidus: p=0.71) (Figure 4).
The main finding of the present study was the lack of difference in the MF slopes of erector spinae and multifidus on the convex and concave sides of the scoliotic curve in individuals with mild AIS. The results suggest that the curves with Cobb angles of less than 30 degrees do not alter the paraspinal muscle fiber composition.
Our study investigated paraspinal muscle fatigability of the erector spinae and multifidus muscles during the trunk holding test in young females with mild AIS compared to healthy controls by using SEMG power spectral analysis. The MVC and endurance time were not significantly different between the test and control groups. Also, there were no significant differences in the decreasing rate of MF slopes among the convex and concave sides of individuals with mild AIS and the control sides of healthy individuals (Figure 4). In other words, our results suggest that the paraspinal muscles of individuals with mild AIS were identical with those of healthy individuals.
SEMG power spectral analysis is sometimes combined with histochemical analysis to determine the muscle fiber type [21-23]. Muscles with a greater proportion of type II muscle fibers exhibit greater reduction in MF over the course of the contraction [23]. In this way, the decreasing rate of MF slopes can predict the muscle fiber type composition [23,24]. The erector spinae contains relatively higher proportion of type I muscle fibers, befitting its function as a postural muscle [25]. Also, the relative area of type I muscle fibers in the erector spinae (which accounts for the relative size and composition of the muscle fiber type) correlates significantly with the MF slope recorded during the trunk holding test [21]. Our study demonstrated that the MF values of the erector spinae and multifidus decreased linearly with time in all subjects with mild AIS. Furthermore, the results of MF analysis suggest that the paraspinal muscle fiber composition on the convex and concave sides of individuals with mild AIS were identical to those of the control.
Many studies described abnormalities of paraspinal muscles in patients with AIS. The predominance of type I fibers on the convex side in patients with severe scoliosis has already been published [11-13], and its asymmetric characteristics have been reported to be associated with the severity of the Cobb angle [13,26]. One important point to emphasize in our study is that the subjects had mild AIS with Cobb angles of less than 30 degrees. Since the composition of muscle fiber type in our subjects with mild AIS was identical to the control, it is possible that muscle fiber type composition in AIS is unchanged, as long as the Cobb angle is relatively small (less than 30 degrees). Thus, the appearance of asymmetry in muscle fiber type composition could be considered a marker of more pronounced deterioration. The convexity versus concavity modifications in severe AIS seem more likely to be secondary adaptations of the muscle in reaction to the structural changes of scoliosis. AIS is a multifactorial disease [5], and muscle imbalance has been considered one of the causes of AIS [9,10,27]. Overall, the present study provided evidence in disagreement with the hypotheses that asymmetry of muscle fiber type composition is the primary cause and suggested that the curves with Cobb angles of less than 30 degrees do not alter the paraspinal muscle fiber composition.
The trunk holding test evaluates the endurance of paraspinal muscles [18]. Its results are considered to correlate with those of SEMG power spectral analysis when quantifying the fatigue rate of the back muscles [28]. Although muscle fatigue has been described in patients with chronic LBP, previous studies reported that paraspinal muscles in patients with chronic LBP displayed more type II fibers, the endurance time during the trunk holding test was shorter in patients with chronic LBP, and the slopes of MF were significantly higher compared to those of the healthy subjects [29]. Furthermore, it is known that the back muscles of men have a significantly higher proportion of type II fibers than type I compared with women [21], as other studies confirmed the presence of gender differences in the SEMG power spectral analysis [17,18]. The results of these studies showed clear differences in endurance time and the slopes of MF based on differences in the components of muscle fiber type. In the present study, there were no differences in the endurance time between subjects of the two groups. This finding also suggests similarity in fiber type composition between individuals with mild AIS and the control subjects. To our knowledge, the trunk holding test had never been studied so far in individuals with AIS. This was the first study that evaluated the endurance time of trunk extensor muscles in AIS. Although there is still room for investigating individuals with severe AIS, we assume that the findings of this study are reliable and clinically valuable. The endurance time may assist in prediction of the curve at risk for progression in AIS patients.
Depending on the individual case, the result of this study suggests that conservative treatment should be provided before the Cobb angle exceeds 30 degrees, including bracing and physical therapy. Many studies have assessed the asymmetry of paraspinal muscle fiber composition between the convex and concave sides in individuals with severe scoliosis scheduled for surgery [11- 13]. However, there is still the question of which side of the curve is more affected. Establishing the extent to which the bilateral paraspinal muscles are affected requires comparison with the control samples of the corresponding muscles. Mannion et al. [12] obtained bilateral samples of the paraspinal muscles during surgery from 14 female scoliotic patients. They found a significantly lower proportion of type I fibers in the muscle on the concave side of the scoliotic curve, but no difference on the convex side, compared with control muscle [12]. However, our findings showed similar paraspinal muscle fiber composition in the convex and concave sides of patients with mild AIS compared with the control side. It is concluded that asymmetry of muscle fiber composition between the convex and concave sides is limited to patients with severe AIS and fiber pathological change on concave side is more severe. Therefore, we assume that trunk exercises that maintain symmetric paraspinal muscle fiber composition are appropriate for patients with mild AIS and propose that endurance exercises that asymmetrically activate the paraspinal muscles on the concave side are important in the medical management of early-stage AIS. The EMG signal amplitudes recorded in exercises that asymmetrically activated the erector spinae and multifidus have been listed by Ekstrom et al. [30] Among them, we suggest that one of the best physical therapy programs to prevent the progression of AIS is the dynamic trunk side bending exercise when lying on the convex side with the lower extremities stabilized as long as possible.
This study has several limitations, including a relatively small sample size and negative data. A future study with a larger sample size to better evaluate mild AIS in required.
To our knowledge, this is the first study to evaluate the properties of paraspinal muscles of patients with mild AIS using SEMG power spectral analysis. The results indicated that the properties of paraspinal muscles on the convex and concave sides in patients with mild AIS are similar to healthy individuals. These findings suggest that 1) asymmetry of muscle fiber composition between the convex and concave sides is limited to patients with severe AIS, and 2) exercises that asymmetrically activate the erector spinae and multifidus in patients with mild AIS are important to prevent the progression of AIS.
The authors thank Yuuhi Taniguchi, Chigusa Ohno and Yoshinori Yasuoka for the technical assistance and Hideaki Tanina, Yuta Minoshima, and Hideyuki Satou for their help in completing all procedures described in the present study. We also thank Dr. Faiq G. Issa (www.word-medex.com.au) for the careful reading and editing of the manuscript.
The authors have no conflicts of interest directly relevant to the content of this article.

![]()

 |
| Figure 1: Body position during evaluation of trunk extensor muscle strength |
 |
| Figure 2: Body position during trunk holding test |
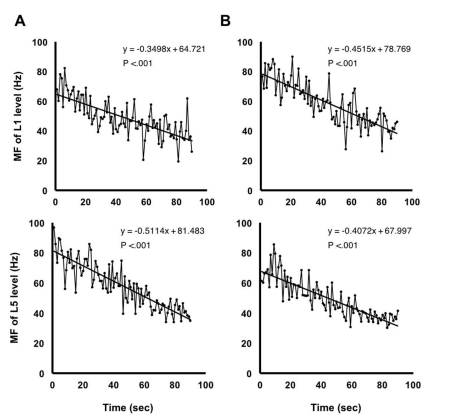 |
| Figure 3: Changes in MF of L1 level (erector spinae) and L5 level (multifidus) on (A) convex and (B) concave sides in a subject with mild AIS (Cobb angle 16o). MF decreased linearly with test time in all subjects |
 |
| Figure 4: The MF slope of (A) Erector spinae and (B) Multifidus during the trunk holding test among the convex, concave and control sides. |
|
Control (n=10) |
AIS (n=11) |
P value |
Age (years) |
20.3±1.3 |
20.8±1.3 |
0.37 |
Height (cm) |
159.8±3.4 |
157.5± 4.4 |
0.18 |
Body weight (kg) |
53.5±5.5 |
50.9±4.6 |
0.26 |
Body mass index (kg/m2) |
21.0±2.7 |
20.6±1.8 |
0.65 |




































