Open Access
Research Article
Max Screen
ISSN: 2767-4649
Copyright: © 2021 Wieselberg SB. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Objectives:To investigate the association between platelet values and COPD severity using linear variables in order to better explain and explore these correlations.
Methods:This is a cross-sectional study performed with patients from the ABC Medical School Pulmonary Rehabilitation Outpatient Clinic, male or female, over 40 years of age with previous COPD diagnosis. The following clinical data was collected: serum platelet count and mean platelet volume, spirometric parameters and the responses from St. George’s Respiratory Questionnaire, which is an instrument designed to measure the impact on overall health, daily life, and perceived well-being in patients with COPD.
Results: Transversal analysis of data revealed a moderate correlation between platelet number and post-bronchodilator Tiffeneau index (p = 0.031), with effect size of 37.55%. Also, an association tendency was shown between the number of severe or unpleasant respiratory events in the last three months and higher values of MPV (p = 0.085), with effect size of 29.20%.
Conclusion:The systemic and hypoxemic inflammatory condition established in COPD has an influence on megakaryiocytopoesis, promoting an increase in platelet turnover and MPV. Since MPV is a marker of platelet activation and responds to the same stimulus that lead to thrombocytosis, it can be a more sensitive index than platelet count, and thus can be used as an early marker of lung severity. Based on our results, we can infer that COPD, likely by means of the inflammatory pathways involved, may impact platelet counts and MPV values. That seems to be especially true for patients with better response to bronchodilators, which favors the hypothesis of inflammatory involvement.
Keywords: COPD; Platelets; Thrombocytosis; Spirometry
List of abbreviations:COPD: Chronic Obstructive Pulmonary Disease; CAT: COPD Assessment Test; 6MWT: 6 Minute Walk Test; SGRQ: St. George’s Respiratory Questionnaire; MPV: Mean Platelet Volume; FEV1: Forced Expiratory Volume during 1st Second; FVC: Forced Vital Capacity; BD: Bronchodilator
Chronic Obstructive Pulmonary Disease (COPD) is a respiratory illness, typically determined by a progressive and irreversible obstruction of the airflow from the lungs. This disease is related to long-term exposure and inhalation of toxic particles or gases, frequently caused by tobacco smoking [1]. According to the Cancer National Institute from Brazil, between 85% and 90% of all deaths among COPD patients can be attributed to cigarette smoking [2]. COPD natural course is characterized by recurrent exacerbation episodes, in which the respiratory symptoms become more intense than the usual day-to-day variation, including dyspnea, coughing and wheezing [3].
Recent studies indicate a potential association between higher serum platelet count and COPD exacerbation episodes [4-8]. In addition, it has been shown that not only the serum count, but also platelet’s activation is increased in patients with this lung disease, being even more intense during exacerbation episodes [9]. This repercussion contributes to inflammatory reaction amplification, hypercoagulation status and also promotes tissue injuries [9].
Indeed, Fawzy et al. executed two observational multicenter studies (SPIROMICS and COPDGene), in which they found that thrombocytosis was related to higher probability of prior exacerbation episodes and more aggressive respiratory symptoms suggesting that serum platelet count could be used as a biomarker to evaluate moderate and severe symptoms among COPD patients [4].
On the other hand, recent experimental studies have shown that the lungs may be a reservoir of hematopoietic progenitor cells and the site of platelet formation [10,11], suggesting that chronic lung diseases could lead to thrombocytopenia. In view of this hypothesis, Skoczynski et al. performed a controlled retrospective study, seeking to define the influence of the advanced COPD stage on the platelet count. However, it did not find differences between COPD patients and the control group [12].
As seen, the references are controversial and uncertain. Although Fawzy et al. has found a positive correlation between thrombocytosis and the severity of COPD, this effect is contradicted by smaller studies. Even more so, by adopting a categorical cut-off at 350.000 platelets, the effect size is harder to measure. Therefore, the present study has the aim to investigate the association between platelet values and COPD severity using linear variables, and including the mean platelet volume in the analysis, in order to better explain and explore these correlations.
This is a cross-sectional study approved by the Human Research Ethics Committee of the ABC Medical School, located in the city of Santo André – São Paulo, Brazil (protocol number: 3.373.764).
Patients enrolled in the study were selected from the ABC Medical School Pulmonary Rehabilitation Outpatient Clinic. Consecutive patients were included if they fulfilled the following criteria: male or female patients over 40 years of age with previous COPD diagnosis in accordance with the Global Initiative for Chronic Obstructive Lung Disease criterion of FEV1 /FVC < 0.70 after bronchodilator use. Patients were excluded if they had any other respiratory disease. All participating volunteers gave written informed consent, in accordance with Brazilian National Health Council Resolution 466/12.
The following clinical data was collected: a blood sample, a spirometry and the responses from St. George’s Respiratory Questionnaire (SGRQ).
Patients who had previously taken a blood sample for any reason, reported on the prior three months, could bring the result to account for the study. Otherwise, they had to perform a new blood collection at the ABC Medical School laboratory during the course of this research. From this laboratory examination, data collected were: serum platelet count and mean platelet volume (MPV). The plateletgram was performed by automation and confirmed with peripheral blood smear.
Regarding the spirometry, it was performed with the “PDS Ferraris Respiratory Koko-Trek Spirometer” by a pulmonary physiotherapist from the ABC Medical School Pulmonary Rehabilitation Outpatient Clinic. The bronchodilator used in the test was salbutamol sulfate, at a dose of 400mcg
The forced expiratory volume during the first second (FEV1) and forced vital capacity (FVC) ratio pre- and post-bronchodilator (BD) values were collected from the Outpatient Clinic data of those who had exams reported between January 2019 and January 2020. The others had to do a new spirometry during the course of this study. It is important to note that this ratio, also known as Tiffeneau index, is a spirometric parameter that represents the proportion of a patient's vital capacity that they are able to expire in the first second of forced expiration, used in the diagnosis of obstructive and restrictive lung disease.
Finally, as the St. George’s Respiratory Questionnaire (SGRQ) is an assessment tool for COPD evaluation, some of the volunteers had already responded to it in the previous three months, of whom the responses were collected from the Outpatient Clinic data. For those who had not recent responses, it was applied during the study. It is important to stress that this questionnaire is significant as a disease-specific instrument designed to measure the impact on overall health, daily life, and perceived well-being in patients with obstructive airway disease. The questionnaire consists of 50 items, divided into two parts: the first one questions about symptoms’ frequency and severity and the second takes into account the impact of the disease on daily activities. The total score ranges from 0 to 100, with higher scores indicating more respiratory limitations. Besides the final score, this study emphasized the fifth item of the first part of the questionnaire, which investigates the number of serious or very unpleasant respiratory events in the past three months.
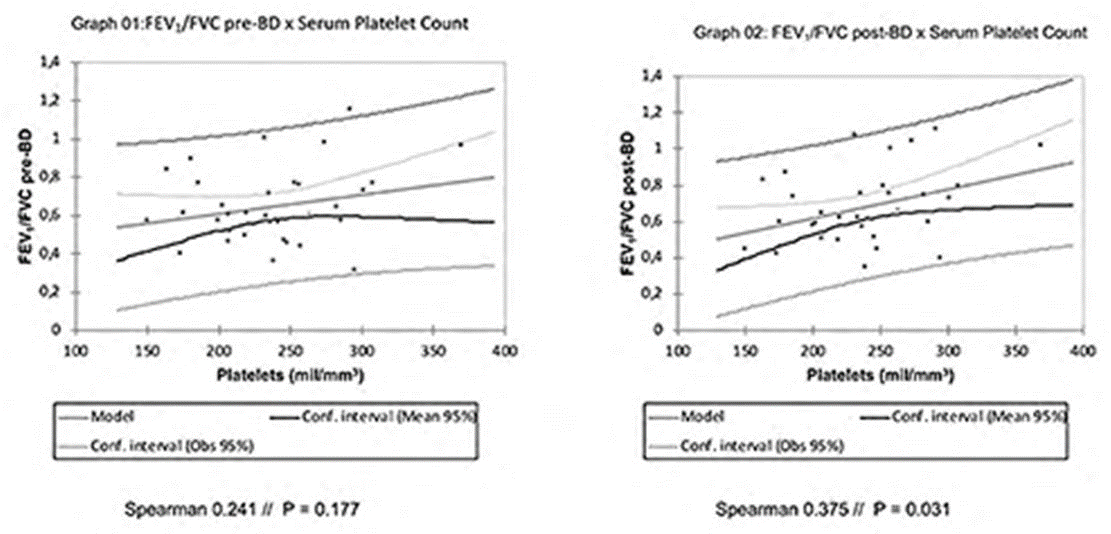
Primarily, FEV1/FVC pre- and post-BD values were correlated with serum platelet count and MPV. Variables were previously mathematically tested for normality by the Saphiro-Wilk test and graphically by plotting histograms. Then, correlation tests were selected depending on the characteristics of the variable: Pearson’s linear correlation was chosen for parametric variables and Spearman’s test for nonparametric variables, both represented in percentage values and linear regression graphs.
Subsequently, serum platelet count and MPV were correlated with SGRQ final score and also with the number of serious or very unpleasant respiratory events in the past three months. As the SGRQ final score resulted in a bimodal distribution, Spearman’s was the correlation test of choice to evaluate this nonparametric variable, and the graphical representation was performed in scatter plots. The same correlations were specifically done with the number of serious or very unpleasant respiratory events in the past three months. For the purposes of this analysis, this variable was understood not as a categorical variable, but as a discrete variable. This is because the relation between them is mathematically equivalent. Thus, it was decided to keep using Spearman’s test, given its greater suitability for discrete variables. Finally, the graphical representation was performed by box-plot graphs.
It is important to notice that platelet levels undergo significant variations with comorbidities, anthropometric and genetic characteristics. On the other hand, MPV appears to be less sensitive to these factors. Besides that, the small number of patients not only limits the ability to measure statistical significance, but can also cause accidental selection bias, since the study was performed with convenience sampling. Furthermore, the limited number of patients makes it difficult to perform multivariate techniques and more refined statistical modeling to assess nonlinear correlations and the import of other variables on the association. Finally, the methodology here implemented was chosen to better explore data, but correlation based approaches do not infer causality, so our results need to be interpreted in light of the previous literature.
A total of 38 patients were recruited and informed about the objectives of this study, as well as its risks, benefits and rights as volunteers. All of them agreed to participate and signed the Informed Consent Form. Of the 38 patients, eight brought blood count results without the MPV value, and five did not undergo spirometry. Population demographics are exposed in Table 1.
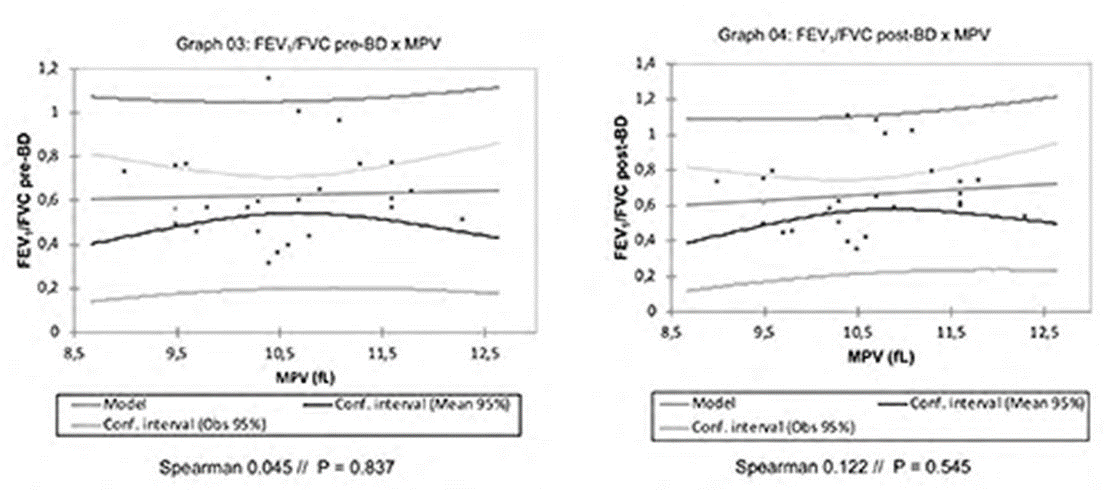
The correlation between serum platelet count and FEV1/FVC post-BD (graph 2) was statistically significant (p = 0.031), with effect size of 37.55%. However, the same was not observed in the correlation between serum platelet count and FEV1/FVC pre-BD (graph1), which resulted in 24.1% (p = 0.117). The correlations between MPV and Tiffeneau index pre- and post-BD (graphs 3 and 4) resulted in 4.5% (p = 0.837) and 12.24% (p = 0.545), respectively.
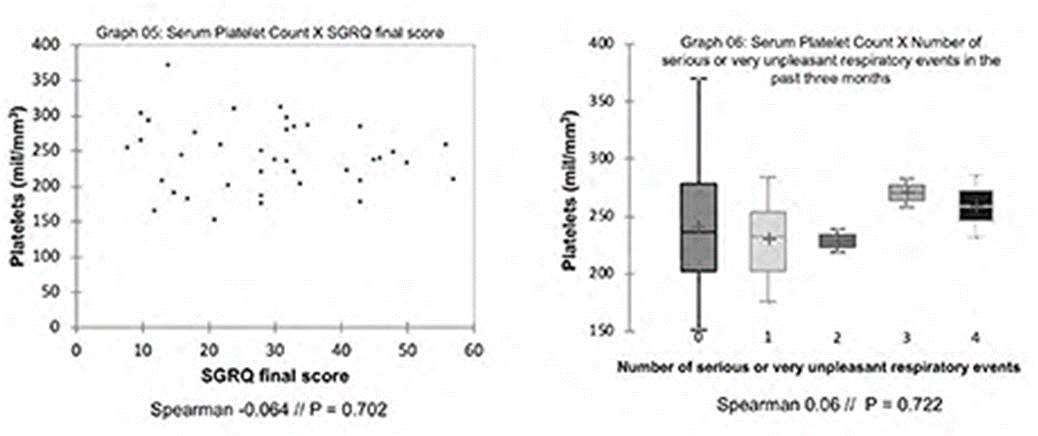
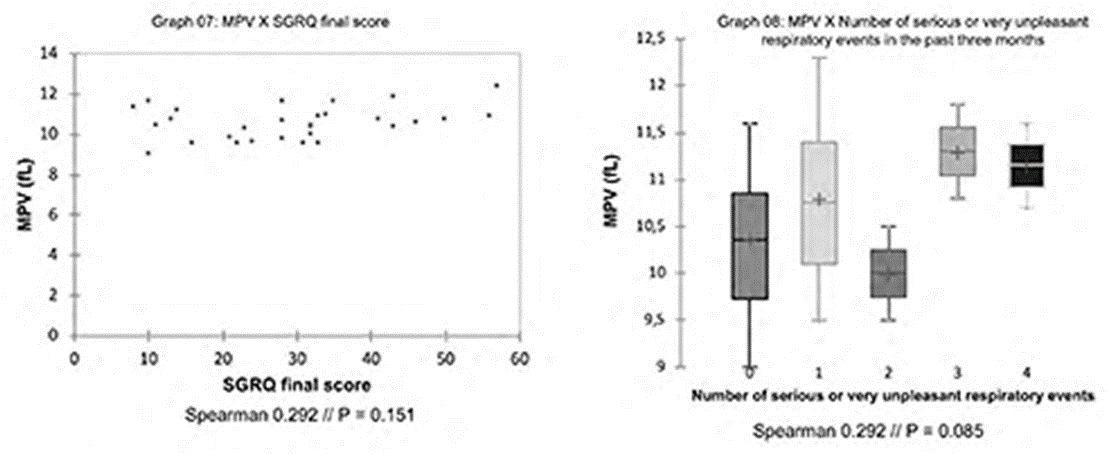
From Spearman’s test result, the correlation between SGQR total score and serum platelet count (graph 5) presented coefficient of -0.064 (p = 0.7), and between SGQR total score and MPV (graph 7) presented coefficient of 0.292 (p = 0.15). Moreover, the correlation between the number of serious or very unpleasant respiratory events in the past three months and serum platelet count (graph6) presented a coefficient of 0.06 (p = 0.722). Lastly, the correlation between the number of serious or very unpleasant respiratory events in the past three months and MPV (graph 8) presented a coefficient value of 0.292 (p = 0.085).
From the cross-sectional analysis of data, it was found a moderate correlation between serum platelet count and post-BD Tiffeneau index. This suggests that an increased number of platelets was shown in patients with higher FEV1/FVC post-BD. In addition, there was an association tendency between increased number of severe or unpleasant respiratory events, in the last three months, measured by SGRQ, and higher values of MPV, resembling a logarithmic curve association trend.
Systemic inflammatory process, inherent to COPD, promotes pro-inflammatory cytokines production, mainly Interleukin 6 (IL-6) [13,14]. It’s up-regulation has an important influence on megakaryocytosis, as IL-6 plays as a relevant stimulus on thrombopoietin production, leading to the production of a larger number of platelets [13]. This cytokine also favors an increase in the ploidy of megakaryocytic nuclei and an increase in platelets’ cytoplasm volume [13].
In face of a pro-inflammatory condition, there is also an increase in MPV due to the intense stimulus to intracellular synthesis of coagulation factors, cytokines, and degranulation of granules [13]. Therefore, MPV must be considered a platelet activation marker, suggesting that, in COPD patients, circulating platelets are more active and also have greater thrombotic potential [15]. Effectively, in a prior study conducted by Cui H. et al., MPV was higher in male and elderly COPD patients compared to controls, and it was even higher in those with more severe degrees of bronchial obstruction, verified by lower FEV1 values. Thus, it suggested that MPV can be used as an early marker of pulmonary severity in this group of patients [16].
Evidence points to a possible utility in using platelet levels as markers of clinical interest in COPD and also potentially guiding therapeutic approaches [4,5]. Harrison M. et al demonstrated higher rates of mortality in COPD patients with thrombocytosis after the first exacerbation episode, and also evidenced an improvement of this trend with the use of anti-aggregation drugs [5]. In agreement with this, in the present study, the SGRQ application showed a trend towards a greater number of exacerbations, therefore, greater disease severity and impact on quality of life, with higher MVP values. This may be a reflection of the association between increased platelet parameters and higher degrees of respiratory severity.
It is important to notice that MPV is related not only to the same stimulus that leads to thrombocytosis, but also to degranulation, coagulation and platelet hyperactivity. That said, MPV can be considered a more sensible parameter than serum platelet count in the context of COPD. This may explain its better correlation with the number of exacerbations, potentially preceding spirometric changes.
Finally, as seen in this study, patients with higher platelet count may respond better to the bronchodilator effect. In face of an increased number of platelets, it can be assumed that, in these cases, disease’s pathophysiology may have a greater inflammatory background, which consequently leads to a more intense stimulation to platelets’ production. Besides that, the inflammatory environment results in greater smooth muscle constriction in the lungs, thus being more sensitive to the bronchodilator effect.
Based on our results, we can infer that COPD, likely by means of the inflammatory pathways involved, may impact platelet counts and MPV values. That seems to be especially true for patients with better response to bronchodilators, which favors the hypothesis of inflammatory involvement. In this way, this study aims to discuss the trends observed and to expose our understanding of them, guiding further studies on the field.
This paper and the research behind it would not have been possible without the exceptional support from all employees who work in the ABC Medical School Pulmonary Rehabilitation Outpatient Clinic.

![]()

    |
Male |
21 (55,26%) |
Female |
17 (44,73%) |
Age (average - years) |
68,3 (58 – 86) |
Smokers |
2 (5,25%) |
Ex-Smokers |
34 (89,47%) |
Non-Smokers |
2 (5,25%) |
Cigarettes Smoked (average - packs. year) |
51,5 (12 - 150) |
SGRQ Total Score (average - points) |
29,1 (8 – 57) |
Platelet count (average – mm3) |
240,4 x 103 (151 – 370 x 103) |
MPV (average – fL) |
10,3 (9,0 – 11,8) |




































