Open Access
Research Article
Max Screen
ISSN: 2456-5482
Copyright: © 2024 Gabriela Ocampo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
To determine if a video physical exam clip of patients with acute bronchiolitis on high flow nasal cannula (HFNC) altered the duration of time from handoff initiation to either acceptance or refusal of the patient from the emergency department (ED) to the inpatient (IP) general pediatric wards.
Study Design:This was a randomized controlled study conducted at a tertiary care children’s ED. Patients with bronchiolitis requiring HFNC and admission to the hospital were randomized to either video physical exam handoff or verbal handoff via telephone call alone. The primary outcome was length of time between handoff initiation and patient acceptance or refusal by the IP team. Secondary outcomes included clinician handoff satisfaction scores and general safety comparisons.
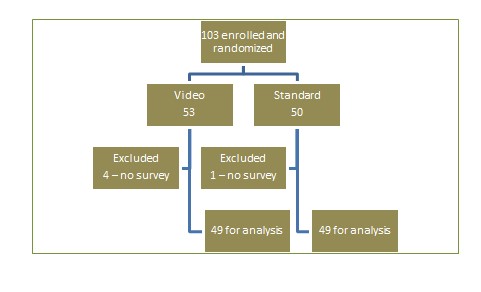
Results:Of the 103 children enrolled, 53 (51%) were assigned to video physical exam handoff and 50 (49%) assigned to verbal handoff alone. There was no significant difference regarding length of time between ED handoff initiation and IP acceptance or refusal of admission between the video and verbal groups (10.71 minutes vs 9.18 minutes, p=0.517, CI -0.619-3.3).Satisfaction survey response rate was 95% for ED clinicians and 75% for IP clinicians. There was no significant difference in satisfaction scores between the two groups (p=0.825). Safety events were low in both groups: p=0.543 (CI: -0.050 to 0.095) though our data suggests the use of video may address safety concerns earlier.
Conclusions:The addition of a video physical exam clip did not significantly alter the duration of time between ED handoff initiation and acceptance/refusal of the patient by the admitting IP service. Satisfaction scores were comparable among the two groups. To our knowledge, this is the first study to evaluate the use of virtual technology during ED-IP handoff. Future studies may be considered as electronic health records video technologies become more widely available.
Keywords: bronchiolitis; HHFNC; heated high flow nasal cannula; hospitalist; admission; handoff
Abbreviations:HFNC: high flow nasal cannula; ED: emergency department; IP: inpatient
Bronchiolitis is a leading cause of pediatric hospital admission in the United States, with an estimated 2 -3% of all US children requiring hospitalization for bronchiolitis during their first year of life [1, 2] Bronchiolitis is a lower respiratory infection and is most often caused by a virus, respiratory syncytial virus (RSV) being a common culprit [3,4]. Mild infections can present with nasal congestion and fever but progression into the bronchioles can lead to airway edema, coughing, tachypnea, retractions, wheezing, hypoxia, and even apnea in young infants [5]. Care of children with bronchiolitis is generally supportive and includes adequate hydration, suctioning of nasal secretions, and supplemental oxygen therapy.
High flow nasal cannula (HFNC) is thought to be more beneficial in acute bronchiolitis as compared to standard nasal cannula for several reasons: less damage to nasal mucosa and improved mucociliary function [6], decreased dead space and improved ventilation [7, 8] more precise delivery of FiO [2, 9] decreased atelectasis and improved lung recruitment through low-medium continuous positive airway pressure, [10-12] and overall more tolerable in infants and children compared to traditional CPAP [6, 12]. However, robust randomized controlled trials utilizing HFNC compared to other respiratory support modalities in bronchiolitis is limited, making it difficult to propose a uniform policy on HFNC administration and titration.
Predicting risk factors associated with more severe disease has proved challenging in patients with bronchiolitis [2-4]. This can present a dilemma for clinicians when deciding the appropriate unit for patient admission and management. Currently there is no consensus regarding initiation or titration of HFNC for children with bronchiolitis. HFNC use outside of the intensive care unit (ICU) is variable from institution to institution, with some pediatric wards placing limits on flow rates and others restricting its use altogether.
Patients diagnosed with bronchiolitis who are admitted to the IP unit from the ED present a challenge during verbal only handoffs as the description of a patient’s respiratory exam is largely subjective. While respiratory rate and oxygen saturation are objective, descriptions of a patient’s work of breathing, presence of retractions, and general description of a patient’s respiratory effort can be dependent on a provider’s level of training. These limitations in the handoff process can make it difficult for the IP team to assess the suitability of a given patient to a general floor versus an escalation of care (to either step-down unit or intensive care unit). Together, these factors can prolong the ED length of stay and delay inpatient admission. Studies in the adult population have shown that there is significant increase in mortality [13] and total length of admission and cost [14] associated with increasing ED length of stay. While similar studies have not been completed in the pediatric population, there is the possibility of similar outcomes and there should be cooperation between the inpatient and ED teams to facilitate the admission process. Methods to improve handoff continue to be studied to provide safe and quality care to patients [15, 16].
We propose the addition of a video physical exam clip during patient handoff to provide an additional objective component of the patient’s respiratory status. This video will allow the inpatient team to assess the patient without relying solely on verbal descriptions or documented vitals. In turn, this may prevent unnecessary trips to the ED from IP providers to assess patients and allow them to continue bedside care for other children on their service. We hypothesize this will lead to faster acceptance time by the inpatient team thereby reducing length of stay in the ED. Furthermore, we believe the addition of a video physical exam will improve the overall handoff experience and increase provider satisfaction. To our knowledge, there have been no previous studies describing video physical exam to enhance patient handoff. Our primary objective is to observe length of time between handoff initiation and patient acceptance or refusal by the IP team. Our secondary outcomes include clinician handoff satisfaction scores and general safety comparisons.
We conducted a randomized, controlled trial comparing video physical exam handoff and verbal only handoff between November 2020 to August 2021 at a tertiary pediatric ED with over 130,000 visits annually. The study was approved by the local institutional review board. Verbal permission was obtained from the parent or guardian of patients randomized to the video physical exam group.
Potential study subjects were identified if they were at least 14 days of age and under 3 years, diagnosed with bronchiolitis, receiving HFNC therapy, and had an admission bed request to the general pediatric ward service. Subjects were enrolled by convenience sampling secondary to whether or not providers had access to the EPIC video recording software and were able to complete the pre- and post- surveys (which may have been limited secondary to shift-shift handoffs prior to admission). We have rotating providers from outside institutions in all areas of the emergency room which minimized bias for selecting patients for groups based on which pod they were triaged to as they may or may not have the necessary recording software. Subjects were excluded for the following reasons: history of prematurity < 29 weeks, cyanotic heart disease or congestive heart failure, pulmonary hypertension, had a home oxygen or non-invasive ventilation need, if a tracheostomy was present, had a diagnosis of neuromuscular disease, or, if a PICU admission was deemed necessary. At our institution at the time of the study, PICU admission was required for any HFNC use of 6L or greater for patients under 3 years of age and any FiO2 greater than 50%.
Patients were assigned to either the video physical exam handoff ( “Video Handoff”) group or verbal handoff only (“Verbal Handoff”) group utilizing a blocked randomization method with randomly selected block sizes of 4, 8, and 12 to minimize bias (Figure 1). Sealed and numbered envelopes were placed in sequential order in a file located in the ED. The ED clinician selected the next sequential envelope (i.e. the next most front packet) and assured the patient met all inclusion and exclusion requirements. At this time, the envelope was opened to reveal which group the patient had been randomized to and to obtain the enclosed study materials.
We utilized video capturing technology available from our electronic medical record (EMR). Epic Haiku is an application that allows authorized users to securely record videos from a personal mobile device. These videos are automatically time stamped and saved to the patient’s chart as part of their medical record (Software). Videos do not save to the recording device, thus complying with Health Insurance Portability and Accountability Act (HIPAA) regulations for patient safety and privacy. Additionally, Epic Haiku is an institutionally approved platform to capture clinical information and requires only verbal permission from the patient or the patient’s guardian for its use. Users of Epic Haiku in our facility must be credentialed to practice at Children’s Medical Center Dallas, and they must also have an active network login. Epic Haiku is available for download on both iPhone and Android devices, however only iPhone devices were able to capture video recordings.
Standardized video requirements included a length between 20-30 seconds; frontal view of the patient’s face, chest, and abdomen; and the video must have been obtained within 60 minutes of patient handoff. Training was provided to ED clinicians during departmental meetings, posted flyers, and in person. ED fellows were available on shift to provide any additional support.
Our institution’s EPIC allows for clinicians to document specific time points for communication with the IP team through the “ED Pt Care Timeline”. When the ED provider calls the IP team, they can document that handoff has been completed. When the patient is ready to go to the IP unit, they are marked ready for transport by the attending physician, which is also documented in the timeline. Other time markers that the timeline notes are ED arrival time, ED rooming time, time IP bed request placed, time IP bed assigned, and time IP bed ready for patient (can be delayed due to having wrong bed for patient age or not being clean yet). Once handoff was completed, ED clinicians were asked to complete a satisfaction survey which included demographic information of the person completing the form (specialty, role, number of years at current role, gender) and questions related to their handoff experience. Handoff satisfaction questions were asked using a 5-point Likert scale (strongly agree, agree, neutral, disagree, or strongly disagree). Completion of this survey implied consent to participate in this aspect of the study. The ED clinician then used Epic’s secure chat feature to send an electronic REDCap satisfaction survey link to the IP clinician taking handoff.
In addition to information obtained from the ED handoff form and satisfaction questionnaires, the patient’s EMR was later reviewed to collect demographic information, details of medical management through hospital admission, and to identify any escalations in care, including rapid response code events, within 12 hours of admission to the general pediatric floor.
Patient demographics were compared using student’s t-test. A two-sample t-test was used to compare the duration of time between ED handoff initiation and either acceptance or refusal of the patient to the general pediatric inpatient service (aka “Duration") between the Video and Verbal handoff groups. It was also used to compare the average total satisfaction scores of clinicians participating in either Video or Verbal handoff.
Of the 103 patients that were enrolled in our study, 53 patients were assigned to the Video group and 50 patients were assigned to the Verbal handoff group. There was no statistical difference of in age when comparing the 2 groups. Average age in months of participants were 8.5 in video group and 11.2 in verbal only group: p=0.560. Of the various demographics, only gender approached clinical significance with a p-value of 0.057 (CI: -5.4681 to 0.0820) [Table 1].
The satisfaction survey response rate was 95% for ED clinicians and 75% for IP clinicians. Overall, satisfaction scores were similar between the two groups (p=0.825). while not statistically different, satisfaction trended higher among the ED clinicians.
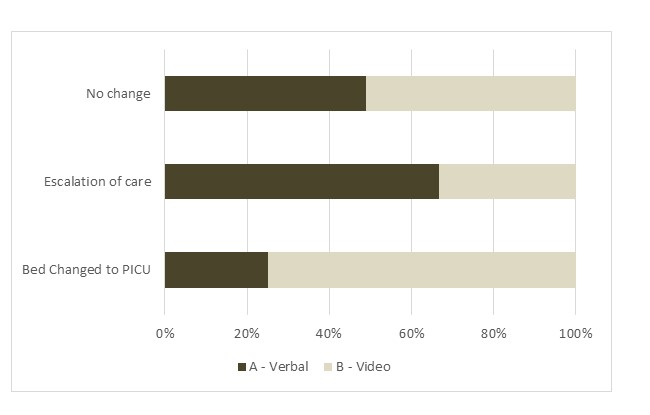
Safety events were low in both groups. A total of 4 patients, 1 in the Video group and 3 in the Verbal group, required transfer to the pediatric intensive care unit within 12 hours of admission (Figure 2). Of these patients, 3 had METs called (medical emergency team) and 1 had a controlled transfer to the PICU. We also noted that 3 patients in the Video group had their ED admission order changed from the general inpatient ward to the intensive care unit versus only 1 patient in the Verbal group. Of these patients, 2 were in the video group and had initiated handoff to the IP general pediatrics team prior to changing admission bed request to the intensive care unit. The additional patient in the video group had initially had a PICU bed request placed but was weaned on HFNC and changed to a general pediatrics bed when they met floor criteria. The 1 patient that had their bed request changed occurred prior to any handoff with the IP team being initiated. There was no significant difference between the video and verbal only handoff groups (p=0.543, CI: -0.050 to 0.095).
Admissions for acute bronchiolitis from the emergency department to the IP unit will continue to pose a challenge for providers until a more uniform way of communicating the respiratory exam is agreed upon. Recognizing a patient’s perceived respiratory effort, and therefore severity of illness, requires experience and knowledge that varies among the different levels of providers in any emergency department and IP unit, especially at a large academic center. Introducing more objective evaluations to the handoff process is vital to optimize communication between different units and ultimately have a more efficient admission process. While our study did not show significant difference in length of time to admission/refusal of patients, it did show high provider satisfaction with video handoffs.
During the COVID-19 pandemic, the United States saw a marked drop in patients seeking medical treatment for acute bronchiolitis during the 2020-2021 season, the same time as enrollment for our study [17]. The decreased total patient volumes may have had some impact on pressures to handoff quickly or overall sense of patient safety than if it had happened during a normal respiratory season. Additionally, there may have been parental pressure to want to avoid the ED until the patient was sicker as to limit exposures to COVID-19, possibly leading to more acute presentations. Further, the COVID-19 pandemic led to decreased exposures among children who were staying away from daycare settings and may have had heightened immune responses due to lack of previous exposure. We also noted fewer inpatient clinicians presenting to the ED to evaluate patients prior to handoff initiation for admission as compared to previous years. This decrease in “in person” evaluations may have been attributed to COVID-19 concerns but it cannot be determined how much this impacted ED length of stay compared to previous years. Additionally, there are other things that can contribute to increased ED length of stay such as nurse handoffs, appropriate room equipment ready (patient beds vs cribs, etc), and transport availability.
Survey response rate was excellent among ED clinicians; however, it was lower for IP clinicians and may represent a response bias. Another ED handoff study [20] showed the opposite trend with a response rate of 50% for ED physicians compared to 66% for IP physicians. While our sample was much smaller than that study (105 patients compared to 2800 in this study), our overall response rate was much higher from both groups. This may have been from specific workflow and reminders in the ED as well as follow up EPIC messages to IP providers immediately after handoff that allowed this. A previous study of handoff quality [19] showed an increase in overall staff satisfaction from 55% to 70%. This was a larger study done across 23 institutions and a variety of handoff settings (shift to shift, ED to IP, periop to IP, IP to IP, and IP to radiology) but shows that further changes to provider handoffs is generally well accepted.
Finally, this was a single-center study and at the time of the study our institution limited HFNC flow rates to a total of 6 liters flow for patients under the age of 3 years (2 years and under) regardless of weight. These are facility specific restrictions and may have created longer ED length of stays as patients required PICU admission whereas at another facility they may have been appropriate for a general inpatient bed. This also may have impacted IP providers perceived comfort with admitting patients to the floor that were at borderline respiratory settings as well as affecting the rate at which patient’s needed to escalate care to the PICU based on these floor maximum settings.
Safety events were overall low. Of the 4 patients requiring transfer to the ICU within 12 hours of admission, all but 1 remained on HFNC. One patient was briefly placed on CPAP and subsequently weaned back to HFNC the following day. We did find it interesting that 3 patients in the Video handoff group had their admission bed order changed to the ICU, versus only 1 patient in the Verbal group. While not statistically significant, this may suggest that video physical exam may be useful in detecting sicker patients compared to verbal descriptions of respiratory exams. While our research was limited to only patients within our facility, future projects could examine the utility of video physical exams in handoffs from outside facilities (either other ED to ED admissions or direct to floor admissions).
Our study is the first of its kind utilizing video technology to capture a patient’s physical exam and use it during ED handoff to the IP service. Research has been focused on optimizing overall handoffs by using specific transfer of care interventions and training for clinical staff. A study of 23 children’s hospitals [19] showed that evidence based recommendations regarding handoff intent and content, standardized tools/methods, and clear transition of responsibilities shows decrease in adverse events. Our study focuses on a specific portion of the ED to IP handoff involving the communication of the patient’s exam and their clinical severity. Further work can be done to combine the video exam with these standardized handoff methods in future research endeavors. Especially in patient populations that have some work of breathing at baseline (those with prematurity, bronchopulmonary dysplasia, trach/vent dependence), having a video physical exam when well could help emergency providers to distinguish an acute escalation in effort.
There could be further utility in repeating this study now that bronchiolitis visits are now back to previous (and sometimes even higher) rates than before the pandemic. As the video physical exam did not show any negative effect on patient satisfaction, further research can also explore further ways to implement video exams for optimizing admission handoffs. Further, the video physical exam could provide information into how the patient responds to interventions such as suctioning, initiation of high flow, or use of bronchodilators which could be available for the team to review if the patient worsens once admitted.

![]()

 |
| Figure 1: Study schematic |
 |
| Figure 2: Outcome of Care |
|
Video Exam Handoff |
Verbal Handoff |
p-value |
Age (months) |
8.541 ±5.850 |
11.234 ±7.537 |
0.560 |
Sex |
|
|
0.057 |
Male |
18 |
20 |
|
Female |
30 |
26 |
|
Ethnicity |
|
|
0.415 |
Hispanic or Latino |
22 |
25 |
|
Non-Hispanic or Latino |
26 |
21 |
|
Race |
|
|
0.0676 |
White |
20 |
25 |
|
Black |
15 |
10 |
|
Not Answered |
12 |
9 |
|
American Indian/Alaska Native |
0 |
1 |
|
Asian |
0 |
1 |
|
Hawaiian or Pacific Islander |
1 |
0 |
|
|
Video Exam Handoff (n=52) |
Verbal Handoff (n=50) |
p-value |
Handoff “Duration” (Minutes, Mean, SD) |
10.71 ±11.87 |
9.18 ± 11.86 |
0.517 |
Bed admission changed to ICU |
3 |
1 |
0.323 |
ICU transfer within 12 hours of admission |
1 |
2 |
0.543 |
Satisfaction with hand-off (%) |
89.8 |
91.2 |
0.825 (Fisher’s exact test) |




































