Open Access
Research Article
Max Screen
ISSN: 2456-5482
Copyright: © 2023 Chaimae El Mahdaoui. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Acute lymphoblastic leukemia (ALL) is considered as the most common pediatric malignancy with 80% of frequency in children between 1 and 10 years old. With the evolution of science, improved diagnosis and adapted treatment, all survival rates increased to a possibility of 80%.
Philadelphia chromosome like acute lymphoblastic leukemia (Ph-Like ALL) is a recent genetic discovery characterized by a gene expression profile and high frequency of IKZF1 gene alteration similar to that of BCR-ABL1 positive ALL with a poor outcome. We can identify it in 10% to 15% in children, 20% in adolescents (between 16 - 20 years old) and young adults. It has been reported that ALL Ph like is known with a high frequency in relapse. Yet, adapted treatment with ITK can improve prognosis of patients with this abnormality.
The standard diagnostic B-All panel includes testing for abnormalities using cytogenetic techniques such as karyotype and FISH completed by molecular techniques if needed to explore cryptic abnormalities.
Before testing the Philadelphia like B-ALL, some abnormalities need to be excluded such as hyperdiploidy, BCR- ABL1, ETV6-RUNX1, MLL.
6 subtypes of ALL Ph like were identified so far
Keywords: Acute lymphoblastic leukemia; cytogenetic; Ph-Like; B-ALL
Novel subtypes were identified in the past decade by advanced comprehensive genomic profiling studies. This allowed the identification of new treatment approaches, targeted chemotherapy and allowed the understanding of treatment failure in some ALL cases [1].
The Dutch Childhood Oncology Group (DCOG), Erasmus University, Rotterdam, made a major discovery in 2009 of a new subgroup of patients. Using Microarray gene expression analysis, a molecular signature similar to ALL Ph Positive showed in a group of 107 patients that 15% to 20% are expressing the same profile but lacks the BCR-ABL1 gene fusion translocation [2] and characterized by additional kinase-activating alterations.
The hallmark of ALL are chromosomal alterations and include aneuploidy (hyperdiploidy and hypodiploidy) and recurring chromosomal translocations such as t(12;21) (ETV6-RUNX1), t(1;19) (TCF3-PBX1), t(9;22) (BCR-ABL1) and rearrangement of MLL [3]. Research has shown that several subgroups of childhood acute lymphoblastic leukemia ( ALL) have unfavorable prognosis. For example, T-lineage ALL (about 15% of all cases) and the precursor B-lineage subtypes with chromosomal translocations creating MLL-rearrangements or the BCR–ABL1 gene fusion, each found in less than 5% of cases [4]. On the other hand, there are favorable prognosis abnormalities in childhood ALL such as TEL-AML1 (ETV6-RUNX1) that is found in 20-25% of B-ALL patients, hyperdiploidy that is identified with >50 chromosomes and that is found in 25% of B-ALL cases and TCF3 (E2A)-rearranged ALL often E2A–PBX1-positive that is found in about 5% of cases. Unfortunately, about 25% of patients have an unclassified genetic profile (B-other) [5]. These discoveries allow treatment improvements to increase survival rate in ALL patients. Relapses are common in these patients, indicating the need for new biological exploration and treatment options for ALL [6].
The discovery of ALL ph like positives allowed the identification of a poor outcome abnormality and the prospect of Ph-like ALL biology provides an opportunity for adapted therapy.
Emerging targeted therapies hold great promise for advancing the treatment landscape of Philadelphia-Like Acute Lymphoblastic Leukemia (Ph-Like ALL). Ongoing research and clinical trials are exploring innovative approaches to specifically target the underlying genetic alterations in this subgroup. One notable development is the investigation of novel tyrosine kinase inhibitors (TKIs) with improved selectivity and potency against fusion kinases present in Ph-Like ALL [3].
Additionally, immune-based therapies, including chimeric antigen receptor (CAR) T-cell therapy and bispecific T-cell engagers (BiTEs), are being evaluated for their potential to harness the immune system in targeting leukemic cells [7]. Furthermore, agents targeting key signaling pathways implicated in Ph-Like ALL, such as the JAK-STAT pathway, are showing promise in preclinical studies [8].These emerging therapies represent a significant stride towards more effective and targeted treatment options for patients.
In addition to medical treatment, it is crucial for patients and families affected by Philadelphia-Like Acute Lymphoblastic Leukemia (Ph-Like ALL) to have access to a network of support and resources. Reputable organizations and support groups play a pivotal role in providing valuable information, emotional support, and practical assistance. The Leukemia & Lymphoma Society (LLS) and the American Cancer Society (ACS) are prominent organizations that offer a wide range of resources tailored to individuals facing ALL, including those with Ph-Like ALL. These organizations provide comprehensive educational materials, access to expert advice, and opportunities for patients and families to connect with others who share similar experiences [9,10].
Furthermore, local cancer centers and hospitals often have dedicated support teams and social workers who can help navigate available resources [11]. Engaging with such groups and organizations has been shown to significantly improve the well-being and overall quality of life for those affected by Ph-Like ALL [12].
The BCR-ABL Like B-lymphoblastic leukemia ( BCR-ABL1 like B-ALL) also known as Philadelphia-like (Ph-like) ALL, is characterized by rearrangements, sequence mutations and copy number alterations that activate tyrosine kinase or cytokine receptor signaling and are potentially amenable to therapeutic targeting with tyrosine kinase inhibitors.
The pattern of gene expression is similar to that of B-ALL with the BCR-ABL1 translocation but lacks the BCR-ABL1 fusion protein and is characterized with a high rate of relapse and poor outcome [13].
This new entity gene expression profile is known by the activation of the ABL class or JAK/STAT signaling pathways associated by kinase-activating gene rearrangements.
Many genes are involved in this process including ABL1,ABL2, CRLF2, JAK2, EPOR, NTRK3, CSF1R and PDGFRβ or by activating gene mutations involving genes including JAK1/2/3, FLT3, IL7R, and SH2B3 [14].
Ras pathway activating mutations are also common, as are mutations to the IKZF1 (IKAROS) gene [14].
BCR-ABL1 Like B-ALL has been added to the World Health Organization update in 2016 as a provisional entity [15].
Patients with Ph-like ALL are generally presented at diagnosis with an initial leukocyte count superior to 100 000/uL. Compared with patients with non Ph like ALL, they often display an elevated minimal residual disease at the end of induction therapy [13]. One of the common cases that justifies induction failures in patients with Ph-like ALL is associated with EBF1-PDGFRB gene fusion [16]
Some of the tyrosine kinase genes activation process is illustrated in Figure 1 [17]
Epidemiologic evaluation constitutes a powerful screen for assessment of patients with high likelihood for the BCR-ABL1-like gene expression phenotype.
The frequency of BCR-ABL1 Like gene expression profile is 15-20% in ALL patients according to different cohorts. It is classified in the high risk group of B-ALL with high-risk features in children as well as new diagnosis B-ALL in adolescents and adults and requires intensive and specific therapy [18- 19].
An interesting study showed that down syndrome patients have high rates of CRLF2 translocations, often associated with activating JAK mutations [20].
Studies have exposed that young adults patients with Ph-like ALL have the worst prognosis compared with children and adolescents (Figure 2).
CRLF2 rearrangement is a frequent genetic alteration observed in children and young adults with Ph-like ALL. The CRLF2 gene, located on chromosome Xp22.33, encodes the cytokine receptor-like factor 2. Dysregulation of CRLF2 expression and signaling due to rearrangements contributes to leukemogenesis and altered disease biology in Ph-like ALL. The most common CRLF2 rearrangement identified in ALL involves the translocation of the CRLF2 gene with the immunoglobulin heavy chain gene (IGH@), resulting in the formation of the CRLF2-IGH fusion gene. This fusion leads to overexpression of CRLF2 and constitutive activation of downstream signaling pathways, including JAK-STAT signaling [20-23].
The CRLF2-IGH fusion has been associated with a higher risk of relapse and poor prognosis in pediatric B-cell precursor ALL [23].
ABL-class gene rearrangements are frequently observed in children with Ph-like ALL. These rearrangements involve fusion of the ABL-class genes (such as ABL1, ABL2, and CSF1R) with various partner genes, resulting in the formation of chimeric fusion proteins. ABL-class rearrangements activate tyrosine kinase signaling pathways, including the ABL and JAK-STAT pathways, and contribute to leukemogenesis [24]. The identification of specific ABL-class rearrangements, such as ABL1 fusions with diverse partner genes, highlights the molecular heterogeneity within Ph-like ALL and may have implications for disease prognosis and targeted therapy approaches [24].
In young adults with Ph-like ALL, there is a striking increase in the frequency of JAK2 rearrangements. JAK2 rearrangements involve fusion of the JAK2 gene with various partner genes, leading to constitutive activation of JAK-STAT signaling pathway. This aberrant signaling contributes to leukemogenesis and altered disease biology in Ph-like ALL [25]. The identification of JAK2 rearrangements in young adults has implications for risk stratification and targeted therapy approaches, as JAK inhibitors have shown promise in preclinical studies targeting JAK-STAT signaling in Ph-like ALL [26].
EPOR rearrangements are another subgroup of genetic alterations observed in Ph-like ALL. These rearrangements involve fusion of the EPOR gene with partner genes, resulting in dysregulated EPOR signaling. EPOR rearrangements contribute to leukemogenesis and have implications for disease biology in Ph-like ALL. The specific partner genes involved in EPOR rearrangements and their functional consequences are areas of ongoing research [27].
It is important to note that the understanding of rearrangements and mutations in Ph-like ALL is continuously evolving, and ongoing research is aimed at uncovering additional genetic alterations and their functional implications. These discoveries hold promise for developing targeted therapies and improving treatment outcomes for children and young adults with Ph-like ALL.
Fluorescence In Situ Hybridization (FISH) is a widely used technique for detecting chromosomal rearrangements in ALL, including Ph-like ALL, in children and young adults. FISH utilizes fluorescently labeled DNA probes that target specific genomic regions of interest. It allows for the visualization of fusion events involving genes such as CRLF2 and other relevant fusion partners. FISH provides valuable information about the presence and frequency of specific rearrangements in leukemic cells [28].
Reverse Transcription Polymerase Chain Reaction (RT-PCR) is a molecular technique commonly employed to detect fusion transcripts resulting from chromosomal rearrangements in ALL Ph-like cases. RT-PCR involves the conversion of RNA into complementary DNA (cDNA) using reverse transcriptase enzyme, followed by amplification of the target fusion transcript. It enables the sensitive and specific identification of fusion genes, such as CRLF2-IGH, which is prevalent in Ph-like ALL. RT-PCR aids in the diagnosis and risk stratification of pediatric and young adult ALL patients [29].
Next-Generation Sequencing (NGS) technologies have revolutionized the detection of genetic alterations in ALL Ph-like cases in children and young adults. NGS allows for the comprehensive analysis of the genomic landscape, including gene fusions, point mutations, and structural variations. Whole-genome sequencing, whole-exome sequencing, or targeted sequencing approaches can identify specific genetic alterations associated with Ph-like ALL. NGS provides high-resolution information, aiding in risk stratification, treatment decision-making, and the development of targeted therapies [30].
Multiplex Ligation-dependent Probe Amplification (MLPA) is a technique used to detect copy number alterations, including deletions and duplications, in target genes relevant to Ph-like ALL. MLPA employs multiplex PCR amplification and hybridization with fluorescently labeled probes to assess the copy number status of specific genes. It helps identify genetic abnormalities, including deletions or duplications in genes such as CRLF2, JAK2, and other relevant loci. MLPA aids in the molecular characterization and risk stratification of pediatric and young adult ALL patients [31].
Conventional cytogenetic analysis, including karyotyping and chromosome banding techniques, remains an important tool for detecting chromosomal abnormalities in pediatric and young adult ALL cases, including Ph-like ALL. Cytogenetic analysis provides an overall view of the chromosomal changes and structural rearrangements in leukemic cells. It complements other targeted detection methods and aids in the diagnosis and risk stratification of ALL patients [32].
These detection techniques play a crucial role in identifying and characterizing the rearrangements and mutations associated with Ph-like ALL. Combining multiple methods allows for a comprehensive assessment of the genetic landscape, aiding in risk stratification, treatment decision-making, and the development of targeted therapies for patients with Ph-like ALL.
Intensive chemotherapy, tyrosine kinase inhibitors and hematopoietic stem cell transplantation are the standard therapy for acute lymphoblastic leukemia with Ph like but recently different targeted therapy are being explored to be induced in the treatment protocols.
JAK Inhibitors: CRLF2 rearrangements often involve dysregulation of the JAK-STAT signaling pathway. JAK inhibitors, such as ruxolitinib and momelotinib, have shown promising results in preclinical and early-phase clinical trials for patients with CRLF2- rearranged ALL [33].
Tyrosine Kinase Inhibitors (TKIs): ABL-class gene rearrangements, including ABL1, ABL2, and PDGFRB fusions, can be targeted with specific TKIs. For example, imatinib is effective against BCR-ABL1 fusion, while dasatinib and nilotinib have shown activity against various ABL-class fusions [34].
JAK Inhibitors: JAK2 rearrangements result in constitutive JAK-STAT pathway activation. JAK inhibitors, such as ruxolitinib and fedratinib, have demonstrated efficacy in targeting JAK2 rearrangements in preclinical studies and clinical trials for Ph-like ALL [21].
EPOR Antibodies and Small Molecule Inhibitors: EPOR rearrangements can lead to dysregulated erythropoietin receptor signaling. Monoclonal antibodies against EPOR or small molecule inhibitors targeting downstream signaling pathways are being investigated as potential targeted therapies for Ph-like ALL with EPOR rearrangements [27].
It is important to note that targeted therapies for specific rearrangements and mutations in Ph-like ALL are still under investigation and may be used in the context of clinical trials or off-label. Treatment decisions should be made in consultation with a specialized oncologist and based on the individual patient's characteristics, including the specific genetic alterations present in their leukemia cells.

![]()

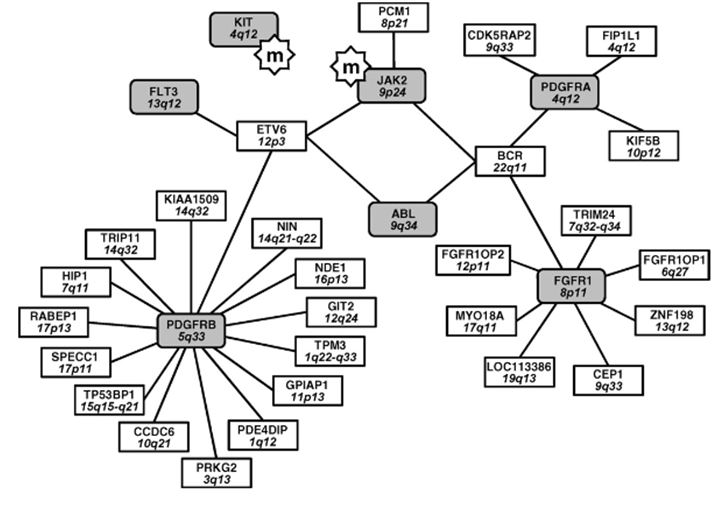 |
| Figure 1: Translocations involved in myeloproliferative syndromes. The tyrosine kinase genes are enriched and can be activated by different partners during chromosomal translocations, or be activated by point mutation (m) |
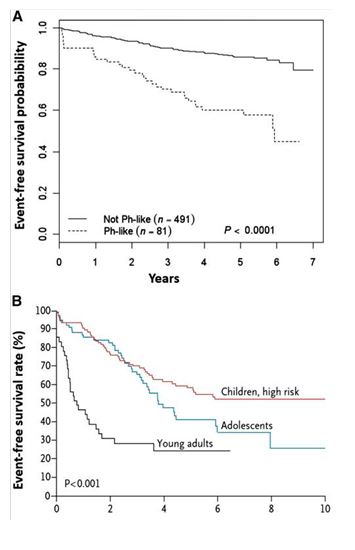 |
| Figure 2: Outcomes of children, adolescents, and young adults with Ph-like ALL. (A) Patients with Ph-like ALL have an inferior outcome compared with patients with non-Ph-like patients treated on AALL0232. (B) Among patients with Ph-like ALL, young adults have the worst prognosis compared with children and adolescents [21]. Adapted from Roberts et al [13] and Loh et al, [22]. |




































