Open Access
Research Article
Max Screen
ISSN: 2456-5482
Copyright: © 2021 Gu Q. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Laryngotracheal stenosis is one of the important causes of pediatric airway obstruction, and the etiology can be classified as congenital and acquired. With the widespread use of tracheal intubation and tracheotomy in pediatric emergency, iatrogenic laryngotracheal stenosis is gradually replacing trauma and infection as the major cause of acquired laryngotracheal stenosis [1]. Nowadays, open surgery is the first choice for severe laryngotracheal stenosis cases [1,2]. Here, we describe a case of childhood iatrogenic severe laryngotracheal stenosis, and the reflection on the current treatment methods of children with laryngotracheal stenosis.
Keywords: Laryngostenosis; Therapeutics; Pediatrics
A 18-month-old boy was admitted to the respiratory department of Children’s Hospital Capital Institute of Pediatrics on January 28, 2020, due to “fever and cough for 8 days”, with the diagnosis of “bronchopneumonia, urinary tract infection, abnormal renal function, and mild anemia”. On January 31, he was transferred to pediatric intensive care units due to dyspnea. At that time, he was diagnosed with “bacterial pneumonia, adenovirus infection, H1N1 influenza, pleural effusion, respiratory failure type I, hemophagocytic syndrome, hypoproteinemia, liver dysfunction, urinary tract infection, compensatory metabolic acidosis with respiratory alkalosis”. At the same day, tracheal intubation was applied to assist breathing. Fiberoptic bronchoscope were performed twice on February 4 and 7, laryngotracheal stenosis was not described at that time. The tracheal intubation was removed twice on February 13 and 16, but due to dyspnea and hypoxemia, the intubation was performed again 1 hour and 1.5 hours later respectively. On February 17, an otolaryngologist conducted a consultation, awake flexible fiberoptic laryngoscopy was performed, reported subglottic stenosis, surgical exploration and tracheotomy was recommended (Figure 1).
On February 18, tracheotomy and laryngotracheal exploration was performed under general anesthesia, a 4# tracheotomy tube was inserted. Laryngotracheal exploration was performed with self-retaining laryngoscope. The subglottic annular stenosis was observed, the percentage of obstruction was about 75%, leaving only a central orifice (Figure 2). Thereafter, budesonide q6h and 3% hypertonic saline q12h atomized inhalation were given.
On March 3, awake flexible fiberoptic laryngoscopy was performed again. The bilateral vocal cords had good movement and could be closed. The surface of the vocal cords was smooth, a little granulation tissue could be seen under the vocal process arytenoid cartilage, and the trachea lumen was unblocked (Figure 3). Trying to block the tracheostomy tube for 5 minutes, the child has no obvious gasping. The next day the child was discharged with a tube. On March 10, he was brought back to have the tracheostomy tube bremoved.
Laryngotracheal stenosis is one of the important causes of airway obstruction in pediatric population, etiologies can be divided into congenital and acquired [1]. With the widespread application of endotracheal intubation and tracheotomy in pediatric emergency, iatrogenic laryngotracheal stenosis gradually replaces trauma and infection and becomes the main cause of acquired laryngotracheal stenosis. Currently, open surgery is the treatment of choice for severe laryngotracheal stenosis cases [1,2], especially endoscopic therapy [3,4]. But is there a more minimally invasive approach? Here we describe a case of childhood iatrogenic severe laryngotracheal stenosis, and the reflection on the current treatment methods of children with laryngotracheal stenosis.
Tracheal intubation and tracheotomy in the pediatric population are basic skills to maintain the airway in emergency treatment, but subglottic and tracheal stenosis secondary to scar tissue also follows as a complication, which is iatrogenic laryngotracheal stenosis. It has been reported that 90% of acquired laryngotracheal stenosis is caused by tracheal intubation [5], especially for neonates [6]. Among them, children’s laryngotracheal stenosis is more difficult to be treated than adults due to their smaller laryngotracheal cavity, poor coordination and developing larynx and trachea.
Laryngotracheal stenosis related to tracheal intubation is mainly caused by acute intubation injury and airway compression of the cannula, prolonged intubation, and too much mandrel pressure are the risk factors for stenosis. In this case, the child received tracheal intubation for respiratory failure. Bronchoscopy did not find laryngotracheal stenosis 1-week post-intubation, and subglottic stenosis was found 2 weeks post-intubation due to intolerance of extubation. This history was typical iatrogenic laryngotracheal stenosis caused by prolonged tracheal intubation.
There are many treatments for laryngotracheal stenosis in children. Children with mild illness can be treated by mitomycin C, endoscopic balloon dilatation [1,7] and laser surgery [2,8], less injury and faster recovery, but with a certain recurrence rate, which requires repeated operations, but multiple operations may aggravate the scar, resulting in later treatment difficulties [2]. Most of the children with severe stenosis need to be treated with open surgery such as laryngotracheal resection, reconstruction [2,9] and Montgomery T-tube insertion [10]. However, the surgical injury is relatively large, especially for infants and young children. The operating space is rather small, and the larynx, trachea and other organs are not fully developed, therefore, minimally invasive treatment is more demanded. In this case, the percentage of subglottic obstruction was about 75%, which was grade III in Myer-Cotton grading system [11] and represented severe stenosis. Two weeks after tracheal intubation, tracheotomy was performed, the tube was removed, and strengthen atomization inhalation therapy was performed. The fiberoptic laryngoscopy was re-examined after two weeks, and most of the subglottic granulation was self-absorbed, thus avoiding the expected laryngotracheal reconstruction.
This case suggests: (1) Since children have a strong self-repair ability, there is no need to rush surgical treatment for iatrogenic laryngotracheal stenosis occurring within a short period. The surgical treatment mentioned here includes minimally invasive laser surgery, balloon dilatation, and open surgery, because any local treatment may cause secondary injury and aggravate the disease. (2) Wait-and-see therapy after removing the etiology may be a good idea, but the key details such as which patient is appropriate and how long to wait still need to be explored further. (3) Many doctors do not recommend tracheotomy, think of new injury for children with scar constitution, so hope to practice more minimally invasive treatment, such as early balloon dilatation. However, we believe that if tracheotomy is not performed, airflow turbulence will inevitably form in the subglottic narrow area during respiration, and violent gas shocks will interfere with the absorption of granulation tissue. Our case showed that timely tracheotomy can achieve a good prognosis.
Of course, only one patient is not of universal significance. However, this is an attempt of a new concept, and we will discuss more cases in the future.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Received special fund of the Pediatric Medical Coordinated Development Center of Beijing Municipal Administration of Hospitals, No. XTZD20180102.

![]()

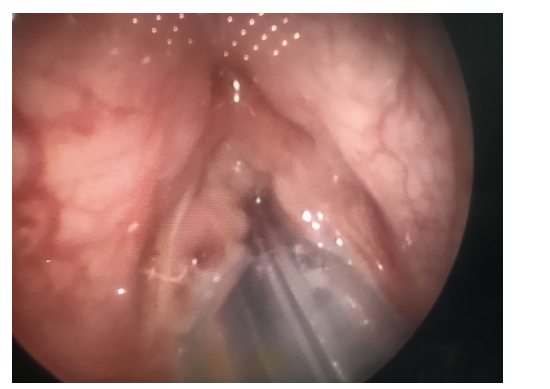 |
| Figure 1: Pre-tracheotomy endoscope image showing subglottic stenosis |
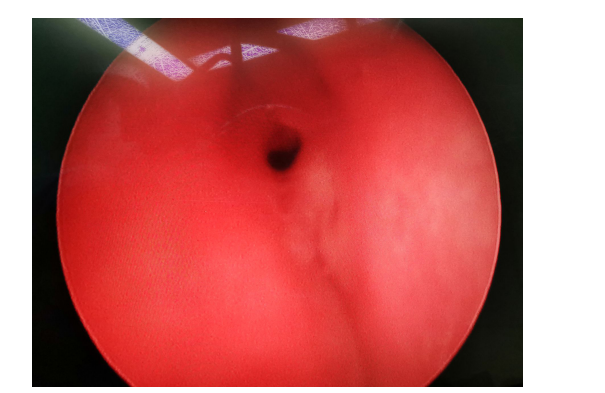 |
| Figure 2: Intraoperative endoscope image showing the percentage of obstruction was about 75%, leaving only a central orifice |
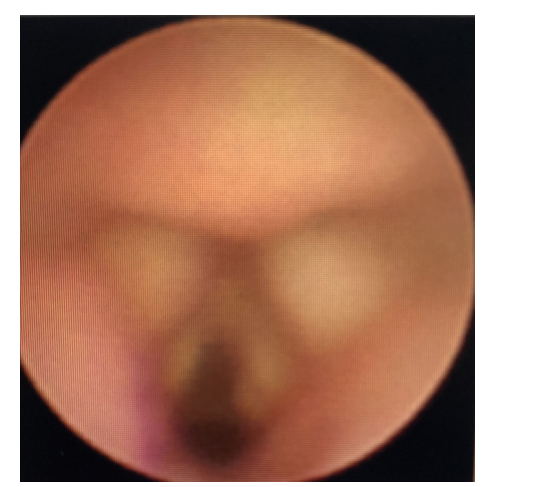 |
| Figure 3: 2-weeks-postoperative endoscope image showing the trachea lumen was unblocked, only a little granulation tissue could be seen under the vocal process arytenoid cartilage |




































