Open Access
Research Article
Max Screen
ISSN: 2456-5482
Copyright: © 2021 Tahhan N. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Neonatal management of severe quadricuspid truncal valve insufficiency is very challenging with high risk of postoperative mortality. Aortic valve reconstruction is the unique rescue and should be consider and previously planned in case of truncal valvuloplasty failure. Many extracardiac malformations can be associated to truncus arteriosus, therefore a cardiac and chest computed tomography scan must be performed before the elective surgical repair.
Learning objective:Anticipate comorbidities and consider truncal valve reconstruction is essential in complex neonatal truncus arteriosus repair.
Keywords:Neonatal Truncus Arteriosus; Quadricuspid Valve; Truncal Valve Regurgitation; Neonatal Ozaki Procedure; Extrinsic Airway Compression
Truncus arteriosus (TA) accounts for 0.7–3% of congenital cardiac defects [1]. Severe truncal valve (TV) insufficiency (TVI) has been reported as one of the most important factors influencing mortality, it is estimated to occur in 25–50% of patients with truncus arteriosus [2].
Therefore, surgical management of moderate or severe TVI is challenging, especially in the neonatal period. However, there is no standard surgical approach to TVI. Associated lesions such as interrupted aortic arch (IAA), truncal valve insufficiency (TVI), and coronary artery anomalies remain major risk factors for short-term and long-term survival. Also, External airway compression by a dilated ascending aorta, other than vascular rings, can cause significant morbidity in patients with TA [3].
A one–month-old term boy, weighing 3 kg, was referred to our institution with the diagnosis of truncus arteriosus.
Echocardiography revealed a TA type 1-2 according to Van Praagh classification [4]; two symmetric ventricles, large outlet VSD, large truncus arteriosus, right aortic arch, 2 good sized pulmonary arteries and quadricuspid truncal valve with severe insufficiency and moderate stenosis.
An elective primary surgical repair according to Rastelli Procedure was performed; VSD closure, right ventricle (RV)-pulmonary arteries tube and truncal valve repair by tricuspidization.
The immediate postoperative echocardiography showed a persistent severe aortic regurgitation with moderate stenosis. Thus, we decided to return immediately to the operating room. An aortic valve reconstruction with fixed pericardium using Ozaki technique was performed [5].
The echocardiography performed after the second aortic valve reconstruction revealed no ventricular dysfunction, mild to moderate aortic regurgitation, no aortic stenosis and a good coaptation of the new leaflets (Figure 1).
Following a failure of weaning of mechanical ventilation after 2 weeks of surgery, a chest injected CT-scan was performed and showed an external compression of the trachea as well as the left and right main stem bronchus by a dilated ascending aorta (Figure 2).
An aortopexy was performed and the baby was extubated 5 days after.
6 months later, the baby still free of respiratory signs with a good staturo-ponderal growth. The control of echocardiography showed a mild to moderate aortic regurgitation with no stenosis.
Truncus arteriosus is considered as a congenital heart defect that is reported with many cardiac and extracardiac malformations [6].
The management of aortic valve diseases espacially in the neonatal period, still very challenging. In case of aortic valvuloplasty failure in infant, a rescue therapy is not achievable by a bioprosthesis substitution, mechanical valve replacement is not technically possible in neonates and a Ross procedure is a high-risk operation and not possible in truncus arteriosus.
Despite improved surgical management of patients with truncus arteriosus, truncal valve regurgitation remains a risk factor for early and late morbidity and mortality [7].
Neonatal period and many others factors such as dysplastic TV, severe TVI, TV stenosis, abnormal number of leaflets and dilated aorta still affect significantly the outcome of truncal valve repair.
Tricuspidization techniques for quadricuspid aortic valve repair was originally described by Imamura et al. [8] with a good result on TVI. However, in their study, there was only one neonate among those who had a quadricuspid truncal valve with severe TVI without associated valvular stenosis. Myers et al. [9] have shown that surgical creation of a tricuspid truncal valve seems to provide a best outcomes but, neonatal repair of truncal valve was a significant independent predictor of reoperation.
More recently, Cuttone et al, [10] have shown the feasibility and a good early postoperative result of aortic valve reconstruction following Osaki procedure in children.
Currently, in neonatal period with severe truncal valve disease, the data available on techniques and outcomes still very limited.Aortic valve reconstruction as described by Ozaki et al. [5] remains the recommended option in case of failure of truncal valve repair in newborn. Questions remain regarding the durability of the fixed pericardium used and the late outcomes.
In this case, we reported a tracheobronchial compression by a dilated ascending aorta which resulted in ventilator dependency. It was diagnosed by a computed tomography (CT) after TA repair.
The airway compression (AC) commonly occurs in patients with anomalies of the aortic arch system and vascular rings. However, several conditions cause AC in preoperative congenital heart diseases cases, including a left-to-right shunt causing dilatation of the pulmonary arteries, truncus arteriosus, tetralogy of Fallot with an absent pulmonary valve, and a malposition or dilated aorta
This associated abnormality to TA is rarely described in the literature [3], its early detection and management is essential to reduce further morbidity and mortality risks.
Aortic valve reconstruction should be considered in newborn with severe truncal valve disease. Preoperative meticulous analysis of truncal valve should be performed especially with 3D echocardiography. In addition, aortic CT must be done systematically to eliminate any extrinsic airway compression in order to be carried out at in the same time of TA repair.
Special thanks to the cardiac anesthesia and the ICU teams for their collaboration.
The authors certify that they have obtained all appropriate patient consent forms.
There are no conflicts of interest.

![]()

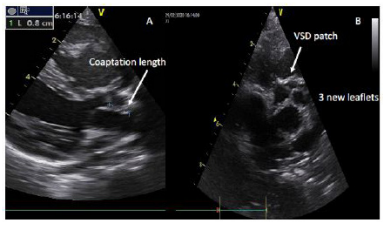 |
| Figure 1: Parasternal long and short-axis echocardiography views showing the good coaptation of the new truncal valve leaflets (A) and the aspect of the Tri-leaflet truncal valve reconstruction (B) |
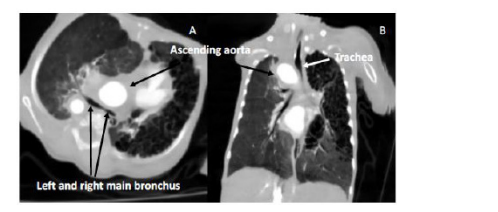 |
| Figure 2: Axial (A) and coronal (B) chest injected CT-scan planes showing an external compression of the trachea and the left and right main stem bronchus by a dilated ascending aorta |




































