Open Access
Research Article
Max Screen
ISSN: 2456-5482
Copyright: © 2019 Alshahrani D. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background:Candidemia is the third most common cause of hospital acquired infection affecting infants in the neonatal intensive care unit (NICU).
Objectives: 1-identify the baseline data about invasive candidiasis (IC) in our NICU, 2-identify the trend of isolated Candida species, 3-identify the risk factors for IC, 4-document the trend of anti-fungal susceptibility, and 5-assess the clinical outcome of neonate who had IC.
Methods:A descriptive retrospective study over a period of 5 years; at a tertiary care center.
Results:We had a total of 3339 admissions over the 5-year period, 27 neonates had 33 episodes of Candidemia, with an incidence rate of 9.9 per 1000 admissions; 16 males and 17 females. The median gestational age was 27 weeks. Seventeen neonates were ELBW, whereas 16 were VLBW, LBW, or NBW. Candida albicans was the most frequently isolated species (61%). The most frequently reported risk factors were the administration of broad-spectrum antibiotics and administration of parenteral nutrition. The overall mortality rate was 33.3%.
Conclusion:Preventive measures to decrease the risk of IC in NICU should be undertaken and followed appropriately, since the outcome even in the well treated patient is serious
Keywords:Candidiasis; Fungal; Neonate; NICU
List of abbreviations:ANC: Absolute Neutrophil; BPD: Bronchopulmonary Dysplasia; BW: Birth Weight; CLD: Chronic Lung Disease; CoNS: Coagulase-Negative Staphylococci; CRP: C-reactive protein; CSF: Cerebrospinal Fluid, CVC: Central Venous Catheter; ELBW: Extremely Low Birth Weight; GA: Gestational Age; GNB: Gram-Negative Bacilli; HFOV: High Frequency Oscillatory Ventilation; HIE: Hypoxic Ischemic Encephalopathy; IC: Invasive Candidiasis; IFI: Invasive Fungal Infection; IVH: Intraventricular Hemorrhage; LBW: Low Birth Weight; NBW: Normal Birth Weight; NDI: Neurodevelopmental Impairment, NEC: Necrotizing Enterocolitis; NICU: Neonatal Intensive Care Unit; PVL: Periventricular Leukomalacia; ROP: Retinopathy of Prematurity; TPN: Total Parenteral Nutrition; VLBW: Very Low Birth Weight; WBC: White Blood Cell Count
Invasive fungal infection is the third most common cause of late-onset sepsis, following Coagulase-negative Staphylococci and Gram-negative bacilli, in the neonatal intensive care units [1,2].
Candida species are the most common causes of IFI, which can present as an isolated candidemia, or as disseminated candidiasis involving the meninges, the heart, the lungs, the kidneys, or the eyes [3]. .
The most frequently implicated risk factors include prematurity, ELBW, CVC insertion, TPN, broad-spectrum antibiotics, NEC, abdominal surgery, mechanical ventilation, and certain medications such as steroids and anti-histamines [4-6].
Although the incidence of neonatal IC was elevated in 1980s and 1990s, the most recent study reported a dramatic fall the incidence of IC in neonatal intensive care units [7,11].
Historically, Candida albicans was the most commonly isolated species, and the most invasive species causing disseminated disease. However, there was an increasing trend in non-albicans Candida as a causative agent for late-onset neonatal sepsis [3,7,8].
IC is associated with a significant morbidity and mortality. Chronic lung disease, retinopathy of prematurity, periventricular leukomalacia, and neurodevelopmental impairment have been noted to be more prevalent in neonates with IC [4,8]. Despite appropriate antifungal therapy, the mortality rate attributed to IC may reach up to 50% among NICU patients [4]. The objective of our study is to identify the baseline data about the incidence of IC at our NICU, review the commonly associated risk factors, identify the trend of Candida species isolated, document the trend of antifungal susceptibility, and to review the clinical outcome of neonates who had IC.
Our study is a descriptive retrospective chart review that was conducted in the neonatal intensive care unit at King Fahad Medical City (KFMC), Riyadh, Kingdom of Saudi Arabia. There is a total of 44 beds in our NICU, divided between level III; 27 beds, and level II; 17 beds. All of our cases were from level III NICU. All neonates with a positive sterile body fluid culture (blood or CSF) for Candida species were included. The study was conducted over a 5-year period; from January 2012 till December 2016. We reviewed the demographic data, risk factors, blood and CSF culture results, other significant lab results, microbiologic data, the management and the outcome.
The study was approved by the Institutional Review Board (IRB.)
We designed a data collection sheet that is composed of seven sections, covering the demographic data, the risk factors, the laboratory data, the isolated Candida species and the antifungal susceptibility, the radiological findings, the management, and the clinical outcome.
We obtained the NICU’s blood and CSF culture results from the microbiology lab over the period of 5 years; from January 2012 until December 2016; then we reviewed it retrospectively in our file system database as well as the NICU system database.
We defined each episode of IC as a positive blood or CSF culture for Candida species. Neonates who had fulminant sepsis and died before blood/CSF culture results and before the institution of anti-fungal therapy; whom later have been diagnosed to have IC; were included as well.
We used the term “early premature” for neonates born earlier than 32 weeks gestation, “late premature” for neonates born between 32-37 weeks gestation, and full-term for neonates born after 37 weeks gestation.
ELBW refers to neonates with a birth weight of less than 1000 grams, VLBW refers for neonates less than 1500 grams, LBW refers for neonates less than 2500 grams, and NBW refers for neonates with a birth weight equal or more than 2500 grams.
We used the term “mild neutropenia” when the ANC was < 1500 neutrophils/microliter, “moderate neutropenia” when the ANC was< 1000 neutrophils/microliter, and “severe neutropenia” when the ANC was< 500 neutrophils/microliter.
NEC is classified as Stage I, II, or III using modified Bell Staging
Comorbid conditions that were assessed included and not limited to cardiac (congenital heart disease), renal (renal cysts, dysplasia), gastrointestinal (atresia, perforation, Hirschsprung disease), neurologic (congenital anomalies, HIE, IVH), and respiratory (pulmonary cysts, BPD).
We defined “recovery with sequelae” as neurodevelopmental impairment, visual or auditory abnormalities, or other organ-system abnormality, such as chronic lung disease or renal impairment. These sequelae were assessed up to 24 months of age, or until the patient was last seen in the clinic.
We defined the mortality secondary to candidiasis as death that occurred within 1 month of the last positive blood or CSF culture for Candida species. Other possible infectious causes of mortality, such as associated Gram-negative sepsis were assessed as well.
Blood culture samples were collected into pediatric blood bottles vials with minimum of 3 milliliter of blood and were inoculated into BACTEC machine (Becton Dickinson) until flagged positive by the machine. Gram stains were performed for all positive cultures and these were subculture on blood, MacConkey, chocolate, and Sabouraud agar.
Colonies on Sabouraud agar were identified by germ tube test positive as Candida albicans, other Candida species were identified by using API 20C AUX (bioMe´rieux, Paris, France). For sensitivity testing, antifungal susceptibility was done on Mueller-Hinton agar with 2% glucose. Minimal Inhibitory Concentrations were determined using E-test with a breakpoint reference from Clinical and Laboratory Standards Institute (CLSI M27-S4) for testing of antifungal susceptibility of yeasts.
The data was initially collected and entered into a Microsoft Excel 2017 (Microsoft Corporation) master sheet. Then the data was reviewed for any missing values or anomalies before being exported to Statistical Package for the Social Sciences (SPSS) for statistical analysis. Data that was missed in more than 30% of the cases was excluded from the analysis.
Baseline and clinical characteristics were presented in frequencies and percentages, whereas all continuous variables were expressed as Mean ± S.D. Pearson’s Chi-square / Fisher’s exact test was applied according to whether the cell expected frequency is smaller than 5. Kruskal-Wallis test was used to determine the median significant difference between the laboratory data and the clinical outcome. P-value of or less than 0.05 was considered as statistically significant. All data were entered and analyzed through statistical package SPSS version 22.
Between January 2012 and December 2016, we had a total of 3339 admissions to our NICU. During this period, a total of 27 patients had 33 episodes of IC. The overall incidence rate over the period of 5 years was 9.9 cases per 1000 admissions per year, where the highest incidence rate was in 2014 (15.1 per 1000 admissions), and the lowest incidence rate was in 2015 (6.2 per 1000 admissions) (Figure 1).
The trend of Candida albicans was almost steady between 2012 and 2016, with an average of 4 cases per year. On the other hand, the prevalence of non-albicans Candida was fluctuating between zero cases in 2013, and 5 cases in the following year.
Demographic data, clinical characteristics, and the risk factors:There was no gender predominance between males and females; 16 versus 17 cases respectively. Early premature neonates were more prevalent compared to late premature and full-term neonates, 63.6%, 33.3%, and 3.0% respectively. The median gestational age was 27 weeks (mean GA = 28.5 ± 4.3 weeks) (Table 1).
ELBW neonates were noted to be more commonly affected compared to VLBW, LBW, and NBW neonates, 51.5%, 21.2%, 21.2%, and 6.1% respectively. The median birth weight was 1010 grams (mean BW = 1200 ± 640 grams).
CVC was present in 66.7% of the neonates, compared to 33.3% with no central line. Almost all of our cases were on parenteral nutrition (97%), and 84.8% were on enteral feeding as well. All neonates received broad-spectrum antibiotics in the preceding month to the development of candidiasis. The most frequently administered antibiotics were Vancomycin (60.6%), Aminoglycosides (57.6%), Meropenem (42.4%), and 3rd generation Cephalosporins (39.4%). Fluconazole prophylaxis was received only by 36.4% of the infants compared to 63.6% who received no prophylaxis prior to the development of candidemia. Most of the neonates had no neutropenia (84.8%), mild (6.1%), moderate (9.1%), and none of them had severe neutropenia (0.0%). Steroid was received by 15.2% of the neonates prior to the development of candidiasis, whereas the rest of the neonates (84.8%) did not receive steroid. Two-thirds of the neonates (69.7%) required assisted/mechanical ventilation as part of their management prior to the diagnosis of IC, whereas one-third of the them (30.3%) did not. Most infants had no NEC (57.6%), Stage I NEC (9.1%), Stage II NEC (3.0%), and Stage III NEC (30.3%). Moreover, 39.4% of all neonates had abdominal surgery, mostly as a management of various stages of NEC, compared to 60.6% who had not. The median hospital stay was 92 days (mean 115 ± 97). Comorbid conditions were present in 29 (87.9%) infants, where 13 (39.4%) had a single comorbid condition and 16 (48.5%) had multiple comorbid conditions. Neurological (48.3%), respiratory (37.9%), and cardiac (34.5%) conditions were the most prevalent (Table 1).
We measured WBC count, ANC, platelets count, and CRP on admission to the NICU and compared it to the time of isolation (Table 2). There was significant rise of the median ANC (3.80 vs. 5.80, p-value 0.007) and CRP (0.30 vs. 23.70, p-value 0.003), and a significant drop of the median platelet count (192 vs. 72, p-value < 0.001) between admission and isolation. There was no significant difference in median WBC on admission compared to the isolation (p-value 0.07).
Abdominal ultrasound was done in 29 patients, 79.3% had normal findings, whereas 20.7% had abnormal findings in the form of renal, hepatic, or splenic hypoechoic lesions consistent with disseminated candidiasis. Echocardiogram was done in 22 patients, 81.8% had normal findings, whereas 18.2% had abnormal findings in the form of myocardial dysfunction. None of the infants evaluated had intracardiac vegetations suggestive of Candida endocarditis. The findings on abdominal ultrasound and echocardiogram were not determinant of a better or worse clinical outcome (p-value 0.244, 0.146 respectively).
We measured the clinical outcome as full recovery, recovery with sequelae, or death. The previously mentioned risk factors were not reflecting the clinical outcome. Gender, maturity, birth weight, CVC, TPN, enteral feeding, antibiotics, anti-fungal prophylaxis, neutropenia, steroid use, mechanical ventilation, NEC, and abdominal surgery were not associated with a better or worse clinical outcome (p-value > 0.05). Moreover, laboratory tests were not significantly reflecting the clinical outcome, namely WBC, ANC, and CRP with p-values of 0.691, 0.156, 0.881 respectively. On the other hand, decreasing platelets count was associated with a worse clinical outcome (p-value < 0.05). The anti-fungal susceptibility testing for Fluconazole was 66.7%, Itraconazole 39.4%, Voriconazole 93.6%, Amphotericin B 95%, and Caspofungin 96.7% (Figure 3). The outcome of infants who received single antifungal therapy was full recovery (22.2%), recovery with sequelae (55.6%), and death (22.2%), compared to infants who received double anti-fungal therapy which was full recovery (41.7%), recovery with sequelae (25%), and death (33.3%). The difference was statistically non-significant (p-value 0.247). Three neonates (9.1%) had fulminant sepsis and died before the preliminary culture results and before being started on anti-fungal therapy. In addition, four neonates developed concomitant Gram-negative sepsis on top of IC, where three of them died. The overall outcome of infants with candidiasis was full recovery in 27.3%, recovery with sequelae in 39.4%, and death in 33% (Table 3).
Infants with Candida albicans who were fully recovered (35%), recovered with sequelae (25%), and died (40%), compared to infants with non-albicans Candida who were fully recovered (15.4%), recovered with sequelae (61.5%), and died (23.1%) had no significant difference (p-value 0.107) (Table 4).
The incidence of IC varies widely between centers and over the years. It may be as low as 1.4 per 1000 admissions per year, or as high as 69 per 1000 admissions per year [4-6,9-12]. In our study, the incidence varied over the years, where the highest was 15.1 per 1000 admissions in 2014, whereas the lowest incidence was 6.2 per 1000 admissions in 2015. The overall incidence over the period of 5 years was 9.9 per 1000 admissions per year, which was almost the same incidence reported by Roshani, et al. in their 12-year study period [3], but higher than what was reported, in the most recent study [11].
There was an increasing concern about the trend non-albicans Candida as a cause of neonatal fungal infection [3,7,10,13-16]. In our study, we found that Candida albicans was the predominant cause of IFI in neonates, accounting for 61% of our isolates, where non-albicans Candida accounted for the rest 39%. Several studies agreed with our finding in that Candida albicans is still the predominant cause of IFI in neonates [3,4,6,9,13,17-21].
We found no gender predominance between males and females; 16 (48.5%) versus 17 (51.5%) cases respectively. The difference was not significant even in the clinical outcome between both genders. In a local study and couple of international studies, there was a slight male predominance [3,4,6,22,23].
Prematurity and LBW are known risk factors for IFI. We found that 63.6% of our patients were born before 32 weeks gestation, with a median gestation age of 27 weeks. Our findings were almost similar to Timo et al. and others [3,4,6,11]. In addition, we found that 51.5% of them weighted less than 1000 grams at birth (ELBW), with a median birth weight of 1010 grams. These findings were comparable to most studies evaluating the risk factors for IFI in NICU [3,4,6,8,11,24,25].
CVC, TPN, and lack of enteral feeding are known risk factors for neonatal sepsis, and especially IC [1-6,14,17,21-24,26-30]. Twothirds of our patients had a central line inserted, and almost all of them were on parenteral nutrition. On the other hand, 84% of them were on enteral feeding as well.
Exposure to broad spectrum antibiotics, especially Carbapenems, 3rd generation Cephalosporins, Vancomycin, and beta-lactam/ beta-lactamase inhibitor are well recognized risk factors for the development of IC among NICU patients [1,4,5,14,24,27,30-33]. In our study, we found that Vancomycin was the most frequently used antibiotic before the development of IC (60.6%), followed by Aminoglycosides (57.6%), Meropenem (42.4%), and 3rd generation Cephalosporins (39.4%).
Fluconazole prophylaxis is a well-known and well-studied protective factor against IFI in NICU patients. Although the compliance may not reach 100%, its effect is well reported [34-38]. Fluconazole prophylaxis is being prescribed based on our local NICU protocols and international guidelines. We start fluconazole for ELBW neonates within the first 48-72 hours of life, as a twice weekly dose for 4-6 weeks or until central line is removed. In our study, 36.4% were on Fluconazole prophylaxis prior to the development of IC.
Steroid has been used in neonates for several reasons mainly related to comorbidities associated with prematurity such as BPD. Several studies observed an increasing prevalence of IFI among neonates who received corticosteroids [1,6,21]. In our study, 15.2% of our neonates received steroids, mainly as a therapy for respiratory distress secondary to prematurity.
Roshani, et al. found that immunodeficiency is a risk factor for development of Aspergillosis rather than IC [3]. On the other hand, Al Thaqafi, et al. found that neutropenia was present in 30% of the patients who had IC [23]. In our study, 15.2% of our patients with IC had neutropenia of varying degree, none of them was severe
Mechanical ventilation is a well-recognized risk factor for IFI, and the risk is proportionately related to the duration of the mechanical ventilation [2,22,24,25,28,30,39]. We had comparable observation where 69.7% of our patients were on invasive mechanical ventilation before the development of IC.
Barton, et al. found in a prospective multicenter study that necrotizing enterocolitis (NEC) is the only independent risk factor for the development of IC affecting 24% of the cases. In addition, Roshani, et al. and Al Thaqafi, et al. reported that prior major surgery is a risk factor for IFI [3,23]. We found that 42.4% of our neonates had NEC, and 39.4% had abdominal surgery prior to the development of IC.
Comorbid conditions were present in 87.9% of our neonates, neurological being the most predominant with a prevalence of 48.3%, respiratory 37.9%, and cardiac 34.5%. All of these comorbid conditions were present prior to the development of IC. This was even higher than what was observed by Tsai, et al. where he found that 59.5% of his patients had chronic comorbidities [29]. Friedman, et al. had followed his ELBW neonates for a total duration of 2 years and reported that 100% had CLD, 26% had PVL, 22% had retinopathy, 60% had adverse neurologic outcomes, and 41% had severe disabilities [8].
The mean hospital stay ranged between 40-100 days, ending either by clearance of infection or death [4,6,24,28]. In our study, we had a median hospital stay of 92 days and a mean of 115 ± 97 days.
Neonatal sepsis, especially IC, is associated with certain laboratory findings. Leukocytosis, thrombocytopenia, and elevated CRP were noted by many researchers as significant laboratory findings and as predictors of clinical outcome [27,40,41]. We found a significant shift in the WBC differentiation, where ANC was significantly rising. In addition, thrombocytopenia and rising CRP were noticed as well. These changes were not significant predictors of the clinical outcome in our study, except for the severity of thrombocytopenia.
In a meta-analysis by Benjamin, et al. they assessed the prevalence of end-organ involvement in neonatal candidemia. They reported the prevalence of cardiac and renal involvement as 5% for both [42]. In addition, Tomerak, et al. documented an echocardiographic finding of left ventricular diastolic dysfunction which was done in cases of neonatal sepsis [43]. In our study,around 80% of both abdominal ultrasound and echocardiogram were within normal limits, while the rest 20% showed evidence of disseminated intra-abdominal candidiasis or myocardial dysfunction.
Amphotericin B remains the main stay in the therapy of neonatal IC [1,3,21,44]. We reported an Amphotericin B susceptibility of 95%, which was close to other local and international studies [18,20,23]. Other researchers reported a varying degree of antifungal susceptibility of Fluconazole, Itraconazole, and Flucytosine [9,18,20,23].
Anti-fungal susceptibility for Fluconazole was 66.7%, whereas Itraconazole was 39.4%. Voriconazole and Caspofungin are considered as an alternative therapy for persistent and progressive candidiasis in those neonates who were unresponsive or intolerant to Amphotericin B [21,45,46]. We found Voriconazole and Caspofungin susceptibility among all isolates to be 93.6% and 96.7% respectively.
Physicians tend to treat disseminated candidiasis with double rather than single anti-fungal therapy [3], even though Amphotericin B monotherapy was found to be effective in most cases of neonatal IC [41]. We found no significant difference in the clinical outcome between neonates treated with a single or double anti-fungal therapy.
The overall outcome measured by the researchers was either full recovery, recovery with sequelae/neurodevelopmental impairment (NDI), or death. Even with appropriate therapy, mortality rate and neurological sequelae are markedly elevated. Most researchers reported a neurodevelopmental impairment to be present in more than 50% of the survivors of neonatal IC and reaching up to 75% in some reports [4-6,31]. In addition, the lowest mortality rate was reported by Lee, et al. and Fu, et al. being 7% and 8.7% respectively [24,39]. On the other hand, many researchers reported a higher mortality rate of more than 20% and reaching up to 50% in neonates with IC [3,4,6]. In our study, the reported full recovery was 27.3%, recovery with sequelae 39.4%, and mortality rate of 33%.
The limitations in our study are (1) small sample size, (2) the data we could obtain were for the past 5 years, and it would be more representative of our NICU if we could obtain a data from 10-15 years back, (3) CSF studies were not done in most of the infants, and those who had CSF studies, none of them had positive CSF culture, (4) neurodevelopmental impairment was not mentioned clearly in the follow-up notes of the survivors.
In conclusion, most of the risk factors associated with IC in neonates were present, although their relation to the clinical outcome was non-significant. Preventive measures to decrease and limit the risk of IC in NICU patients should be undertaken and followed appropriately, since the outcome even in well treated patient is serious.

![]()

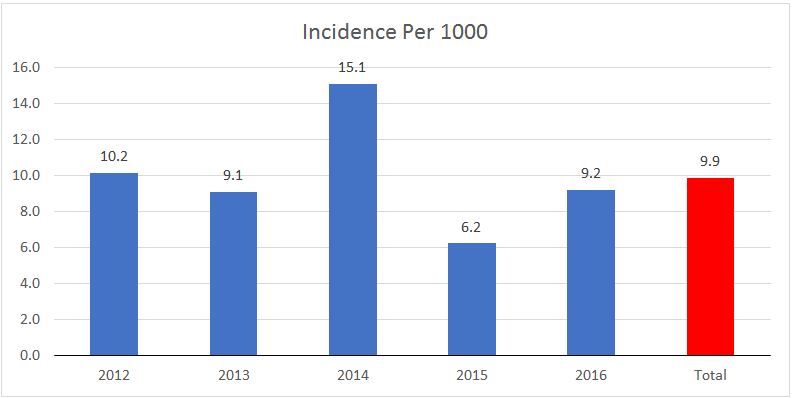 |
| Figure 1: Incidence per 1000 admissions per year |
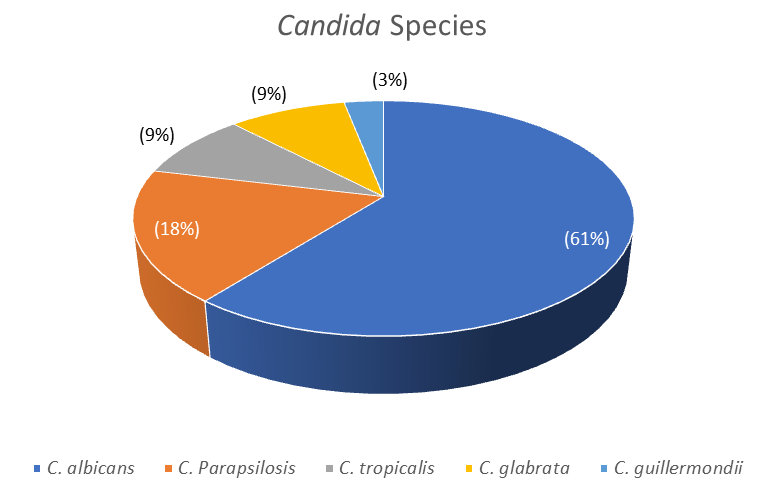 |
| Figure 2: Candida Species |
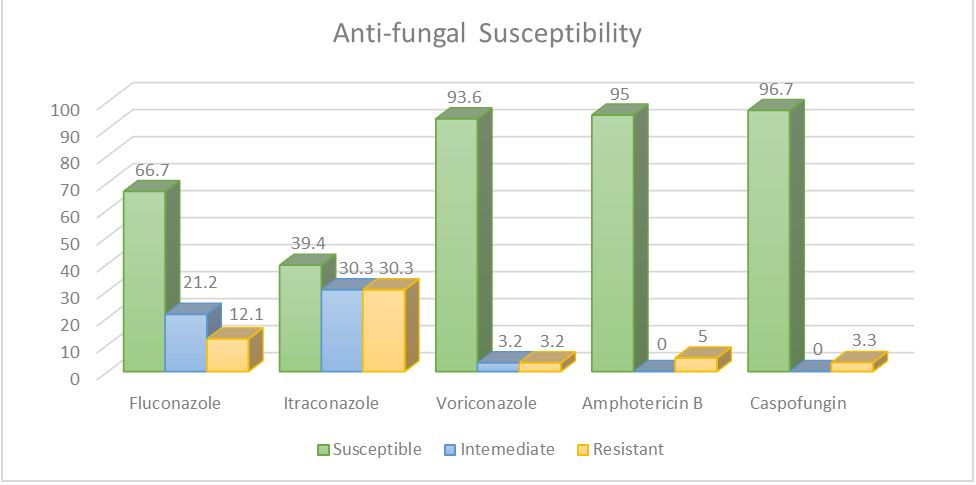 |
| Figure 3: Anti-fungal susceptibility |
Variables |
Number |
(%) |
Median |
Mean |
Gender |
|
|
|
|
Male |
16 |
-48.5 |
- |
- |
Female |
17 |
-51.5 |
- |
- |
Gestational Age |
|
|
|
|
(weeks) |
- |
- |
27 |
28.5 ± 4.3 |
Maturity |
|
|
|
|
<32 weeks |
21 |
-63.6 |
- |
- |
32-37 weeks |
11 |
-33.3 |
- |
- |
>37 weeks |
1 |
-3 |
- |
- |
Birth Weight |
- |
- |
1.01 |
1.200 ± 0.640 |
ELBW |
17 |
-51.5 |
- |
- |
VLBW |
7 |
-21.2 |
- |
- |
LBW |
7 |
-21.2 |
- |
- |
NBW |
2 |
-6.1 |
- |
- |
CVC |
|
|
|
|
Yes |
22 |
-66.7 |
- |
- |
No |
11 |
-33.3 |
- |
- |
TPN |
|
|
|
|
Yes |
32 |
-97 |
- |
- |
No |
1 |
-3 |
- |
- |
Enteral Feeding |
|
|
|
|
Yes |
28 |
-84.8 |
- |
- |
No |
5 |
-15.2 |
- |
- |
Antibiotic Use |
|
|
|
|
Yes |
33 |
-100 |
- |
- |
No |
0 |
0 |
- |
- |
Anti-Fungal Prophylaxis |
|
|
|
|
Yes |
12 |
-36.4 |
- |
- |
No |
21 |
-63.6 |
- |
- |
Neutropenia |
|
|
|
|
No Neutropenia |
28 |
-84.8 |
- |
- |
Mild |
2 |
-6.1 |
- |
- |
Moderate |
3 |
-9.1 |
- |
- |
Severe |
0 |
0 |
- |
- |
Steroid Use |
|
|
|
|
Yes |
5 |
-15.2 |
- |
- |
No |
28 |
-84.8 |
- |
- |
Mechanical Ventilation |
|
|
|
|
Yes |
23 |
-69.7 |
- |
- |
No |
10 |
-30.3 |
- |
- |
NEC |
|
|
|
|
No NEC |
19 |
-57.6 |
- |
- |
Stage I |
3 |
-9.1 |
- |
- |
Stage II |
1 |
-3 |
- |
- |
Stage III |
10 |
-30.3 |
- |
- |
Abdominal Surgery |
|
|
|
|
Yes |
13 |
-39.4 |
- |
- |
No |
20 |
-60.6 |
- |
- |
Comorbid Conditions |
|
|
|
|
Yes |
29 |
-87.9 |
- |
- |
No |
4 |
-12.1 |
- |
- |
Hospital Stay |
|
|
|
|
(days) |
- |
- |
92 |
115 ± 97 |
Laboratory Test |
Median |
Mean |
p-value |
||
|
On Admission |
At Isolation |
On Admission |
At Isolation |
|
WBC |
9.5 |
11.4 |
11.2 ± 8.3 |
14.8 ± 11.5 |
0.07 |
ANC |
3.8 |
5.8 |
4.8 ± 4.8 |
8.7 ± 8.8 |
0.007 |
Platelets |
192 |
72 |
202 ± 78 |
102 ± 85 |
0.001 |
CRP |
0.3 |
23.7 |
4.1 ± 13.5 |
38.8 ± 46.1 |
0.003 |
Antifungal therapy |
Number of cases (%) |
Full recovery(%) |
Recovery with Sequelae (%) |
Death (%) |
p-value |
Single therapy |
18 (54.5) |
4 (22.2) |
10 (55.6) |
4 (22.2) |
0.247 |
Double therapy |
12 (36.4) |
5 (41.7) |
3 (25.0) |
4 (33.3) |
|
No therapy |
3 (9.1) |
0 (0.0) |
0 (0.0) |
3 (100.0) |
|
Total |
33 |
9 (27.3) |
13 (39.4) |
11 (33.3) |
|
|
Number of isolates (%) |
Full Recovery |
Recovery with Sequelae |
Death |
p-value |
Candida albicans |
20 (60.6) |
7 (35) |
5 (25) |
8 (40) |
0.107 |
Non-albicans Candida |
13 (39.4) |
2 (15.4) |
8 (61.5) |
3 (23.1) |
|




































