Open Access
Research Article
Max Screen
ISSN: 2456-5482
Copyright: © 2019 Aqil N. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
We present the case of 18-month-old boy with Urticaria Pigmentosa. Clinical feature was presented as generalized eruption of multiple brown maculopapular lesions on trunk and limbs of one year and 5 months duration. No subjective symptoms were present. First skin lesion occurred in the First month of life. Darier’s sign was positive. Dermoscopy showed a pigment network and a light-brownish blot. Diagnosis of mastocytosis was confirmed by histopathology
Keywords: Mastocytosis; Urticaria Pigmentosa; Dermoscopy
Mastocytosis is a rare disease characterized by proliferation and accumulation of mast cells in various organs (bone marrow, skeletal system, gastrointestinal tract, spleen, lymph nodes and liver), most commonly in the skin. Mastocytosis includes cutaneous Mastocytosis (CM): Maculopapular CM (MPCM)/ Urticaria Pigmentosa diffuse cutaneous Mastocytosis (DCM), Mastocytoma of skin, Systemic Mastocytosis (SM) [1]. Urticaria Pigmentosa is the most common variant of cutaneous Mastocytosis (70, 9%) [2]. Mastocytosis is uncommon in any form [3]. In about 70-75% of cases, lesions of Mastocytosis are evident before the age of 2 years [4]. Recently, two authors reported the Dermoscopic patterns of Mastocytosis [5]. The pigmented network seen in melanocytic lesions was also described in urticaria Pigmentosa. We are presenting another typical case of urticaria Pigmentosa and its Dermoscopy [3,6].
We report the case of 18-month-old infant who was presented by his parents with generalized eruption of multiple brown maculopapular lesions on trunk and limbs of seventeen months duration. There wasn’t a history of generalized urticarial flushing. He had been delivered with cesarean section at full term without any complication. The general health, growth and development of the child were unaffected. There was no family history of similar disease or any other dermatological or autoimmune disease. On examination, there were multiple red brown macular lesions on the trunk and limbs. The mucosae, palms, soles and groins were spared. Dermoscopy showed a central pigment network and a light-brownish peripheral structure (Figure 1 and 2). On stroking the individual lesion, there was formation of wheal and flare (positive Darier’s sign) (Figure 3). No nodules or bullae were seen at the time of the examination (Figure 4). There was no systemic involvement. There was no hepatomegaly, splenomegaly or lymphadenopathy. A provisional diagnosis of urticaria Pigmentosa was made. The histological study revealed hyperpigmentation of the basal layer and increased number of mast cells in dermis. Complete peripheral blood count was normal. The infant was treated with antihistaminic and topical steroids for 4 week which led to the regression of his lesions. The parents were advised regarding avoidance of excessive scrubbing and massage of the skin. At the end of six weeks, the child had only residual pigmentation left at the lesional sites with no new lesion formation.
Urticaria Pigmentosa (UP) is a type of cutaneous Mastocytosis characterized by aggregates of mast cells in the dermis, leading to the development of dark yellow to brown macules. Numerous reddish-brown or yellow-brown monomorphic maculopapular, plaques or nodules appear on the skin of the body [7]. The palms, soles, face and scalp may be free of lesions. Lesions urticate within a few minutes of gentle rubbing (Darier’s sign). The condition is accompanied by variable degree of pruritus [8]. Systemic involvement is rare in urticaria Pigmentosa [9,10]. In our patient, disease occurred in the first month of life. Clinical feature is typical for urticaria Pigmentosa, including reddish-brown macules on the skin of the entire body sparing palms and soles. Darier’s sign was positive. Dermoscopy is a noninvasive technique designed to evaluate color and structures of the epidermis, the dermoepidermal junction and the papillary dermis, which are not seen with the naked eye. One of its main applications is to classify melanocytic and non-melanocytic lesions. Several algorithms have been designed to diagnose melanocytic lesions, and one of the main criteria is the presence of pigmented network [3,6]. However, this Dermoscopic structure is also seen in nonmelanocytic lesions such as dermatofibroma, solar lentigo, seborrheic keratosis, accessory nipple, Kaposi’s sarcoma and even in the normal skin. Recently, two authors reported the Dermoscopic patterns of Mastocytosis [11-14]. The pigmented network was also described in urticaria Pigmentosa, a subtype of maculopapular cutaneous Mastocytosis. It is believed that the pigment network seen with Dermoscopy is due to a high concentration of mast cell growth factor that stimulates melanocyte proliferation and melanogenesis which leads to hyperpigmentation of basal keratinocytes [3,6]. As it was seen in our case [3,6,15]. The diagnosis of cutaneous Mastocytosis is confirmed by a dermal infiltrate composed of mast cells that can be better seen with special stains such as Giemsa, Toluidine Blue or Astra blue. Treatment of UP is mainly symptomatic with avoidance of all known mast cell degranulation stimuli (physical triggers especially rubbing, excess heat, intense exercise, insect and snake bites, medications like aspirin, non-steroidal anti-inflammatory drugs, alcohol and radio contrast media) [15-17]. Antihistaminic such as H1 antihistamines or H2 antihistamines or a combination of both, are the first step medications among systemic treatment options. Doxepin may also be used for its antihistamine properties. The mast cell stabilizers like Sodium Cromoglycate and Ketotifen are also used in patients with UP [18,19]. Topical Corticosteroids can be used and also intralesional Triamcinolone Acetonide injection is available for localized lesions [20].
The study has been approved by the ethics committee of faculty of medicine of fez. An informed consent to participate in the study was obtained from the patient.

![]()

 |
| Figure 1: Multiple red brown macular lesions on the trunk, face, buttocks and upper limbs |
 |
| Figure 2: Multiple red brown macular lesions on the limbs |
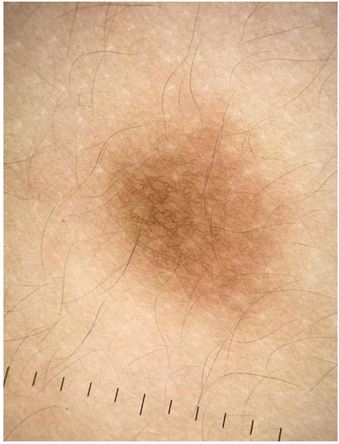 |
| Figure 3: Dermoscopy 10x. Central pigment network and a light-brownish peripheral structure |
 |
| Figure 4: Positive Darier�s sign |




































