Open Access
Research Article
Max Screen
Copyright: © 2019 Portugal FA. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Delirium is common in palliative care and often not diagnosed or mistaken for sedation or anxiety. There are multiple validated screening tools. The clock drawing test (CDT) is a rapid and patient centered screen for delirium which can be followed longitudinally. It also has the possibility of detecting the underlying neuroanatomical lesion. We present a patient with a right hemispheric subdural hematoma who had a reversal of the numbers on the clock face. This has been described with pathology of the right hemisphere. This patient experience illustrates the benefits of the CDT not only in detecting delirium but also revealing the neuroanatomical locus which generated the delirium episode and assisted the palliative care team in identifying patients with appropriate decision-making capacity
Keywords: Clock Drawing Test; Palliative Care
The impact of delirium in palliative medicine is increasing because of the number of patients with comorbidities and assessment complexity due to diverse presenting characteristics [1]. Thirty percent of hospitalized patients and 51% of postsurgical patients develop delirium during a hospital stay. In addition, 25-85% of patients with advanced illnesses during their last weeks of life will have terminal delirium [2,3]. Unfortunately, an accurate understanding of its prevalence and incidence is hindered by the fact that delirium remains underdiagnosed [4]. Reasons that can explain its underdiagnosis or rather, misdiagnosis include similar clinical presentations. For example, hypoactive delirium is often mistaken for depression while hyperactive delirium is confused with anxiety.
Fortunately, several screening tools exist and have been validated for the assessment of delirium. These include the Memorial Delirium Assessment Scale (MDAS), the Confusion Assessment Method (CAM), and the Delirium Rating Scale (DRS) [5]. The consistent use of these tools has the potential to diagnose delirium earlier and thus reduce associated morbidity by reversing the cause for delirium.
The Clock Drawing Test (CDT) is one cognitive screening tool that was used in the following case report [6-8]. The associated benefits of the CDT are that it is a quick bedside screen which can be used in non-verbal patients, is a patient-completed assessment which can be objectively followed over time as well as evaluate a wide range of cognitive functions. The core instruction of the test is to inform the patient to draw the numbers on a clock face and to draw the hands of a clock to show a fixed time. It is important to note that various scoring systems exists although not one appeared to have a superior predictive validity over the other. In addition, no prior expertise is needed to carry out this screening test. Its simplicity relies on the patient to be able to demonstrate correct and even spacing of the numbers along with the correct placement of the hands of the clock. In doing so, clock drawing assessesmemory reconstruction, visual perceptual analysis, motor execution, attention, language comprehension and numerical knowledge.
The following case report describes the use of the CDT by the palliative service for goals of care discussion and demonstrated a unique finding related to the underlying cause of neurological decline. Consequently, the objective was to demonstrate how the CDT can be used to evaluate appropriate patients who have questionable decision-making capacity. Finally, based on an unexpected result, another objective was to interpret and explain the underlying pathology.
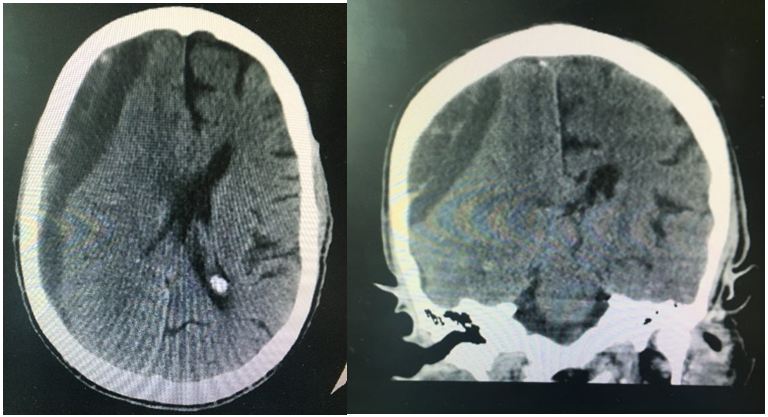
Mr. D.H., a 62-year-old male with a past medical history of end-stage renal disease on dialysis, chronic obstructive lung disease, and chronic systolic heart failure, was referred to the hospital because of progressive frontal headaches and weakness that was associated with an unsteady gait arising from a fall. He has a history of recurrent falls but significantly he sustained a head injury from a fall two days prior to admission. He did not go to the hospital at that time. However, at the time of his dialysis, the patient became dizzy, weak and was sent to the emergency department for further evaluation and a noncontrast CT of the head identified a significant, acute on chronic subdural hematoma involving the right hemisphere with mass effect (Figure 1). Subsequently, he was admitted to the trauma intensive care unit and underwent a right frontoparietal craniotomy for evacuation.
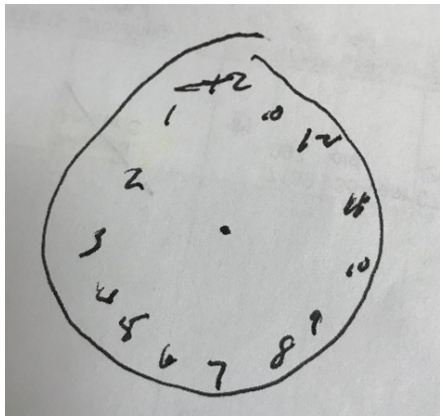
The palliative team was consulted to discuss goals of care given his multiple chronic comorbidities and uncertain prognosis. The patient upon examination was confused and at times incoherent but commented on wanting “everything” done. This was implied that the patient would want all medical interventions and procedures that would prolong his life such as CPR and intubation. However, he had an advanced directive that was inconsistent with his current statement. Consequently, the clock drawing test was done as a screen for delirium and as part of an assessment of decision-making capacity. He was alert and oriented to self but not to place and time. He was confused and inattentive for most of our interview. A bedside CDT was done (Figure 2) which demonstrated a reversal of the number sequence around the clock face (reversed CDT). It was concluded that he was not able to make his own decisions from our examination due to his delirious state.
His wife, who had durable power of attorney according to the advanced directive, requested do not resuscitate measures if his medical condition continued to deteriorate as it would accurately align with his goals of care. Towards the end of the hospitalization, the patient was medically stabilized and discharged to rehabilitation and was to follow-up with neurosurgery for resolution of his traumatic head injury
What makes this finding unique is two-fold: 1) the reversed CDT is an unusual finding and is rarely reported in the medical literature, 2) the importance of identifying delirious patients uniquely by self-assessment through the CDT and 3) the ability of the CDT to determine location of cerebral injury/dysfunction. Kumral and Evyapan described 6of 380 patients with righthemispheric strokeswhodisplayed reversed CDT versus 0 out of 320 patients with left-hemispheric strokes [9]. This is consistent with the findings in our patient given that his subdural hemorrhage occurred along the right cerebral convexity. In another medical report, however, Brugnolo et al demonstrated that reversal of the numbers on the CDT did not only occur in stroke patients but in varying cognitive disorders such as Alzheimer’s dementia, vascular dementia, fronto-temporal dementia and Lewy body dementia [10]. They were also able to determine a peculiar pattern of brain dysfunction in nine patients with Alzheimer’s dementia by brain perfusion SPECT which was associated with the reversal of numbers. Their findings showed that fronto-temporal dysfunction, particularly of the right hemisphere, played a role in reversed CDT [11]. The reversal of numbers on the CDT was also demonstrated in a case report of two delirious patients in the acute care palliative unit by Zama, Maynard and Davis, in which after responding to antipsychotics and opioid rotation, a normalization of the CDT was achieved [12]. This unique finding demonstrates the value of the CDT in identifying delirium, which is vital in palliative medicine and the possibility of uncovering the neuro anatomical pathology [13-16].
There are drawbacks to delirium screening tools. Cognitive impairment is an umbrella term for disorders of thinking, concentrating, reasoning, remembering and formulating ideas and it includes but is not confined to disorders such as delirium [17]. Few studies that have evaluated delirium using the CDT have produced inconsistent results. A study by Bryson et al concluded it was a poor screening tool in a population at high risk for postoperative cognitive disorder [18]. Adamis et al also attempted to address this and concluded that the CDT was good for screening cognitive impairment, but not optimal for detection of delirium in elderly medical patients with the hallmark being waxing and waning sensorium and inattention [19].
Each screening tool has its own limitations. The limitations of the CDT are as follows: its use is determined by ease and familiarity of the user as well as different scoring methodology. Mendes-Santos et al reported a wide variety of CDTs each relying on different systems of administrations and quantitative and qualitative scoring with no consensus on which system produces the most valid results [20]. Other potential limitations include its lack of utility in those patients with visual impairment or neurological difficulties such as paralysis and tremor. Some physicians have expressed concerns of bias from age and education though this is disputed by others. Yet, positive features are that it is not affected by mood, language, and culture as well as its brevity and high negative predictive value (0.95-0.73) [21-23]. However, this was largely done in patients with early dementia or psychosis which may not be applicable to delirium.
In summary, the CDT remains a quick and efficient screening tool that is very useful in palliative medicine, particularly when decision-making capacity is potentially compromised. In this case, we were able to demonstrate a unique and rare instance of reversed CDT, that is explained by a right subdural hemorrhage. This finding would warrant further exploration in a larger, representative sample.

![]()

 |
| Figure 1: Distribution of the sample by percentage (N=225) |
 |
| Figure 2: Distribution of the sample by percentage (N=225) |




































