Open Access
Research Article
Max Screen
ISSN: 2641-7847
Copyright: © 2020 Lahjaouj M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Distant metastases from follicular thyroid carcinoma are not uncommon, but bone localization in the cranial vault is extremely rare. Although these metastases have a poor prognosis, early diagnosis and appropriate treatment can improve quality of life. We report a case of follicular thyroid carcinoma revealed by a metastasis of the cranial vault initially diagnosed as meningioma.
Keywords: Thyroid Cancer; Follicular Type; Metastasis; Cranial Vault
Cranial vault tumors are rare. Their clinical manifestations are almost identical, but their etiologies are very variable. These tumors might be benign or malignant, primitive or secondary. Metastases are frequent but rarely secondary to thyroid carcinoma.
Thyroid cancer accounts for 1 to 2% of all cancers and 90% of endocrine cancers [1]. Distance metastases are rarely revealing and mainly affect the lung and bone [2]. Bone metastases are often found in the scapula, sternum and iliac bone. Cranial localization is rare and is found only in 2.5 to 5.8% of thyroid cancers [3]. We report the case of follicular carcinoma of the thyroid revealed by a single metastasis of the bony and extra-dural cranial vault and we discuss the clinical, para-clinical and therapeutic features of this disease.
We report a case of a 41-year-old male patient with no significant medical history. A painless bump appeared in the right fronto-parietal cranial arch and gradually increased in size for six months. He then experienced intense headaches without other signs of intracranial hypertension. Clinical examination found a painless soft right mass, in the fronto-parietal, 3 cm long and without inflammatory signs. Head computed tomography showed a right parietal soft tissue tumor, which is hypodense, with peripheral and central calcifications and significant bone erosion of the cranial convexity. It measures 50 x 30 x 25 mm and is highly enhanced by contrast medium. This mass had an attachment to the cerebral falx, and caused a slight mass effect on the midline and homolateral lateral ventricle (Figure 1). A meningioma was suspected, and surgical excision was performed. Pathology results revealed a bony, extra-dural cranial localization of a carcinomatous proliferation of thyroid origin (expressing CK7, Throglobulineg, and TTF1). Neck examination did not show any thyroid nodule or lymphadenopathy. Cervical ultrasound showed a hypoechoic right lower polar nodule of 20 x 14 mm with microcalcifications. Further assessment did not show other secondary locations (lungs, bones, etc.). A total thyroidectomy was performed (Figure 2). Pathology examination showed a well differentiated infiltrating multifocal follicular carcinoma, non-encapsulated, and without vascular invasion, staged T3a N0 M1. Head CT scan performed after surgery found the reappearance of the extradural cranial lesion measuring 70 x 50 mm (Figure 3). The patient was put on TSH-suppression therapy and received two courses of radioactive iodine at a dose of 100 mill curies, and ten sessions of external radiotherapy. The response to treatment at his six months follow-up was considered excellent as the head CT scan was normal, neck ultrasound showed no residue and thyroglobulin levels were undetectable. The evolution was good at his two years follow-up.
Distant metastases from differentiated thyroid cancers (DTC) are rare and occur in 10 to 15% of patients [4]. The most common locations are the lung and bone [5].
Cranial metastases from follicular thyroid carcinoma (FTC) are rare. They are exceptionally revealing the primary tumor.
FTC is the histological type of thyroid cancer that is considered the most aggressive, characterized by vascular invasion, explaining the frequency of distant metastases [6]. Although it represents less than 15% of all DTC, FTC has an incidence of bone metastases of 7% to 20% [7]; cranial location represents only 2.5 to 5.8% [3].
FTC has a hematogenous dissemination mostly in areas with high blood flow, such as bone marrow.
Bone metastases are often clinically silent but may present with pain [8]. As a Korean retrospective study shows, only 12 of 28 (43%) patients with bone metastases from follicular or papillary thyroid carcinomas were asymptomatic [9].
Metastases of the cranial vault appear clinically as a fixed, painless mass of scalp, usually unique and slowly increasing in size [10]. Head imaging (CT and MRI) shows an expansive extra dural osteolytic process intensely taking the contrast, with damage to the subcutaneous tissues [11]. The differential diagnoses are meningioma and sarcoma [12].
Treatment is based on surgical excision of bone metastasis when it is unique [13], in addition to total thyroidectomy with central neck dissection including superior mediastinal nodes followed by radioiodine therapy [5]. External radiotherapy remains the treatment of choice in the event of inoperable metastases and positive surgical margins [5,12].
Bone metastases from DTC usually have a worse prognosis than lung metastases [12].
Survival rate of patients with metastases to the cranial vault range between 14 months and 4.5 years [10].
Cranial vault metastases are uncommon and rarely revealing of follicular thyroid cancer. The absence of specific clinical features does not raise suspicion of this etiology, which makes it difficult to diagnose. Management should be multidisciplinary, consisting of total thyroidectomy with lymph node dissection and removal of the metastatic lesion, as far as possible. The treatment will be completed with radioiodine therapy and / or external radiotherapy. TSH-suppression therapy is indicated in all cases.

![]()

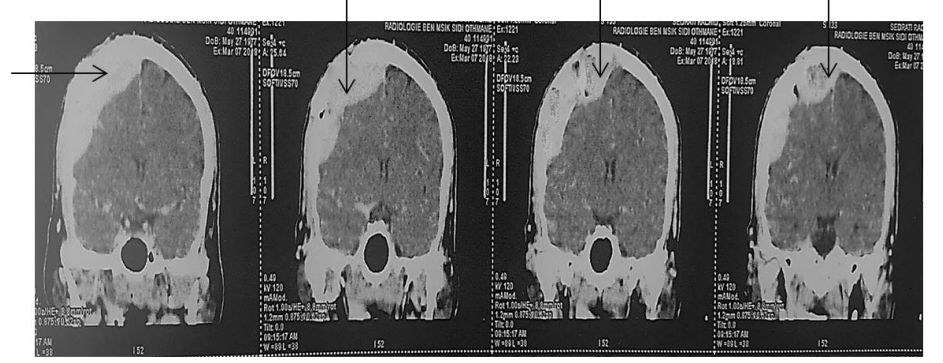 |
| Figure 1: The brain CT san showed a right fronto-parietal process ( black arrow ) |
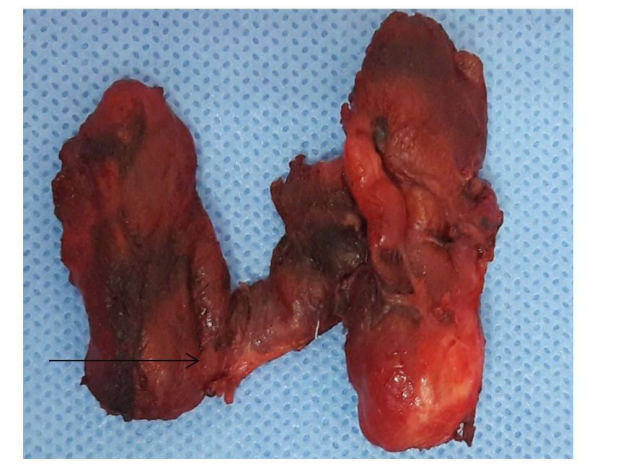 |
| Figure 2: The specimen of total thyroidectomy (arrow indicating the nodule) |
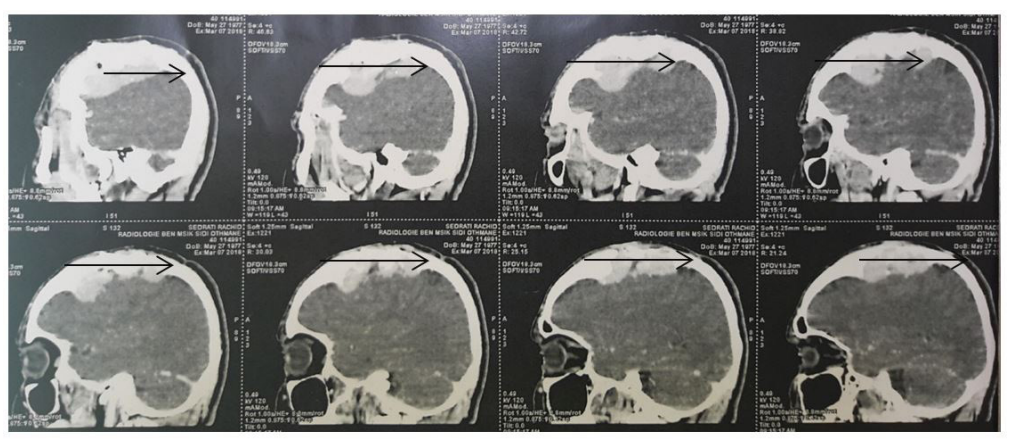 |
| Figure 3: The recurrence of vault metastasis (arrow indicating vault metastasis) |




































