Open Access
Research Article
Max Screen
ISSN: 2641-7847
Copyright: © 2019 Malik JN. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Aim: In the pre-anesthesia era, the anguish of planned surgical maneuver was dreadful and the experience of actual procedure “utterly speechless torture”. Although, the concept of pain relief and even total insensibility was not unfamiliar to medical profession, some of the “Big Giants in Medicine” believed “knife and pain as inseparable” and the efforts to relieve or prevent pain “in vain”. In such a situation the anesthesia,one of the greatest boons of science for mankind, “burst like a revolution on medical profession”. Despite hostility from religious sect, professional colleagues and civil societies the pioneers in discovery of anesthesia stood firm, unshaken by the negative criticism. Although the fate of the active contestant of “Ether Controversy” was mournful,their untiring and dedicated struggle to relieve the sufferings of mankind can never be underscored. Renowned Arab surgeon Ibn al Quff (1232-1286 AD) was the first to suggest anesthesia as independent speciality. However, it took almost 700 years for his dream to come true.
Materials and methods: This prospective hospital based study was carried out in a tertiary care centre during the 5 year period between 2013-2018. Clinical work-up was done and data collected regarding age, site of tumour, alcohol and/or tobacco abuse. After histopathological and imaging study, diagnosis as per TNM staging was made. All 17 patients underwent surgery as the primary treatment, followed with or without postoperative radiotherapy. Kaplan Meier disease free survival was estimated as treatment outcome.
Results: 52.9% cases had squamous cell cancer of the buccal mucosa followed by tongue (35.2%), retromolar trigone (5.8%) and floor of mouth(5.8%) cases. 94% of patients consumed tobacco and/or alcohol. Out of these squamous cell carcinomas, 52.9% were well differentiated, 47% were moderately differentiated and none poorly differentiated carcinoma. Majority (47%) presented in TNM stage IVA followed by stage III, II and I of 17.3% each. Overall disease free survival at 3 years follow-up was 47%.
Conclusion: Majority of the patients presented in advanced stage and almost all of the patients consumed tobacco &/or alcohol. Although association of tobacco/alcohol with oral cancer in young is inadequately reported in literature, our study further corroborates the role of substance abuse, need for cancer awareness and screening in young patients for better treatment outcomes.
Keywords: Oral Cancer; Young; Survival Analysis; Squamous Cell Carcinoma
List of abbreviations: OSCC: Oral Squamous Cell Cancer; UICC: Union for International Cancer Control; AJCC: American Joint Committee on Cancer
Oral cancer is the sixth most common cancer in the world and ranks among the top three cancers in India [1]. It is a major cause of mortality in areas of the world where chewing of tobacco or smoking tobacco with or without alcohol intake is a common practice. OSCC is mostly found in elderly males, however over the last few decades its incidence in young adults including the females has been increasing [2]. Byers et al. was the first to notice this trend in young adults around 1975 and later studies also reported the same findings [3].
The main factor leading to this epidemiological change is still not completely known. Many authors have reported that significant correlation between OSCC and use of alcohol and tobacco is not found in young people [4]. In fact it is interestingly reported that lot of young patients, particularly women report only minimal or no usage of alcohol or tobacco [5]. It is suggested that factors such as genetic inheritance, immunodeficiency, dietary factors, Herpes simplex, Human Papilloma virus, polymorphism of Interleukin-6 and Tumor necrosis factor are also important etiological factors in the development of OSCC either alone or in combination [6].
Not only in terms of causative factors but OSCC in young adults is suggested by many authors to be a different clinical entity than in older patients in terms of behaviour and prognosis [3,7]. They report rapid progression and poor response to treatment in young patients as compared to old patients [8,9]. The aim of this study is to compile and analyse the clinico-pathological profile and survival outcomes of young patients (< 40 years) of OSCC in our institution.
Cases of oral cancer in less than 40 years old patients were studied (Figure 1). Out of a total of 79 patients of head and neck cancer diagnosed and treated in our hospital during the period from January 2013 to December 2018, only 17 patients of OSCC were less than 40 years and included in the study. Demographic data recorded included details regarding age, gender, family history of cancer, site of tumour, tobacco and/or alcohol abuse (Figure 2). WHO grading system was applied to classify tumours into well, moderate and poorly differentiated.
Clinical and pathological details along with radiological findings were used to stage the patients using UICC TNM Classification of malignant tumours as per AJCC 2010. Treatment methods, loco-regional recurrences, and survival outcomes were further assessed in these patients.
We had 19 young-age patients of oral cancer, squamous cell cancer being the commonest type (n=17) while one patient had adenoid cystic carcinoma and another patient had mucoepidermoid carcinoma. The squamous cell carcinoma cases were included in the study among which 9 (52.9%) were well differentiated, 8 (47%) were moderately differentiated and none poorly differentiated carcinoma. Out of these 17 cases majority of patients 94% (n=16) consumed either tobacco or alcohol and only one patient had negative history of alcohol or tobacco use. All 9 cases of buccal mucosa patients (100%) and 5 out of 6 tongue cancer patients (83.3%) habitually consumed alcohol or tobacco or both (Figure 3).
Around 47% (n=8) of tumours were in T2 stage according to the size of tumour, and percentage of tumours belonging to T4a, T1, and T3 were 4 (23.5%), 3 (17.6%), 2 (11.7%) respectively. Regional nodes were involved in 11(64.7%) patients, while 6 (35.2%) patients had N0. According to TNM staging maximum patients, around 47% (n=8) were in stage IVA and patients in Stage III,II, I were 17.3% (n=3) each. Treatment was done according to NCCN (National Comprehensive Cancer Network) guidelines. All 17 (100%) patients received surgery as the primary treatment, followed with or without postoperative radiotherapy.
After the completion of treatment none of the patients had residual disease but one patient died due to post-surgical complication (tracheostomy tube blockage). Post treatment recurrence was seen in 8 out of 17 (47%), Mean duration of developing recurrence was 6 months with a range of 2 months in T4a to 12 months in T1N0. Out of these 8 patients, 5 (29.4%) had local recurrence while 3 (17.6%) had regional recurrence. Six out of these eight (75%) had advanced stage at the time of presentation. Two patients (11.7%) developed second primary during follow up. For recurrent lesions salvage surgery treatment was done in 6 patients and palliative radiotherapy treatment was given to two patients. Overall disease free survival in this study at 3 years follow up was 47% calculated using Kaplan -Meier survival analysis (Figure 4).
OSCC in patients under 40 years of age constituted about 21.5% of all cases of SCC of oral cavity in our hospital which is similar to other Indian studies [10]. However it is observed in a lower percentage ranging up to 6% in western studies [11,12]. All of our patients were males except one female which is in accordance with most of other studies [10-12]. Only few studies have shown a female predominance in young adults [3,13].
Tobacco use in both smoke or smokeless forms and alcohol has been proven to be an important risk factor for development of OSCC [14]. However role of these risk factors in younger patients diagnosed with OSCC have been studied by many authors and found to be debatable [15]. This may be due to the observations as per many studies that in a lot of young patients of OSCC the duration of consumption was too short for carcinogenesis to occur or they never consumed alcohol or tobacco [4,5,16]. In our study around 13 patients had consumed some form of tobacco and 6 were addicted to alcohol. Only 1 patient (5%) in our study never had alcohol or tobacco.
Additional risk factors like the effect of environmental carcinogens, causes of chronic local inflammation and viral infections could also be evaluated for statistical significance but in a larger cohort. A lot of studies have documented HPV as a possible risk factor for oropharyngeal & OSCC, especially in young but due to technical and financial constraints this test could not be performed. None of these young patients in our study had any additional risk cofactors. A positive family history of cancer has been studied as a predisposing risk factor for oral cancer in younger age where it is found to have higher chances of developing carcinoma at the same site in first degree relatives [10]. However in our study none of the patients had positive family history of oral cancer.
Analysis by site of involvement shows that 9 (52.9%) cancer cases were on the buccal mucosa in young patients in our study which is in accordance with most of the other Indian studies [10,17] while majority of western studies report tongue to be the most common site for oral site in young patients [17-19]. Tongue was the next most common site of involvement 6 (35.2%) followed by retromolar trigone 1 (5.8%) and floor of mouth 1 (5.8%) cases. This trend in India may be because of the common habit of keeping tobacco/ quid in the gingivobuccal sulcus which is a significant causative factor for buccal cancer. Similarly in our study a higher percentage, 8 out of 9 (88.8%) patients with buccal mucosa cancer chewed tobacco compared to 4 out of 6 (66.6%) tongue cancer patients.
Most of the tumours in our study were well differentiated a trend which has also been observed by some authors but co-relation of tumour differentiation with prognosis is debatable according to some authors [18,20,21].
It is quite unfortunate to observe that most of our patients presented in the advanced stage of the disease (IVA). This is similar to the finding observed in some other studies [22,23]. This shows the delay in consulting the clinician by the patients However a lot of other studies report a contrasting trend [9,24] which might be due variability in cancer awareness in different populations.
The percentage of patients with nodal involvement was very high/significant similar to other studies [16,25]. Regan et al reported a rate of 50% nodal involvement in his study [18] while Son et al. [25] reported it to be more than 50%. However, Sarkaria et al. in an Indian study described less rate of nodal involvement [9].
Higher rate (47%) of loco-regional failure is probably due to advanced stage at the time of presentation in our series. Interestingly, although in few studies, similar high rate of failure is observed despite of the fact that majority of their patients presented in early stage [9].
These varied results of young patients of OSCC in the literature thus proves that clinico-pathological behaviour and survival outcome of Squamous cell carcinoma in young adults is still not adequately studied. Further studies are needed with large sample size and research into other possible confounding and prognostic factors particularly the role of genetics.
It is important for the doctors to be well aware of increasing trend of OSCC in young adults and any suspicious sign or symptom even in low risk adults should therefore not be ignored. Early detection of OSCC is directly linked to patient survival.
The authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in the study and for data or photographs submitted as part of the Contribution.
The authors declare that no explicit patient data appears in the article
The authors declare that no experiments were performed on humans or animals for this investigation.

![]()

 |
| Figure 1: Oral carcinoma in young patients (a) Buccal; (b) Tongue |
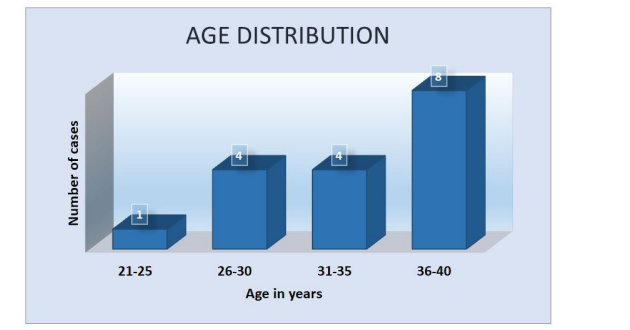 |
| Figure 2: Age distribution in young cases of OSCC |
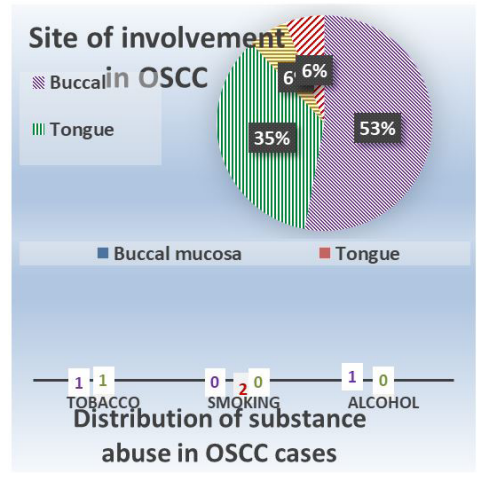 |
| Figure 3: Sites of involvement in OSCC cases & association with substance abuse |
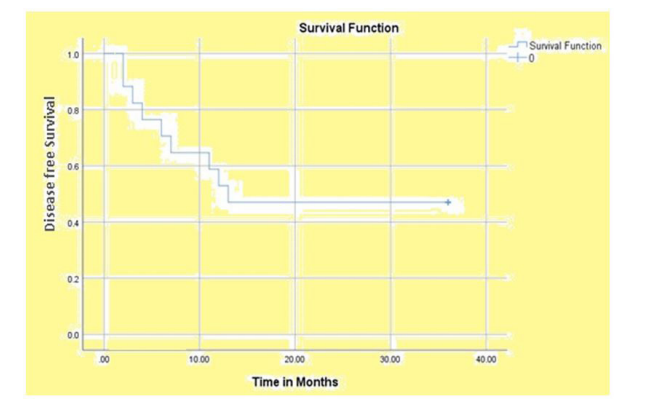 |
| Figure 4: Post treatment disease free Kaplan Meier survival curve |




































