Open Access
Research Article
Max Screen
ISSN: 2641-7847
Copyright: © 2019 Kouhi A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Aim:Prosthesis material and design is thought to have a role in effective sound transmission, rate of complications and success of stapes surgery. Titanium has been shown to be a promising material in this regard. We compared the intra-operative events, complication rate and the hearing outcomes results of stapes surgery using titanium versus fluoroplastic piston prosthesis.
Materials and methods:Patients with diagnosis of otosclerosis underwent stapedotomy using either Causse loop piston fluoroplastic (Medtronic, USA) or Soft CliP piston titanium (Kurz GmbH, Germany) prosthesis. 50 patients were randomized in each group. Main outcome measures were reduction of Air Bone Gap (ABG), Speech Reception Threshold (SRT), subjective change in tinnitus and rate of complications like sensory neural hearing loss, chorda tympani nerve damage and vertigo. Chi square and ANOVA tests were used to compare outcomes between two groups.
Results:All of the patients had successful surgery at 8th week and one failure was seen in fluoroplastic group at one year (ABG< 20). Mean improvement of ABG in fluoroplastic and titanium groups was 37 and 25 dB respectively, which was not statistically significant. Mean reduction of SRT, subjective improvement of tinnitus, and the rate of complications were not different among the two groups.
Conclusion:Titanium Soft CliP prosthesis is as successful and safe as conventional fluoroplastic loop prostheses that have long proven themselves. Although prosthesis selection depends on surgeons’ choice, it seems that this special design may be safer for patients in education setting and surgeons with limited experience
Keywords: Otosclerosis; Stapes Surgery; Ossicular Prosthesis; Titanium; Hearing Loss; Correction of Hearing Impairment
Results of stapes surgery depend on multiple factors. Patients’ variables, surgeon’s experience, method of surgery, as well as prosthesis material and design. Several different prostheses have been made to overcome the technical issues and reduce the rate of complications during this surgery [1,2]. Surgeons encounter multiple risks, such as prosthesis overshoot into the inner ear, Incus dislocation, and problems during prosthesis crimping [3]. Material and design of the prosthesis is thought to have a great role in successful sound transmission by rigid coupling to the Incus, proper weight, strength, and bio-integrity [4].
These issues are even more important in stapes surgery education. It is shown that these faulty events are more common in surgeons who have not passed their learning curve [5,6].
Titanium is being used in stapes surgery since 1990 [5,7]. The most important features of titanium are bio-compatibility, low weight, good strength, and low impedance [5,8]. Also in long term studies, titanium has the least complications and extrusion rate among all the other materials used as middle ear prosthesis [9,10]. Due to its strength it can be manufactured in thinner sizes and more delicate designs which will lead to better view for the surgeon. Soft CliP piston titanium (Kurz GmbH, Germany) have some features in its design that theoretically may overcome some issues during prosthesis insertion. As it does not require crimping, the risk of Incus dislocation may be less, the design loci for Incus helps to hold the prosthesis over the long process and may prevent overshooting into the inner ear. Loop fluoroplastic piston has been widely used in stapes surgery with excellent hearing results and very low complication rate [11]. As titanium prosthesis are significantly more expensive, these fluoroplastic prosthesis are widely used especially in low income countries.
We compared intra-operative events, complication rate and the hearing outcomes of stapes surgery using Soft CliP piston titanium (Kurz GmbH, Germany) and cause loop piston fluoroplastic (Medtronic, USA).
Patients:In this randomized clinical trial 100 ears with conductive hearing loss and clinical diagnosis of otosclerosis were included. Study was performed in a tertiary otology referral center. The main inclusion criteria were consistent history, normal tympanic membrane, well aerated middle ear in patients with sufficient conductive hearing loss, “As” tympanogram and absent stapedial reflex. If intra-operative findings showed any other pathology, patient was excluded from the trial. Also revision cases were not included in this study. A Method and eligibility criterion was consistent during the study and no changes were made. Informed consent was obtained from all of the patients. The ethics review board of Tehran University of Medical Sciences approved this trial.
Surgical Technique:All of the patients were operated by the most senior author (MTK). Every patient underwent trans-canal stapedotomy procedure under general anesthesia. Micro-scissors were used to cut and remove supra-structure. Fenestration of footplate was performed by perforators and hand drills to 0.7 mm in all patients and 0.6 mm diameter prosthesis was used in both groups. Fenestration was sealed with fat graft from ear lobule after prosthesis insertion.
Intervention:Patients were randomly allocated to either Soft CliP or Teflon piston arm by Block Randomization. Randomization was triple blind and surgeons were unaware of the type of prosthesis before the surgery. Physician who did the follow-up and those who did the statistical analysis was blinded as well.
Audiologic Study:Audiologic evaluation including pure tone audiometry (PTA), speech audiometry and tympanogram were obtained from all of the patients before the procedure, and audiometry was repeated 8 weeks and 1 year after. Mean Air-bone gap was calculated in 500, 1000, 2000, 4000 Hz frequencies.
Analysis:Main outcome measures were: air-bone gap, speech reception threshold, family history, tinnitus, duration of disease. Complications monitored were: incus dislocation, vertigo and sensori-neural hearing loss. Statistical package for social sciences (SPSS) version 18 was used to analyze the data. Chi square test was used to compare tinnitus or complications between two groups. ANOVA was used to compare air-bone gap and speech test results between two groups.
One hundred patients enrolled in this study (50 Loop Teflon pistons, 50 Titanium Soft CliP). Mean age of patients was 35 years in Teflon and 37 years in Titanium group. Table 1 shows demographic data of the patients.
Intra-operative complications such as Incus dislocation or tympanic membrane perforation were not seen. Chorda tympani nerve was sacrifices in 6 patients in Teflon and 5 in titanium group. Assuming the criteria of having post-op air-bone gap lower than 20 dB, all of the procedures were successful either at 8 weeks or 1 year. After one year this was 98% in Teflon group. ABG before the intervention was 28.98±6.68 dB in Teflon and 31.05±7.75 dB in Titanium group (p=0.199). Mean ABG after operation was 3.35±4.69 dB in Teflon and 6.1±5.47 dB in Titanium group at 8 weeks. ABG difference before and after the operation was not statistically different between two groups (p=0.137). There was no significant sensorineural hearing loss in both groups. At one year after surgery, ABG improvement was not different too (24.93±5.82 for Teflon and 25.07±4.23 for titanium, p=0.21)
Assuming success as having post-op ABG less than 10 dB, success rate was 90% in Teflon group and 85% in Titanium group at 8th week post op. After one year this was 88% in Teflon and 86% in Titanium group.
Speech reception threshold (SRT) before and after the procedure in Teflon group was 52 dB and 26 dB, respectively. SRT was 57 dB and 29.6 dB before and after treatment in Titanium group. SRT difference before and after treatment was not statistically significant between two groups (p=0.496). Figure 1 shows hearing thresholds before and after procedure in two groups. This difference was not significant in all of the frequencies except 250 Hz that Teflon group had slight but significant better improvement than titanium group. Bone conduction threshold has improved in some frequencies after surgery and over-closure was seen in both groups. Twenty-two patients in Teflon group had pre-op tinnitus, of which 20 had no tinnitus after the operation and the other 2 had decreased intensity, while in Titanium group 16 had pre-op tinnitus, and 15 had no tinnitus and 1 had decreased after the surgery. Vertigo was seen in 3 patients in Teflon and 2 patients in titanium group in immediate post-operative day which resolved with conservative therapy in all after first week. Post-op vertigo had significant correlation with post-op BC level (p< 0.01). The most common prosthesis used was 4.5 mm length. Table 2 shows the size in two groups. Prosthesis length had no effect on postop ABG (P>0.05).
Titanium has been used in ossicular chain reconstruction successfully in the literature [2,7,9,10,12-16]. Many titanium prostheses have been designed for stapes surgery till now. Soft CliP prosthesis is proposed to have some positive features that make its use easier, safer, and possibly more effective. Some of these features are easier insertion due to prosthesis fine structure, anterior extension of superior flange of clip that prevents overshoot into the vestibule, better coupling and contact points parallel to direction of sound wave which leads to better sound transmission, no need for crimping that decreases the risk of Incus displacement. Teflon Loop piston is widely used stapes prosthesis for a long period with good success rate and minimal complications. Special design of Soft CliP prosthesis suggests better results and safer insertion in education institutions and for less experienced surgeons, because overshoot of prosthesis and complications during crimping of the prosthesis are relatively common in these settings.
Neudert et al, studied 3 groups of ossiculoplasties for reconstruction of incus long process, Titanium angled, autologous incus interposition, Titanium clip. Hearing outcomes were not statistically significant among groups and all of these methods can result in good hearing results [13]. However, incus long process reconstruction can be done successfully by bone cement which is much cheaper than prosthesis and has very good results.
In a study by Yung et al, prosthesis dislocation was not different among titanium and hydroxyapatite prostheses [12]. Zhang et al, performed a meta-analysis in ossiculoplasty with titanium and non-titanium prosthesis and they found no difference regarding sound transmission and prosthesis stability [13]. In 2007 Tange et al showed that crimping and non-crimping prosthesis are similar regarding post-op hearing results [3]. Multiple studies have shown good results and good safety with titanium prostheses [1,16-18]. Our study showed similarly good results with both prostheses even at one year follow up. However, longer follow up period can be informative regarding possible complications such as prosthesis dislocation from incus and changes of hearing status during long follow up period.
One of the major draw backs of titanium prosthesis especially in a developing country such as Iran is its high price.
Vertigo was uncommon in both groups, and it seemed that inner ear damage was minimal with both designs and materials. However, presence of post op vertigo was related with post-op BC level, showing that vertigo may be a reasonable sign of potential inner ear damage. This is well described in the literature [19]. Although there are some studies in contrary, but meta-analysis has shown that prosthesis length has no impact on hearing outcomes or complications [20]. Our finding is congruent with this. Titanium had better post-op bone conduction threshold in 250Hz in comparison to Teflon piston. This may show better impedance and acoustic compliance that has led to better recovery of ossicular chain recovery [21]. This effect may be case of higher ABG in this frequency band in our patients, in other words, air conduction threshold are the same but bone over-closure is more in titanium.
One of the most important features of titanium and especially soft-clip design is easier insertion and lower complications especially in un-expert hands. Therefore, in training setting this prosthesis may be a better option. We think another clinical trial regarding hearing results and complication of stapedectomy may be informative and help investigate this consensus.
Both Teflon piston and titanium Soft Clip prosthesis can provide efficient and comparable results for patients with otosclerosis
The study was supported by a grant from the Tehran University of Medical Sciences(grant number: 91-02-48-18346). The titanium prostheses were supplied by Kurz Company at discounted price equivalent to Teflon piston prostheses.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
The ethics review board of Tehran University of Medical Sciences approved this trial.

![]()

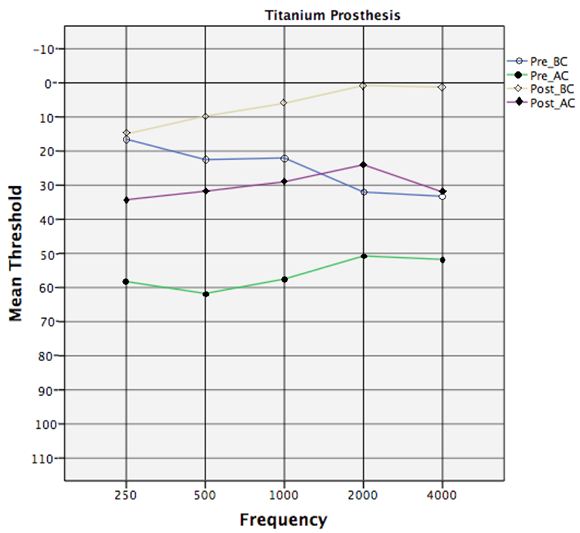 |
| Figure 1: Pre- and Post-operative audiogram of patients in Titanium group |
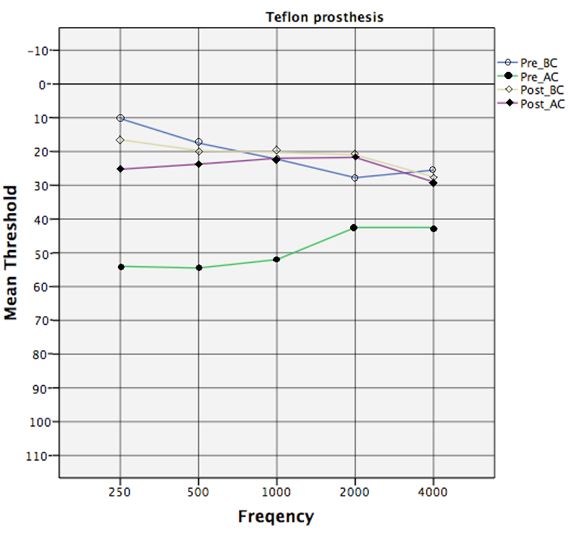 |
| Figure 2: Pre- and Post-operative audiogram of patients in Teflon group |
Parameter |
|
Teflon |
Titanium |
Age |
year (SD) |
35.55(8.18) |
37.75(7.84) |
Pre-SRT |
dB (SD) |
52.00(8.07) |
57.00(9.53) |
Post-SRT |
dB (SD) |
26.00(7.09) |
29.75(7.92) |
Sex |
female/male ratio |
1.86 |
1.86 |
Tinnitus before |
number (%) |
22(44%) |
16(32%) |
Tinnitus after |
number (%) |
2(4%) |
1(2%) |
Vertigo before |
number (%) |
5(10%) |
3(6%) |
Vertigo after |
number (%) |
3(6%) |
2(4%) |
Chorda sacrifice |
number (%) |
6(12%) |
5(10%) |
Size (mm) |
Teflon |
Titanium |
4.25 |
15% |
- |
4.5 |
75% |
55% |
4.75 |
10% |
45% |




































