Open Access
Research Article
Max Screen
ISSN: 2641-7847
Copyright: © 2018 Sofiane N. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Arterio-venous malformation (AVM) accounts for 1.5% of extra cranial hemangiomas and vascular malformations, and is often found in the head, face and limbs. It is the most dangerous type of vascular malformations and is the most difficult to cure. Careful analysis of the clinical features and evaluation of therapeutic options represent basis for successful management of AVMs. We report a case of AVM of the auricle revealed by a head trauma. CT angiography demonstrated an atypical and complex blood supply making surgical resection dangerous.
Keywords: Arterio-Venous Malformation (AVM), Auricle, Selective Embolization
An Arterio-venous Malformation (AVM) is an abnormal connection between one or more arteries and veins, bypassing the capillary system [1]. It accounts for 1.5% of extra cranial hemangiomas and vascular malformations, and is often found in the head, face and limbs. It is the most dangerous type of vascular malformations and is the most difficult to cure. This paper report a larger AVM of the auricle revealed by a head trauma.
A 32 years old woman presented to the emergency room in a state of hemorrhagic shock following cranio-facial trauma at left temporal impact point. On physical examination, the patient was in hemorrhagic shock with hemodynamic instability. The left pavilion of the ear was enlarged, swollen and completely deformed with a vascular mass, bleeding at the slightest touch (Figure 1). After stabilizing the hemodynamic state, a head and cervical CT demonstrated a voluminous arterio-venous formation of the left ear pavilion extending to the level of the outer temporal region and the parotid region with presence of a nidus behind the ascending branch of the mandible and an arterial supply by one branch of the external carotid including the posterior auricular artery and venous drainage towards the external jugular (Figure 2).
Left external carotid arteriography showed a very extensive AVM of the left ear fed by numerous branches from the following arteries:
• Left vertebral artery: by a muscular branch anastomosing with the occipital artery at the level of the Bosnian knot.
• Left carotid siphon: through anastomoses with the internal maxillary artery.
• Left occipital artery dilated and curvy
• Left facial artery
• Left ascending pharyngeal artery
• Median anastomoses of the right external carotid artery
Venous drainage is relatively rapid by dilated veins towards the left external jugular. Embolization was not performed because of the complexity of the arterial supply with presence of dangerous anastomoses (Node of Bosniak)
The pathogenesis of AVM is unclear. Collateral vessel formation, failure of regression of primitive
Arterio-venous connections and local ischemia play a role in the pathogenesis [2]. Especially in case of auricular AVMs, local ischemia plays an important role in the pathogenesis. There were at least two named feeding vessels seen on the angiographic studies of auricular AVMs, and the most common feeding arteries were posterior auricular, superficial temporal and occipital artery [3]. Schobinger classified AVM into four stages. The symptoms of stage I (quiescence) are warm and discolored skin; those of stage II (expansion) are bruit, pulsation, and swelling. Stage III (destruction) is characterized by pain, ulceration, and bleeding; whereas stage IV (decompensation) features cardiac failure [2,4]. The presenting signs and symptoms correlate with the stage of AVM. Although many AVMs are asymptomatic; they may alternatively trigger severe pain and/or bleeding. The most common symptoms are pulsation (51.2%), bleeding (41.5%), and pain (29.3%). Hearing can also deteriorate, presumably because the bruit is audible [5,6]. There are two types of AVM with regard to the flow rate: fast-flowing and slow-flowing. Most of fast-flowing regions are arterio-venous fistulas whereas slow-flow AVMs are produced by venous, capillary, or lymphatic lesions [7].This flow rate based classification may be of importance as different treatment options are needed for the two types. Enlargement of an AVM may be triggered by trauma, infection, or hormonal influences [8].
CT scans show a soft tissue mass, but have a limited role as diagnostic tools in high-flow vascular malformations [1]. Currently, MRI is the standard modality for initial examination because it provides precise anatomical distribution and flow dynamics of the lesion [9]. Also, AVM can be diagnosed with pulsed Doppler, which documents the arterial output, and can be used to follow the progression of an AVM [10]. Selective angiography is most useful for the investigation of AVM, to identify the specific arterial supply, and can be performed in conjunction with super selective embolization of the AVM. It demonstrates the flow characteristics, feeding vessels, and dangerous anastomoses [11]. Management of AVMs is usually conservative and is indicated in stages I and II auricular AVMs, especially during childhood, with regular follow-up. Progression to stage III warrants intervention [1]. Selective embolization followed by timely surgical resection and reconstruction is the most recommended treatment [11]. For the best management of AVMs, it is essential to achieve complete elimination of abnormal arterio-venous shunting. A combined approach of complete surgical excision with prior super selective embolization is the treatment of choice [12]. Although there is no general agreement on the time of the operation after embolization, complete excision should be performed within 48 hours because of collateralization [13]. Highly selective embolization of AVM as a single treatment is rarely curative with high-flow lesions, but is a well-accepted treatment adjunct to aid in surgical resection [4]. In our case embolization was not possible due the complexity of the arterial supply with presence of dangerous anastomoses (Node of Bosniak). Our approach was therapeutic abstention with eviction of sports or professional practices exposing to trauma. The patient was regularly seen in consultation for eight months then lost to follow-up. There was no hemorrhagic incident during this period.
Injection of sclerosants is not useful in AVM as the agent should remain in sufficient amount for certain duration to prove effective [11]. There is no place for proximal ligation of vessels in the management of arterio-venous malformation in any location [3]. Auricular amputation for AVM was recommended by Dingman and Grabb in 1965 [14]. AVM does not usually extend to deep external auditory canal (EAC) and resection can be confined to cartilaginous portion. Reconstruction can be made with costal cartilage, temporo-parietal flap and split thickness skin graft can be performed [3]. However recurrence or re expansion can occur in a couple of years, though it can remain quiescent for decades [11].
Management of head and neck AVMs is challenging and the results can be disappointing. In most cases of auricular AVM, optimal treatment is a combination of super-selective embolization and complete surgical excision. However, treatment is unnecessary (especially in children) if the AVM is small and asymptomatic (stage I and II). Patient must be followed regularly (ideally every six months) in a specialized center; and must be enlightened as to the nature of his condition and evolution modalities.

![]()

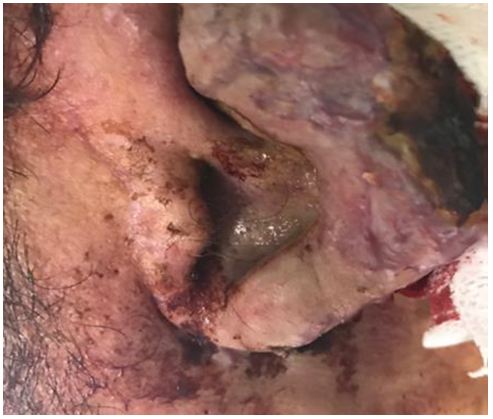 |
| Figure 1: clinical aspect of AVM of the left ear pavilion |
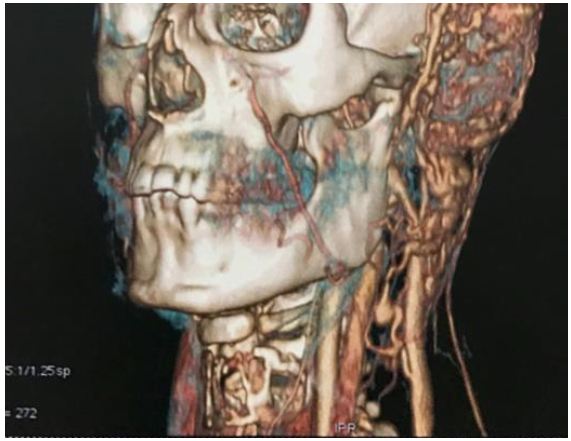 |
| Figure 2: Head and neck CT angiography showing an extensive AVM of the left ear |




































