Open Access
Research Article
Max Screen
ISSN: 2641-7847
Copyright: © 2018 Naceur S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Castleman’s disease is due to a lymphoproliferative disorder by the polyclonal proliferation of B cells inside lymphoid organ.Two types exist: the localized form which is usually benign and multicentric form which is more severe. The main risk is the development of lymphoma. Our aim is to report a case of a 18 years old man patient. Her medical history was unremarkable. She presented with a localized form on the right side of neck lymph node. After the ablation of the nodes,none relapse was noticed.
Keywords: Castleman’s Disease; Localized; Cervical Node
Castleman’s disease or angiofollicular lymph node hyperplasia, first described in 1956 by Benjamin Castleman, is a rare lymphoproliferative disease estimated to be less than 1/100000, the etiology of which is still poorly understood. No genetic or toxic factors have been identified; associated with a high frequency of Kaposi’s sarcoma in HIV patients (role of HHV8) [1]. Can occur at any age with peak frequency in adulthood and typically occurs in two forms: localized and multicentric. The localized form is often benign and is treated by surgical removal in contrast to the multicenter form of poor prognosis and which requires complementary systemic treatment [2,3]. Our goal is to report a case of unicentric Castleman disease in a 18 year old adolescent.
An 18 year old patient admitted to the ENT department for right lateral adenopathies who have been evolving for one year. He did not complain of fever, weight loss,tiredness, or other symptoms. He had no particular background. The physical examination found two masses laterocervical straight, supra centimetric, firm, painless and mobile in the superficial and mobile of the superficial and deep plane. She had neither hepatomegaly nor splenomegaly, and the rest of the ganglionic areas were free. The hologram was normal. C-reactive protein was less than 6 mg/L and the erythrocyte sedimentation rate was 7 mm at 1hour. Electrophoresis of serum proteins found no anomaly. Ultrasonography of the soft tissues confirmed the presence of right cervical lymphadenopathy measuring 20 mm long axis.She underwent complete surgical removal of lymphadenopathies whose histological examination revealed follicular lymphoid hyperplasia. Elsewhere the architecture is reworked by inflammatory fibrosis, seat of a polymorphic infiltrates made of lymphoplasmocytes, histiocytes and granulocytes. Presence also of trabeculae of hyaline fibrosis and a large proliferation and vascular hyperplasia, with vessels with thickened wall. Absence of Hodgkin’s cells (Figure1). The diagnosis of unicentric castleman’s disease was retained in its hyaline-vascular form. She had not received chemotherapy. Its evolution was marked by the absence of recurrence of lymphadenopathy after one year of decline.
Castleman’s disease, also known as angiofollicular lymphoid hyperplasia, is considered a rare disease [4]. Its etiology would still be unknown. It is characterized by a lymphoproliferative syndrome that can appear along the lymphatic system [2].This disease mainly affects adolescents and adults, with no predominance of sex [5]. It is classically manifested in 5 two forms: localized form would sit at 70% in the mediastinum. Cervical localization is only 10-15% of cases. The presence of peripheral cervical lymphadenopathy predisposes to a multicentric form that would have a poor prognosis [1].The latter is accompanied by processions localized symptomatologies and systemic type of polyadenopathies, hepatosplenomegaly, polyseritis central and peripheral neurological signs. The biological anomalies encountered are an inflammatory syndrome, anemia, thrombocytopenia, polyclonal hypergammaglobulinemia, renal insufficiency or even a syndrome of deadly multi-organ failure. His diagnosis is based on histology. In 90% of cases, it is a hyavascular type often associated with a localized form. The rest case takes is found in the multicentric form or the plasmablastic type if the disease is associated with HIV infection [2]. Our patient had an eccentric shape at the neck. This situation is not usual for this clinical form, and it involves making an extensive assessment in search of other foci of lymphadenopathy to avoid missing a multicentric form whose care would be different and the reserved prognosis. She had benefited from a surgical removal of her lymphadenopathies at the same time to aim diagnostic and therapeutic adapted to her case.exeresis is indeed the only treatment of the unicentric form of Castleman’s disease [5]. Moreover, its good evolution was proved by the absence of recurrence to this day. Another important point was to be able to eliminate the diagnosis of this disease from a pathology with ganglionic expression accompanied by similar histological signs as some autoimmune diseases systemic lupus erythematosus,rheumatoid arthritis,gujarot-sjorgen syndrome),an infection viral to EBV [6];the second is the obligation not to miss aauthentic lymphoma, knowing that the plasmablstic type could be transformed into non-Hodgkin’s lymphoma, and that a castleman’s disease could sit in the breast or satellite of a disease of Hodgkin [7].
Castelman’s disease is one of many differential diagnoses of lymphadenopathy.Anatomopathological examination is essential to make the diagnosis. The unicentric form is often benign and curable by surgical excision alone. On the other hand, extra-thoracic localization usually associates with the multicentric form that requires complementary systemic treatment and is considered to have a poor prognosis. An assessment of extension in search of other localizations is then essential not to miss the latter clinical form.

![]()

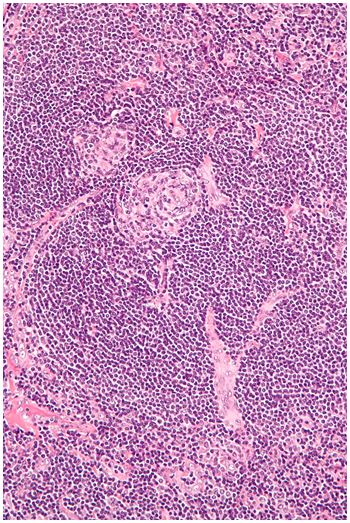 |
| Figure 1: Follicular hyperplasia and concentric deposits of lymphocytes in (bulb of onion) |




































