Open Access
Research Article
Max Screen
ISSN: 2639-930X
Copyright: © 2024 Betts Tony. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background:The Side Shift approach to correction of scoliosis curves has been used by therapist at the Royal National Orthopaedic Hospital (RNOHT) for over 30 years. The Side Shift approach was developed by Mrs Min Mehta, and has been Modified using consensus based evidence of SOSORT. Clinical observations had indicated that not all patients could actively (Auto) correct to beyond the trunk midline, a key principle of Side Shift. At the RNOHT a classification system based upon the ability of an individual to auto-correct the spine during a Side Shift movement has been developed to aid the appropriate application of the shift exercises and allow future comparative analysis
Aim:To develop a Clinical Classification System for the Physical Therapy treatment of scoliosis, which is reliable, valid and universally accepted.
Methods:58 Consecutive patients who have AIS were tested, by two clinicians (a Physiotherapist and an Orthotist), in 2013. The clinicians were blinded to the classification of each other. The results were tested for reliability. Three types of SideShift were developed. Type 1: Flexible, Type 2: Stiff, and Type 3: Rigid. Data was collected for comparison on hypermobility, Cobb angles, and ATR scores.
Results:Agreement was measured using the Kappa statistic (κ). Intra-rater Reliability: The kappa value for agreement between the raters measures on occasion one and occasion two showed substantial agreement, κ = 0.77, 95% CI (0.61 – 0.91), P < 0.01. There was good intra-rater reliability.
Type 1 Side Shift accounted for 73% of subjects with an average Hypermobilty score of 6/9. A one way analysis of variance (Anova) was calculated on Hyperlaxity score by Side Shift Types . This analysis was significant F (2, 32) =7.55, p<.001.
Conclusion:The results suggest that the Side Shift classification is a reliable descriptive scale of the mobility of the trunk and the ability to Auto-correct across the midline of the body.
Keywords: Scoliosis; Royal National Orthopaedic Hospital; Hyperlaxity; Side Shift Classification
Scoliosis can lead to a truncal shift of the spine away from the mid-line posture in the coronal and sagittal planes. This shift is known as a lateral deformity of the spine associated with the rotation of the spinal vertebrae, the principle structural deformity of scoliosis. Classification systems exist to guide the management of surgery (the King and Lenke systems) and Brace treatments (Cheneaux, Rigo and SpineCor). Few exist for the management of physical exercise (Lehnerth-Schroth classification system) [1-10]. The Side Shift approach to correction of scoliosis curves has been used by therapist at the RNOHT for over 35 years [2]. The approach of using excessive side trunk movements to correct the lateral shift of the trunk in the coronal plane is based on the theory that a flexible curve can be stabilised with lateral movements.
These lateral movements promote a reduction in the postural forces which affect a structural curve. Min Mehta proposes that growth can be a corrective force for spinal deformity in Children. Movement is directed in opposition to the curve of the spine towards the lower veterbral tilt, below the apex of the curve. Whilst correcting the curve position through truncal shifts, the body is using muscular forces and connective tissue stretches/ mobility to re-align the soft tissue components of a scoliosis. It is felt that frequent repetition of corrective movements also helps to promote somo-sensory integration of the spinal position to a more upright and physiological posture [1-11]. An evaluation of the treatment methods to treat scoliosis at the Royal National Orthopaedic Hospital Trust (RNOHT) was undertaken to provide evidence-based reasoning for this treatment philosophy.
Theoretical science models provide the basis for exercise based corrective treatments. The Wolff law states that skeletal transformation is dependent on the exertion of pressures from outside the animal”: the Davis law for soft tissue remodelling, relates elongation of ligaments (soft tissues) to applied tension (through elongation or shortening forces) and the Frost principle, defines that bone re-modelling can be adapted by the relationship between applied strains and bone mass. These law’s provide the impetus for studies which seek to explore the clinical capacity of correcting spinal growth through promoting oppositional movements (exercise) to convex curve patterns and promoting postural awareness of the spine. Further basic science studies by Stokes [4] provide the biological basis to explain the influence of movement and muscle forces upon the curves of scoliosis, and quantify the amount of corrective force necessary to influence curve angles [1].
Prior Clinical studies by Min Mehta demonstrated clinical improvements using the Side Shift approach. Min Mehta used single and multiple case reports to demonstrate positive clinical and radiological correction of scoliosis by Side Shifts. This study was an unblinded retrospective study presenting observational and radiological results of over 2530 patients. Clinical Studies by Boer et al [10] and Murayama [4] also demonstrated significant Curve changes with and during Side Shift exercises. These articles represent low quality research articles according to strict criteria of methodological reviews (JB). However they do represent an attempt to measure clinical outcomes related to Side Shift exercises. The Clinical model has been developed and modified at the RNOHT. The Aim of all exercise based treatment is to restore the upright posture of the trunk over the pelvis, and correct or stabilise the curve. The side shift approach has been modified with practice, experience and clinical re-evaluation. It includes principles of the Schroth regime (Rotational angular breathing techniques) and treatment advice suggested by consensus from SOSORT group [11].
Clinical observations had indicated that not all patients could actively (Auto) correct to beyond the trunk midline, a key principle of Side Shift. The classification system developed was based upon the ability of an individual to auto-correct the spine during a side shift movement. It was developed to aid the appropriate application of the shift exercises and allow future comparative analysis. Three types of Side-Shift were developed and are described as;
Any pattern curve which can be corrected by shifting the trunk to beyond the coronal midline to produce a mirror curve correction to the contra lateral side (concavity) of the scoliosis. These curves are extremely flexible.
Any pattern of curvature which can be corrected to the mid line of the coronal plane to place the trunk over the pelvis and C7 is in plumb line with sacrum, the convex curvature of the spine reduces and rotated vertebrae partially de-rotate.
Any pattern of curvature which cannot correct to the midline, remains shifted over to the convexity side during a side shift manoeuvre and the vertebrae does not de-rotate, but remains prominent. These curves are extremely rigid and may represent a severe structural curve.( see Figure 1 A schematic view of the Three types of Side Shift).
The classification scale was tested for intra and inter-reliability prior to its use in the department.
58 consecutive patients with a medical diagnosis of AIS were recruited for this study. The patients were categorised. Two different members of the treatment team at the Royal National Orthopaedic hospital (2 Therapist) and one Orthotist, were blind to the categorisation of the presenting patients. Each member of the team was given a descriptive and illustrative summary of the agreed descriptive Side Shift Classification explained above.
Observations and measurements made were considered a normal part of the clinical examination and analysis a clinical audit, therefore ethical approval was not sort.
Patients received brief examinations recording Hypermobility scores according to the Beighton scale and measurements of ATR, by scoliometer. Cobb angle measurements and Curve pattern diagnosis were made previously by Consultant surgeons.
The patient sample consisted of adolescents diagnosed with Adolescent Idiopathic Scoliosis (AIS) by a Consultant Orthopaedic Surgeon. Inclusion criteria comprised AIS patients aged 7 to 18 without neural axial abnormalities, excluding those with congenital or neuromuscular scoliosis, with curves greater than 20 degrees and Risser 0-5.
Agreement was measured using the Kappa statistic (κ). Kappa values were assessed as poor if κ< 0.00, slight if 0.00 ≤ κ ≤ 0.20, fair if 0.21 ≤ κ ≤ 0.40, moderate if 0.41 ≤ κ ≤ 0.60 , substantial if 0.61 ≤ κ ≤ 0.80, or almost perfect if κ > 0.80 (Landis and Koch 1977).
Fishers Exact Test was used to asses the associations between the categorical variables of interest
Pearson’s correlation coefficient (r) was used to asses the relationships between the numerical variables of interest.
Sample size calculations were performed to ensure the study would provide confidence intervals of a desired width. With 46 patients the study has adequate numbers to detect agreement using the kappa statistic with two-sided 95% confidence intervals of width 0.3.
All statistical analysis was performed using Stata/IC version 12.0, (StataCorp, College Station, TX, USA). A P-value < 0.05 was considered statistically significant.
A total of 58 patients were included in the study.
Table 1 shows the scores obtained by rater one on occasion 1 and occasion 2 for each of the 58 individuals. The frequencies with which the scores agree are shown along the diagonal.
The kappa value for agreement between the raters measures on occasion one and occasion two showed substantial agreement, κ = 0.77, 95% CI (0.61 – 0.91), P < 0.01. There was good intra-rater reliability [12].
Table 2 shows the scores obtained for rater 2 and rater 3 for 21 individuals. The frequencies with which the two raters agree are shown along the diagonal.
The kappa value for agreement between the two raters measures showed substantial agreement, κ = 0.7623, 95% CI (0.504 - 1.000), P < 0.01. There was also good inter-rater reliability.
12 (21%) of the 58 individuals had a lumbar curve, 39 (67%) Thoracic, 5 (9%) Thoroco-lumbar and 2 (3%) cervical.
33 (57%) of the 58 individuals were scored type 1, 10 (17%) type 2 and 15 (26%) type 3.
Table 3 shows the Category of type scores (rater 1, ocassion1) and Descriptive curve measures for the 58 individuals.
Fishers Exact Test confirmed there was a significant association between the Descriptive curve and category of type score, P = 0.03.Table 3 shows the differences in the distributions of category of type scores by descriptive curve.
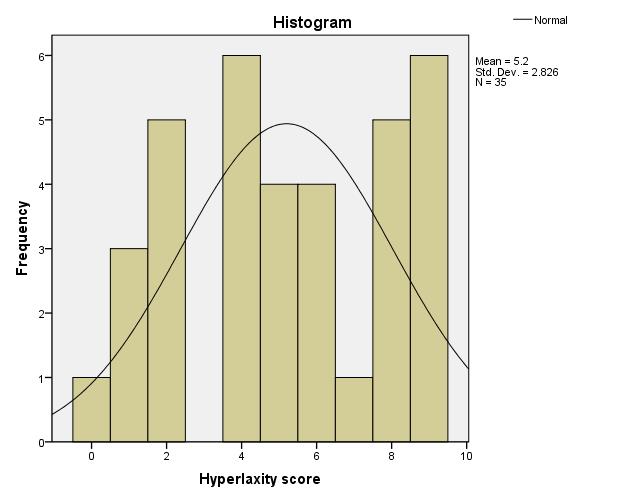
Hyperlaxity score showed a normal distribution (see below) therefore we could use a parametric test- anova to show differences between groups.
A one way analysis of variance (Anova) was calculated on Hyperlaxity score by Side Shift types (see Table 1). This analysis was significant F (2, 32) =7.55, p<.001.
Posthoc analyses using the Bonferroni post hoc criterion for significance indicated that the average Hyperlaxity score was significantly lower in the Type 3 (M=2.14, SD=1.35) condition compared to Type 1 (M=6.26, SD=2.6), p<.001. Findings also confirmed that Hyperlaxity score was significantly lower in Type 3 (M=2.14, SD=1.35) compared to Type 2(M=5.33, SD=2.55) (p< 0.05).
There was no significant difference found between Type 1 (M=6.26, SD=2.6) and Type 2 (M=5.33, SD=2.55) (p>0.05).
Among the patients, Side Shift types were distributed as follows as Type 1, Type 2, and Type 3. Correlation analysis revealed a significant association between Side Shift types and hypermobility scores (p < 0.05), indicating that patients with certain Side Shift types tended to exhibit higher hypermobility scores compared to others.
This Study has demonstrated that the proposed Side Shift Classification can be a reliable and valid tool for describing, the relative mobility of the spine. Different Types of Side Shift, correlate well with generalised flexibility scales. The Type 1 description of flexibility (mirror image correction) correlates with Hypermobility scores above 6/9 which is considered to describe Hyperlaxity of the joints (Grahame). An Analysis of the different categories of the Side Shift Types with Hyperlaxity (hypermobility) demonstrated a significance difference between the different types and Hyperlaxity scores. The average Hyperlaxity score (2/9) for Type 3 (Rigid) was significantly lower than compared to Type 1 (flexible) Side Shift. This indicates that the ability to Side Shift is related to generalised Hyperlaxity scores. The less flexible the subject is, the less mobile is the ability of the subject to Shift the Trunk across the midline.
There are two main movement concepts important for the Side Shift approach and they are [2,7];
1. Over -correction as an active movement force to promote curve correction during growth: Auto-correction( Min Mehta ).
2. Mirror image correction- truncal side shift; (Harrison), to aid pain and correct truncal mal-alignments
The results of this descriptive study, suggest that the classification proposed, is a reliable system for separating differences in the mobility of truncal Side shift exercises used in the treatment of scoliosis. The scale allows different therapist and non operative practitioners to review the patient’s ability to auto-correct, beyond the Midline posture –mirror image, and to the midline posture. The aim of exercise therapy, in the treatment of small to minor to moderate Scoliosis (spinal deformities in any plane of motion), is to re-establish upright physiological postures and aid the correction and/or stabilisation of the presenting spinal deformity. The lack of physiotherapy Classifications for the treatment of scoliosis makes it difficult for practitioners to communicate the efforts of corrective movements. The initial aim and reasonings for developing these classifications are
The scale provides a description of mobility which correlates with generalised flexibility of patients as defined by Hypermobility scores. Types 1 Side Shifts are flexible curves that can Mirror image correct the posture during truncal lateral translations. These patients have Hypermobility scores above 6/9, which suggest that generalised Hypermobility does relate to the ability to mirror image correct the truncal posture beyond the Midline in the coronal plane. These provide some clinical-construct validity to the Side Shift scale. It relates to flexibility in general.
An analysis of the results suggests that this is a useful descriptive basis for classifying Side Shift mobility in a population with Scoliosis. The reliability scores indicate that this descriptive scale can identify three separate types of mobility during the Side Shift manoeuvre. Type 1 Side Shift can over- correct the Trunk posture to beyond the midline and create a mirror image of the spinal posture from its resting position in standing. These spines have the flexibility to move into the overcorrected position. The overcorrected position provides the forces needed to create growth modulation upon the spinal tissues. (Mehta 1984, Stokes [4]. The ability to do the exercises may have a profound effect upon the effectiveness and outcomes of the technique. It may also define the boundaries of use of the Side Shift technique to scoliosis patients with limited ability to Side Shift. Type 1 patients had a strong correlation to generalised Hyperlaxity (hypermobility) scores. This suggests that being flexible in general is related to being able to overcorrect the spinal posture. It also suggest that this group of patients were more commonly associated with generalised Hyperlaxity. The average score of Hyperlaxity was greater than in the general public and representes ( 6/9 Score) a category of patients defined as hypermobile (Grahme R) Further study is needed to analyse the significance of this findings. It could be that generalised Hypermobility, a Type 1 Flexibility score and curve (Cobb angle) outcomes are related. Type 2 Side Shift represented Curves that could correct the trunk position to the Midline (neutral Coronal balance). This is an important physiological consideration as it places the spine in the most universally accepted natural and healthy posture [8, 9, 10, 11]. This is often the aesthetic goal of medical outcomes for patients with scoliosis. [11] Type 3 Side Shifts, are defined as rigid curves because they are unable to either move to a corrected position in the midline (neutral posture) or overcorrect. This is considered a disadvantage for the correction of spinal Curvatures by means of exercise manoeuvres. If the spine of a patient cannot move to a correctable posture it is probable that movement is not a corrective force for these patients.
The findings underscore the clinical significance of the Side Shift classification system in scoliosis management. By categorizing patients based on Side Shift types, clinicians can tailor treatment strategies more effectively. For instance, patients with Type 3 Side Shift may benefit from specific interventions aimed at addressing hypermobility, whereas those with Type 1 Side Shift may require different therapeutic approaches.
Moreover, understanding the correlation between Side Shift types and hypermobility scores can inform prognosis and guide treatment decisions. Clinicians can anticipate potential challenges associated with hypermobility in certain patient subgroups and implement preventive measures accordingly. This personalized approach to scoliosis treatment is essential for optimizing outcomes and enhancing patient care.
In conclusion, the Side Shift classification system offers valuable insights into the heterogeneity of scoliosis presentations and their implications for treatment planning. By incorporating Side Shift assessment into clinical practice, healthcare professionals can better address the unique needs of AIS patients and improve treatment outcomes.
Anecdotal evidence from the department suggested that the Side Shift exercises are appropriate for smaller flexible and postural idiopathic curves, less than 30 degrees in growing children. The author presents this article as a preliminary study in the development of the Side Shift Classification system.
A follow up with more clinicians involved in the reliability would help to add proof to the categorisation. The categories are simple, with three descriptive types that correspond to movement. The addition of objective measures relating to the amount of shift may improve the robustness of the categories. There were times when the two clinicians disagreed over the categories especially between Type 2 (stiff) and Type 2 (rigid) it is possible for the trunk to move (translate) without the apex of the curve to move. This can present a problem when deciding if the spine is in a neutral position relative to the head and pelvis. We resolved this after the study by agreeing that if movement was possible and the spine was able to move above the sacrum that functionally this could be considered a effective mid position which would improve the coronal balance.
Modifiers may need to be added to the classification. The Author observed that some curves, which were prominently rotated, would lose the rotation when they had Side Shifted. This appeared to be a resolution of the transverse plane deformity during the Side Shift. Other Curves remained rotated. The clinical significance is not yet known, but it is proposed that Curves which can Correct in multiple planes during one movement may have a better outcome with exercises that those that move in only one plane.
The significance of a scale is only useful if it can in some way be related to outcomes of treatment. A further study is planned to examine the outcome of the different categories.
In addition to the identified limitations, potential biases or confounding factors should be considered. For example, the study may be subject to selection bias if the patient sample is not representative of the broader population of AIS patients. Moreover, the study's reliance on observational data may introduce information bias, as subjective interpretations of trunk movement and curve characteristics could vary among clinicians.
These limitations could impact the study's generalizability, as findings may not be applicable to all AIS patients. Furthermore, the lack of standardized protocols for Side Shift assessment and classification may hinder comparisons with other studies and limit the ability to draw definitive conclusions about the classification system's utility in clinical practice. Addressing these limitations in future research could strengthen the validity and applicability of the Side Shift classification system.

![]()

 |
|
Test 2 |
|
||
Test 1 |
1 |
2 |
3 |
Total |
1 |
29 |
4 |
0 |
33 |
2 |
0 |
9 |
1 |
10 |
3 |
1 |
2 |
12 |
15 |
Total |
30 |
15 |
13 |
58 |
|
Rater 3 |
|
||
Rater 2 |
1 |
2 |
3 |
Total |
1 |
10 |
3 |
0 |
13 |
2 |
0 |
2 |
0 |
2 |
3 |
0 |
0 |
6 |
6 |
Total |
10 |
5 |
6 |
21 |
|
Type |
|
||
|
1 |
2 |
3 |
Total |
Lumbar |
6 (50%) |
0 (0%) |
6 (50%) |
12 |
Thoracic |
23 (59%) |
9 (23%) |
7 (18%) |
39 |
Thoroco-lumbar |
4 (80%) |
1 (20%) |
0 (0%) |
5 |
Cervical |
0 (0%) |
0(0%) |
2(100%) |
2 |
Descriptives |
||||||||
Hyperlaxity score |
||||||||
|
N |
Mean |
Std. Deviation |
Std. Error |
95% Confidence Interval for Mean |
Minimum |
Maximum |
|
Lower Bound |
Upper Bound |
|||||||
Type 1 |
19 |
6.26 |
2.600 |
.596 |
5.01 |
7.52 |
0 |
9 |
Type 2 |
9 |
5.33 |
2.550 |
.850 |
3.37 |
7.29 |
2 |
9 |
Type 3 |
7 |
2.14 |
1.345 |
.508 |
.90 |
3.39 |
1 |
4 |
Total |
35 |
5.20 |
2.826 |
.478 |
4.23 |
6.17 |
0 |
9 |
|
Sum of Squares |
df |
Mean Square |
F |
Sig. |
Between Groups |
87.059 |
2 |
43.529 |
7.548 |
.002 |
Within Groups |
184.541 |
32 |
5.767 |
|
|
Total |
271.600 |
34 |
|
|
|
(I) Type |
(J) Type |
Mean Difference (I-J) |
Std. Error |
Sig. |
95% Confidence Interval |
|
Lower Bound |
Upper Bound |
|||||
Type 1 |
Type 2 |
.930 |
.972 |
1.000 |
-1.53 |
3.38 |
Type 3 |
4.120* |
1.062 |
.001 |
1.44 |
6.80 |
|
Type 2 |
Type 1 |
-.930 |
.972 |
1.000 |
-3.38 |
1.53 |
Type 3 |
3.190* |
1.210 |
.038 |
.13 |
6.25 |
|
Type 3 |
Type 1 |
-4.120* |
1.062 |
.001 |
-6.80 |
-1.44 |
Type 2 |
-3.190* |
1.210 |
.038 |
-6.25 |
-.13 |
|




































