Open Access
Research Article
Max Screen
ISSN: 2639-930X
Copyright: © 2023 Motomi Ishibe. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Periprosthetic joint infection (PJI) following total hip arthroplasty (THA) is a serious complication. The debridement, antibiotic treatment, and implant retention (DAIR) procedure is considered the treatment of choice for acute PJI. This report describes the effectiveness of the DAIR procedures performed at our clinic. It was retrospectively reviewed that the outcomes of 13 patients who underwent DAIR due to PJI after primary THA. The DAIR procedure involved the debridement of unhealthy-looking tissue, irrigation with a massive amount of antibiotic-laden saline, and the exchange of the modular parts of the prosthesis. The average follow-up period after DAIR was 27 months. The interval between symptom onset and DIAR exceeded 4 weeks in two cases, which were both successfully treated. DAIR was performed twice in three cases with a mean interval of 9 days. The neck was exchanged in all seven cases that underwent THA using a modular-type neck, with all cases showing the successful control of infections. Overall, all 13 cases succeeded in infection control. A satisfactory success rate of infection control (100% (13/13)) was observed. The take-home message is that DAIR should be performed even if the interval between the infection onset and DAIR exceeds 4 weeks; moreover, it should be repeated if the first DAIR is insufficient for controlling the infection.
Keywords: Debridement; Antibiotic Treatment; Implant Retention; Periprosthetic Joint Infection; Total Hip Arthroplasty
List of Abbreviations:PJI: Periprosthetic joint infection; THA: Total hip arthroplasty; DAIR: Debridement, antibiotics, and implant retention; DM: Diabetes mellitus; CRP: C-reactive protein; ESR: Erythrocyte sedimentation rate OA: Osteoarthritis
Periprosthetic joint infection (PJI) after total hip arthroplasty (THA) is a serious complication. The incidence of PJI is 0.88%-2.22% and 4%-8% after primary and revision THA, respectively [1-4]. The treatment options for PJI include debridement, antibiotics, and implant retention (DAIR); one-stage exchange arthroplasty; two-stage arthroplasty; and resection arthroplasty. In the case of one-stage exchange arthroplasty, two-stage arthroplasty and resection arthroplasty, removal of a prosthesis firmly fixed to the bone may result in intra- and post-operative fractures. This makes the DAIR approach attractive, especially in the elderly.
DAIR mainly involves the debridement of infective and necrotic tissues, irrigation with large amounts of physiological saline, the simultaneous exchange of modular parts (liner, head, and neck if possible) of the prosthesis, and subsequent antibiotic administration, with confirmed stability with respect to the implant and sufficient soft tissue coverage [5]. DAIR is considered the treatment of choice for acute PJI occurring within 4 weeks after THA or the onset of symptoms [6-9]. According [10] there was no significant difference in the 1-year re-revision rate after a DAIR procedure by timing the DAIR procedure for THA based on Dutch registry data [10]. It remains unclear whether DAIR is effective for PJI symptoms that occur beyond 4 weeks after THA. In principle, DAIR was performed with the exchange of all removable prosthesis components in cases with infection symptoms after THA was performed at our clinic regardless of the duration between THA and the onset of infection. The aim of this retrospective study is to investigate the treatment outcomes of DAIR in our clinic and to determine whether DAIR is effective in treating PJI even in cases that take place more than four weeks after THA or/and after the onset of infection symptoms.
Between January 1, 2012, and February 28, 2021, 6,395 primary and revision THAs were performed in our clinic. Among them, 16 cases were diagnosed with PJI, with DAIR carried out in 13 cases. Figure 1 shows the study’s flowchart with respect to patient selection. PJI was diagnosed based on the 2018 International Consensus Meeting criteria for PJI [11].
DAIR involved reopening the joint; the debridement of unhealthy-appearing tissue; irrigation using 3-6 L of antibiotic-laden saline; and the exchange of the liner, head, and neck in case a modular-type stem was used. In all cases, the surgeons confirmed the stability of the prostheses, placed an intra-articular drain, and closed the joint. Intravenous and subsequent oral antibiotics were postoperatively administered for all patients.
The following factors were investigated; age; sex; genesis; the presence/absence of diabetes mellitus (DM); neck modularity; time of infection onset; causative organism; preoperative hematological findings; duration interval between the onset of infection and DAIR; the presence/absence and content of additional surgery; the period of intravenous and oral antibiotic administration; post-- DAIR follow-up period; the presence/absence of infection eradication; and the KLIC-score as a useful predictor of early failure after DAIR [12]. The onset of infection was defined as the emergence of hip pain or fever after a retrospective survey of the history of the patient. Infection eradication was defined as the absence of the use of antibiotics for > 1 month, a lack of clinical symptoms, and hematological normalization (C-reactive protein (CRP) levels < 1.0 mg/dl and erythrocyte sedimentation rate (ESR) at 1 h < 30 mm). Data analyses. Data were collected and analyzed by using Microsoft Excel (Microsoft Corporation, Redmond, Washington, USA). A univariate analysis with means for continuous variables and proportions for categorical variables were performed.
The average age of the 13 patients who developed PJI after primary THA and subsequently received DAIR was 58 years (range: 51-64 years). The average follow-up period after DAIR was 27 (9-82) months. There were nine male and four female patients. In all cases, the primary diagnosis was osteoarthritis (OA). Two cases presented with DM as a complication (Table 1)
A modular-type neck was used in seven cases. The average interval between THA and the onset of infection was 67 (14-485) days. This means that not all cases were postoperative acute, and they were also late acute. The identified microorganisms were Cutibacterium acnes, Staphylococcus aureus, and Staphylococcus epidermidis in one, eight, and two cases, respectively. Microorganisms were not detected in two cases. The average CRP level before DAIR was 10.6 mg/dl (range, 1.84-24.24), while the average ESR at 1h was 83.7 mm (range, 34-120 mm; data not acquired in two cases). The average interval between the onset of infection and DAIR was 26 days (range, 3-195 days). Three cases with local hip pain, surgical site swelling, local heat and redness, and high CRP levels after DAIR underwent additional DAIR within an average interval of 9 days (range, 7-12 days) after the first DAIR, which was considered insufficient to control the infection.
Regarding the antibiotics used postoperatively, levofloxacin, ciprofloxacin, cefotiam, clindamycin, and minocycline were intravenously administered. During the period of intravenous antibiotic administration, a hematological examination once or twice per week was performed; moreover, the antibiotics were changed to others to which causative microorganisms were sensitive toward in case the serum CRP, or the ESR levels did not improve. For the subsequent oral administration of antibiotics, levofloxacin, minocycline, and others were used in six, four, and three cases, respectively. The average period of postoperative antibiotic use was 36 (range, 15-54) and 86 (range, 20-210) days for intravenous and oral administration, respectively.
The KLIC-score was 2.5 in cases 2, 3, 5, and 7, however it was 0 in the other cases. Infection was observed to have been controlled
The following were the recommendations of “The Second International Consensus Meeting on Musculoskeletal Infection” conducted in Philadelphia in 2018:
The advantages of DAIR of the prosthesis include early postoperative and acute hematogenous PJI, which was defined as symptoms existing for ≤ 4 weeks, with the stability of the implant. KLIC and CRIME80 scores may aid in risk stratification.
The exchange of all modular components during DAIR reduces the risk of PJI recurrence. Early DAIR can be considered in case of acute infection following unicompartmental knee arthroplasty. However, in case the initial treatment effort causes failure or chronic infection, the implanted prosthesis should be removed, followed by a one-stage or two-stage conversion to total knee arthroplasty should be performed in combination with antibiotic therapy.
After a failed DAIR procedure, the removal of the components should be strongly considered.
The optimal length of antibiotic treatments following DAIR remains unclear since there is considerable heterogeneity regarding the length, dose, and administration of treatment. A minimum of 6 weeks of antibiotic therapy could be sufficient in most patients with PJIs undergoing DAIR-provided surgical treatment.
One-stage exchange arthroplasty remains a viable management option for chronic PJIs. However, it may not be suitable for patients with signs of systemic sepsis, extensive comorbidities, infection with resistant organisms, culture-negative infections, and poor soft tissue coverage [10].
In our study, a satisfactory rate of infection control (100% [13/13]) was observed compared to previous reports (16%-88%) [13-15]. Eleven patients who showed PJI after THA underwent DAIR within 4 weeks after infection onset, all of which lacked evidence of further or ongoing infection.
Cases 10 and 11 underwent DAIR > 4 weeks after infection onset. In case 10, low-grade fever persisted after THA. However, given the circumstances, including the transfer of the patient to another hospital, the diagnosis was significantly delayed, and DAIR was performed 195 days after the onset of the infection. Even with a significant delay in DAIR, infection recurrence was not allowed at 7 months after DAIR. Case 11 showed fever and hip pain 15 days after THA. DAIR, which was performed 36 days after infection onset, prevented infection recurrences within 3 months; however, this is still a short interval. The period from the onset of infection to debridement is among the determining factors for successful post-PJI debridement [16-18]. Although earlier debridement is better, there are often long intervals between the onset of infection and debridement for several reasons, including the diagnostic delay of infection, as in case 10. In these cases, it may be a heavy burden for patients to indicate prosthesis removal and one-or two-stage revision with respect to surgical invasion and medical costs. Our findings that infection control was achieved in cases that underwent DAIR beyond 4 weeks after the onset of infection are encouraging even though only two cases exhibited this. [16] reported a comparable infection sedative rate between DAIR and two-stage revision surgery; moreover, they showed that successful DAIR showed similar and superior functional results compared with initial THA and two-stage revision, respectively [19]. Given the aforementioned reports, unlike the above-mentioned consensus, we recommend that surgeons be allowed to perform DAIR for PJI cases > 4 weeks after the onset of infection at least once; however, it may have a lower success rate with respect to infection control.
Cases 7, 8, and 9 underwent additional DAIR after the first DAIR due to insufficient infection control. These cases finally showed no post-treatment infection recurrence. The above-mentioned consensus recommends removing the prosthesis if a single DAIR is unsuccessful. However, [16] reported performing DAIR in 122 PJI cases after THA, with 83 cases showing successful infection control. Repeated DAIR was performed in 32 of the remaining 39 failed cases, with successful infection control in 23 cases. Overall, successful infection control was achieved in 106 cases via a single or repeated DAIR [16]. Moreover, [18] reported that in 34 PJI cases, 28 and 6 hips required single and double debridement, respectively, to achieve infection control [18]. In our report, infection control was obtained in two out of three cases was obtained through repeated DAIR. Therefore, at least another debridement might be allowed if a single DAIR cannot sufficiently control infections.
According to [12], the failure rate in KLIC-scores 2 to 3.5 was 19.4%, whereas in this study all four cases in KLIC-scores 2 to 3.5 were cured of infection. Furthermore, infection control was achieved in all seven cases that were implanted with a Modulus stem (Lima, Udine, Italy), which comprises a cylindrical distal-fit type stem with a modular neck, followed by exchanging all feasible parts, including the neck, during DAIR. DAIR involving the replacement of modular parts has better outcomes than simple debridement [16,17, 20-24]. Moreover, we agree with the consensus of recommending the replacement of all exchangeable parts during debridement.
Furthermore, the effect of DAIR might be superior when the modular-type neck is exchanged than when only the liner and head are exchanged since the former allows more extensive irrigation and debridement. According to [25], late acute PJI, which was defined as the development of acute symptoms (≤ 3 weeks) occurring ≥ 3 months after arthroplasty, has a high failure rate. Although case 8 corresponds to late acute PJI in the present study, there was no recurrence of infection at the time of the follow-up visit. Our findings suggest that the indication of DAIR for PJI after primary THA could be extended. In particular, DAIR should be attempted at least once even in case of delayed DAIR after the onset of infection; however, the earlier it starts, the better. An additional implementation of DAIR should be affirmatively considered in the case of unsatisfactory results with respect to the first DAIR. The number of cases in this retrospective study is small; thus, future studies with a larger number of cases will be necessary.
This study reported the outcomes of 13 patients who developed a post-THA infection and underwent DAIR. Successful infection control was achieved in all 13 cases (100%), including 2 cases in which the interval between infection onset and DAIR exceeded 4 weeks. Furthermore, DAIR was performed in three cases without successful infection control after the first DAIR, resulting in successful outcomes in all three cases (100%). DAIR should be attempted at least once, even if the interval between the onset of infection and DAIR exceeds 4 weeks; moreover, it can be repeated if the first DAIR is insufficient in controlling the infection. Despite the small number of cases in this study, DAIR is a potentially viable procedure for the treatment of PJI, and there is a need to further identify how it should best be conducted and which patients benefit from it.

![]()

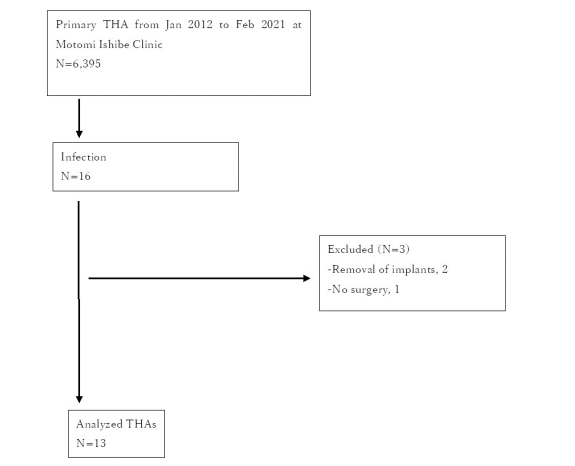 |
| Figure 1: Patient selection flowchart. THA, total hip arthroplasty |
Characteristics |
Total (N) |
Number of patients |
13 |
Mean age in years (range) |
58 (51 to 64) |
Number of male patients |
9 (69%) |
Number of female patients |
4 (31%) |
Diagnosis: Osteoarthritis |
13 |
Complication: DM DM, diabetes mellitus. |
2 (15%) |
Case No. |
stem |
Neck modularity |
Interval THA to symptoms (days) |
Organ ism |
Preoper ative CRP (mg/dl) |
Preoperative ESR at 1 h (mm) |
Interval symptoms to DAIR (days) |
Re-operation |
Antibiotic adminis tration (intravenous, days) |
Antibiotic admin istration (oral, days) |
Follow- up (months) |
Infec tion control |
KLIC-score |
1 |
Synergy |
Non-modular |
30 |
MSSE |
3.44 |
55 |
11 |
N/A |
cefotiam, 20 |
48 |
57 |
Yes |
0 |
2 |
Modulus |
Modular |
16 |
MSSA |
23.1 |
118 |
3 |
N/A |
cefotiam, 46 |
20 |
82 |
Yes |
2.5 |
3 |
Modulus |
Modular |
28 |
MSSA |
14.61 |
NA |
8 |
N/A |
ciprofloxacin, 41 |
60 |
70 |
Yes |
2.5 |
4 |
Synergy |
Non-modular |
14 |
Unknown |
2.73 |
64 |
19 |
N/A |
cefotiam, 54 |
99 |
29 |
Yes |
0 |
5 |
Bicontact |
Non-modular |
37 |
MSSA |
24.24 |
80 |
7 |
N/A |
levofloxacin, 50 |
46 |
10 |
Yes |
2.5 |
6 |
Modulus |
Modular |
77 |
MSSE |
5.11 |
97 |
11 |
N/A |
minocycline, 31 |
73 |
11 |
Yes |
0 |
7 |
Modulus |
Modular |
34 |
MSSA |
29.21 |
NA |
4 |
ID |
clindamycin, 46 |
169 |
28 |
Yes |
2.5 |
8 |
Accolade |
Non-modular |
485 |
MSSA |
1.84 |
120 |
7 |
ID |
clindamycin, 36 |
210 |
18 |
Yes |
0 |
9 |
Modulus |
Modular |
29 |
MSSA |
7.99 |
92 |
14 |
ID |
clindamycin, 54 |
123 |
13 |
Yes |
0 |
10 |
Modulus |
Modular |
32 |
Cutibac terium acnes |
2.99 |
34 |
195 |
N/A |
levofloxacin, 26 |
44 |
12 |
Yes |
0 |
11 |
Trifit |
Non-modular |
15 |
Unknown |
3.55 |
55 |
36 |
N/A |
cefotiam, 15 |
81 |
9 |
Yes |
0 |
12 |
Modulus |
Modular |
54 |
MSSA |
9.13 |
86 |
10 |
N/A |
levofloxacin, 29 |
85 |
9 |
Yes |
0 |
13 |
Trifit |
Non-modular |
19 |
MSSA |
10.31 |
120 |
13 |
N/A |
levofloxacin, 25 |
57 |
9 |
Yes |
0 |




































