Open Access
Research Article
Max Screen
ISSN: 2639-930X
Copyright: © 2021 Xue F. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background:The surgical treatment of OPLL is controversial.
Objectives:Herein, we aimed to compare the neurologic improvement, postoperative complications, and changes of Cobb’s angle between four main surgical approaches, including anterior cervical decompression and fusion (ACDF), laminoplasty (LAMP), laminectomy (LC), and anterior controllable antedisplacement and fusion (ACAF), to treat cervical ossification of posterior longitudinal ligament (OPLL).
Methods:We conducted a comprehensive literature search in four electronic databases (PubMed, Embase, Medline and the Cochrane Library). The enrolled randomized or non-randomized controlled studies were published before April 2021, comparing at least two surgical techniques, including ACAF, ADF, LAMP, or LC for OPLL treatment. The quality of the included articles was evaluated according to Newcastle-Ottawa Scale. The main outcome measures comprised: improvement rate (IR) of Japanese Orthopedic Association (JOA) score, postoperative Cobb’s angle changes and complications. Besides, subgroup analysis was performed based on the occupied rate (≥50%) and affected segments (≥3).
Results: A total of 23 studies containing 1847 patients were enrolled in this network meta-analysis. In terms of IR of JOA, the anterior approaches were superior to the posterior approaches. As for the postoperative complications, the ADF ranked first (93%) with the highest rates of complications, while ACAF ranked fourth place (71%). Regarding Cobb’s angle changes, ACAF exhibited the best outcome. As for the high occupied rate (≥50%), ACAF and ADF demonstrated similar IR of JOA and LC, and LAMP ranked third (73%) and fourth (81%). Regarding multi-levels (≥3), ACAF presented advantage over LC and LAMP without statistical significance.
Conclusion: ADF and ACAF showed advantage over LC and LAMP of higher IR of JOA. ACAF was associated with a significantly lower incidence of postoperative complications. For the high occupied rate (≥50%), the clinical outcome was similar above. Regarding multi-levels (≥3), ACAF may play a better role on IR of JOA than LC and LAMP.
Keywords: OPLL; Surgical Approaches; Network Meta-Analysis; Clinical Outcome
Ossification of the posterior longitudinal ligament (OPLL) is a chronic condition that results in progressive myelopathy [1,2]. When OPLL is left untreated, it may ultimately lead to neurologic morbidity and a significant loss of independence [3]. It is significantly influenced by geographic location and ethnicity, with the highest reported prevalence in East Asian countries [4], with a cervical OPLL prevalence of 4.1-6.3% [5-7].
Surgical intervention has significantly improved the clinical prognosis of most myelopathy patients owing to OPLL[8]. Patients with OPLL managed conservatively were found to have a significantly higher cumulative incidence of hospitalization for spinal cord in- jury than matched controls [9]. Several traditional surgical techniques have been applied to treat OPLL, including anterior cervical decompression and fusion (ACDF), laminoplasty (LAMP) and laminectomy (LC) with or without fusion.
Numerous studies, including clinical trials and meta-analyses, have focused on comparing the clinical outcomes of such surgical approaches [10-13]. However, it appears that they disagreed on the choice of surgical approach for different patients. One new tech- nique is referred to as anterior controllable antedisplacement and fusion (ACAF), first described by Lee et al. [14] and Miao et al. [15] This technique comprises four main procedures, as shown in supplementary material 1: (1) discectomy and anterior vertebral body resection of the involved levels; (2) placement of intervertebral grafts and an anterior plate to the vertebrae-OPLL complex (VOC); (3) bilateral osteotomies performed at the widest portion of the multilevel OPLL mass to mobilize and isolate the VOC; and (4) the VOC being “hoisted” off the spinal cord by tightening of the cage screws. Illustrations of the surgical technique are available in supplementary material 8. This technique enables multilevel decompression to be accomplished with an anterior approach without direct manipulation of the OPLL mass. Recent studies have demonstrated the advantages of the novel technique over other approach- es for better neurologic improvement and lower complication rates [16-21].
Network meta-analysis allows for a more integrated analysis [22]. Network meta-analyses of existing datasets make it possible to estimate the comparative efficacy, summarize and interpret the wider picture of the evidence base, and understand the relative merits of multiple interventions [23]. Therefore, herein, we aimed to conduct a systematic review and network meta-analysis to compare the clinical outcomes of four surgical techniques for cervical OPLL, including IR of JOA, changes of Cobb’s angle, and postoperative complications.
This systematic review and network meta-analysis followed the most recent version of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for network meta-analysis.
Studies were eligible for inclusion if they met the following criteria:
Patients: diagnosed with cervical myelopathy due to OPLL and indicated for surgery;
Intervention and control: comparison of at least two surgical approaches, including ACAF, ACDF, LAMP or LC; Clinical outcome: IR of JOA, Cobb’s angle changes or postoperative complications;
Follow-up time: at least 6 months;
Study design: randomized controlled trials (RCTs) or non-RCTs.
The studies were excluded if they met the following criteria: animal studies, biomechanical studies, duplicate publications of one trial, case report, letter, revision, technology note, thoracic OPLL, commentaries, reviews and meta-analyses.
We searched for English articles in PubMed, EMBASE, Medline, and the Cochrane Library using the following keywords: ((ossifi- cation of posterior longitudinal ligament) or (ossified posterior longitudinal ligament) or (calcification of the posterior longitudinal ligament)) and ((anterior decompression and fusion) or (anterior cervical corpectomy with fusion) or (laminoplasty) or (laminecto- my) or (anterior controllable antedisplacement fusion) or (vertebral body sliding osteotomy)). All databases were searched from the date of inception through April 2021.
Two authors (TY.Z and XF.C) independently assessed potential articles for eligibility using the aforementioned criteria. Differences were resolved by discussion with another senior author (F.X. Prof.) Data were independently extracted by two reviewers (WY.X and SZ.Z) and reviewed by another senior author (F.X. Prof.).
The extracted data included the author, year of publication, intervention type, number of patients in each arm, mean patient age, affected segments, and occupied rate. Our clinical outcomes comprised IR of JOA, Cobb’s angle changes, or postoperative compli- cations.
The occupied rate is defined as the thickness of the OPLL divided by the anteroposterior diameter of the bony spinal canal on an axial CT image [21] or X-ray [24].
As all studies included were nonrandomized controlled studies, the Newcastle-Ottawa Scale was employed to assess the quality of each study. This scale allocated a maximum of nine points for the risk of bias in three domains: (1) selection (four points), (2) com- parability (two points), and (3) exposure and outcomes (three points). A study that scored 6 or more was eligible for data pooling and one that scored 7 or more was considered high quality[11]. The evaluation process was independently conducted by two reviewers (SZ.Z and WY.X), and all discrepancies were resolved by discussion with another senior author (F.X. Prof).
First, we performed a pairwise meta-analysis using a random-effects model in STATA (v15.0). The treatment effects were calculated as odds ratios (ORs) for dichotomous outcomes and standardized mean differences (SMDs) for continuous outcomes with 95% confidence intervals (CIs). We assessed statistical heterogeneity in each pairwise comparison with the I2 statistic and P-value. If sig- nificant heterogeneity (I2>50%) was detected among the included studies, we performed sensitivity analysis or subgroup analysis to explore the cause of the heterogeneity.
Second, STATA and ADDIS were deployed to run the network meta-analysis. ADDIS is an evidence-based decision support system that was developed by Valkenhoef G et al. and is based on Bayesian theory. Four independent Markov chains were auto- matically generated to obtain a posterior distribution and were run for 20,000 tuning iterations and 50,000 simulation iterations per chain. Run lengths were extended if Brooks-Gelman-Rubin diagnostic or time series plots indicated that the Markov chains had not converged [25].
The model’s inconsistency was assessed by inconsistency factors, variance calculation [26] and node-splitting analysis [27]. If the data were consistent, the inconsistency factors would be close to 0 so that the 95% Cl for an inconsistency factor did not contain the neutral value (zero), which clearly indicated inconsistency. If there was no inconsistency, the random-effects variance and incon- sistency variance would be roughly equal. If the data were inconsistent, the random-effects variance would be expected to decrease significantly from the consistency model to the inconsistency model
The occupied rate and affected segments often influence the clinical decisions of orthopaedic surgeons. Therefore, we preplanned a subgroup meta-analysis according to the occupied rate (≥50%) and affected segment (≥3).
Our search identified 2596 citations, and 721 potentially eligible articles were retrieved in full text (Figure 1). In the end, we included 23 reports published between 2001 and 2020, comprising a mean number of patients per study of 80 (range, 26-252). Across the trials, the mean age of the patients ranged from 45.9 to 65.8 years. In total, 1847 patients were included in our analysis; the details of each study are presented in Table 1, and a network of eligible comparisons is presented in Figure 2.
Since all studies involved were nonrandomized controlled studies, the Newcastle-Ottawa Scale was deployed to assess the quality of each study. Among the 23 included studies, one obtained 6 points on the NOS, seven studies acquired 7 points, and the other 15 received more than 7 points. The quality assessment of the included studies is summarized in supplementary material 1.
The outcomes of pairwise comparisons are summarized in supplementary material 2. The heterogeneity of some pairwise meta-anal- yses was not satisfactory but acceptable. The pairwise comparison showed no statistically significant difference between every two approaches in the IR of JOA, the postoperative complications and Cobb’s angle changes.
The results of the network meta-analysis for IR of JOA, postoperative complications and Cobb’s angle are summarized in Table 2. Regarding IR of JOA, the anterior approaches were obviously better than the posterior approaches, and no significant difference was found between ACAF and ACDF. Regarding the postoperative complications, ACAF and LAMP had a significantly lower risk than ACDF, with RRs of 0.18 and 0.28, respectively. Meanwhile, ACAF had a much better advantage in improving postoperative changes in Cobb’s angle than the other three approaches.
The ranking of treatments is presented in Table 3. For the IR of JOA, ACAF and ACDF shared the same probability of ranking first (50%, 50%), while LC and LAMP ranked third and fourth (70%, 71%), respectively. Regarding the postoperative complications, the worst treatment was ACDF (93%). LC and LAMP ranked second and third (69%, 61%), respectively, while ACAF had the lowest ranking (71%). Regarding the postoperative change in Cobb’s angle, ACAF was the best surgical approach (100%), ACDF was the second-best (82%), and LC and LAMP ranked third and fourth (73%, 89%), respectively.
The evaluation of inconsistency factors and variance calculation presented no apparent inconsistency in the outcomes (supple- mentary material 3 and supplementary material 4). The results of the node-splitting test also found no inconsistency between any comparison pairs (supplementary material 5).
The extent of OPLL disease (number of levels involved) and the occupied rate are the two main factors that will be considered during approach selection by orthopaedic doctors. Therefore, we conducted a subgroup analysis according to the occupied rate (supple- mentary material 6) and affected segments (supplementary material 7). For the high occupied rate (≥50%), the anterior approaches were superior to the posterior approaches. ACDF was the best surgical approach (57%), ACAF was the second best (50%), and LC and LAMP ranked third and fourth (73%, 81%), respectively. Regarding multilevels (≥3), no significant difference was found among ACAF, LAMP and LC. The rank probability outcome demonstrated that ACAF was the best surgical approach (70%), LC was the second-best (53%), and LAMP had the lowest ranking (68%).
In this systematic review and network meta-analysis, we enrolled 23 cohort studies involving 1847 OPLL patients undergoing surgery, including ACAF, ACDF, LAMP, and LC. Most included studies (22/23) were classified to be of high quality according to the Newcastle-Ottawa Scale. We evaluated the effects of the four surgical approaches on OPLL patient prognosis based on postoperative Cobb’s angle changes, postoperative complications, and IR of JOA. Meanwhile, we conducted a subgroup analysis of the occupied rate and affected segments.
According to the network meta-analysis and IR of JOA, the anterior approaches displayed great advantages over the posterior ap- proaches. In the rank probability analysis, the probability of ACAF and ACDF ranking first was 50%, while LC and LAMP ranked third and fourth, respectively. In the subgroup analysis of high occupied rate (≥50%), compared with LAMP, ACAF and ACDF had a higher IR of JOA with statistical significance. ACDF, ACAF, LC and LAMP ranked first, second, third and fourth, with probabil- ities of 57%, 50%, 73%, 81%, respectively. In the subgroup analysis of multilevels (≥3), ACAF was the best approach, while LC and LAMP ranked second and third, respectively. These results were consistent with some other meta-analyses [11,28].
The primary goal of surgical management of OPLL is to relieve neural compression by either (1) direct resection or thinning of the ossified mass or (2) expansion of the spinal canal to accommodate OPLL lesions [4]. ACDF could relieve spinal cord compression by direct resection or thinning of the ossified mass. LAMP or LC could relieve ossified ligament compression by passively expanding the spinal canal volume through the posterior approach. On the other hand, ACAF could actively move vertebral bodies and ossified ligaments through the anterior approach to actively relieve neural compression. Therefore, the anterior approaches were superior to the posterior approaches from a decompression perspective. The indirect decompression impact by posterior approaches was inversely correlated with the occupied rate, which affects the neurologic recovery prognosis. Meanwhile, some studies stated that postoperative progression of ACDF was significantly reduced with LAMP or LC due to direct resection [29], and the posterior ap- proaches are associated with more reoperations.
ACDF ranked first with a 93% possibility regarding postoperative complications, while LC and LAMP ranked second and third, respectively. ACAF had the lowest rates of postoperative complications. Postoperative complications were common, ranging from 9.7-65.4% [30,31]. The overall incidence of surgical complications of cervical OPLL was 21.8% according to a literature review [32]. The common complications include cerebrospinal fluid leakage, C5 palsy, axial neck pain, recurrent laryngeal nerve injury, haema- toma, hardware complications, neurologic deficit and surgical site infection. Because the surgical approach to ACDF enters from the anterior side of the neck, it will sometimes damage the recurrent laryngeal nerve, leading to dysphagia, dysarthria, and hoarseness. Meanwhile, ACDF may tear the dura because of direct resection when the ossified ligament is close to the spinal dura or associated with the dura’s ossification. Although the aetiology of so-called postoperative “C5 palsy” has yet to be definitively established, it is a phenomenon that is widely acknowledged after cervical spine surgery, especially for posterior approaches[32]. ACAF, due to ante- rior approaches, can avoid C5 palsy to a great extent. Simultaneously, ACAF will not directly resect the ossified ligament, reducing cerebrospinal fluid leakage.
Regarding Cobb’s angle changes, the anterior approaches were significantly superior to the posterior approaches, which could re- store cervical lordosis, reduce the incidence of postoperative kyphosis deformity, and improve spinal stability.
Several limitations were found for this network meta-analysis. First, since ACAF was proposed in the last two years, very few studies have compared ACAF with other surgical approaches, preventing us from including more studies in the pairwise analysis. Consequently, more clinical studies are required on ACAF in the future. Second, the postoperative complications of the anterior and posterior surgical ap- proaches were quite different, and the treatment and prognosis of different complications were dissimilar, so our study on complications was quite general. In future meta-studies, postoperative complications should be classified more carefully to guide clinical practice. Third, we ignored the impact of different radiological subsets of OPLL on surgical outcomes due to the limitations of the original literature.
The anterior approaches showed a significant advantage over the posterior approaches, with statistical significance regarding IR of JOA and maintaining cervical lordosis, regardless of the occupied rate. Simultaneously, ACAF was linked to a significantly lower incidence of postoperative complications than the other three techniques. Regarding multilevel OPLL, ACAF was better than LAMP and LC.
According to the latest guidelines of the International Committee of Medical Journal Editors, all authors listed meet the authorship criteria, and they agree with the manuscript.
This study was funded by Ministry of Education Key Laboratory of trauma treatment and nerve regeneration.
The authors declare no conflicting interests.
The datasets generated and analyzed during the current study are not publicly available due to the data also forms part of an ongoing study but are available from the corresponding author on reasonable request.
Stata Statistical Software 15 (StataCorp., T.X.,USA)
ADDIS V1.16.8
Not applicable.
Not applicable.
Not applicable.
DY.Z and BG.J were responsible for the study design. SZ.Z, WY.X, XF.C and TY.Z contributed to the acquisition and analysis of data. WY.X, SZ.Z and F,X contributed to the interpretation and analysis of data. SZ.Z were responsible for drafting the article. WY.X and F.X were responsible for revising it critically for important intellectual content. DY.Z and BG.J have approved the version to be pub- lished and all subsequent versions. SZ.Z and WY.X were major contributors and should be listed as to co-first authors.

![]()

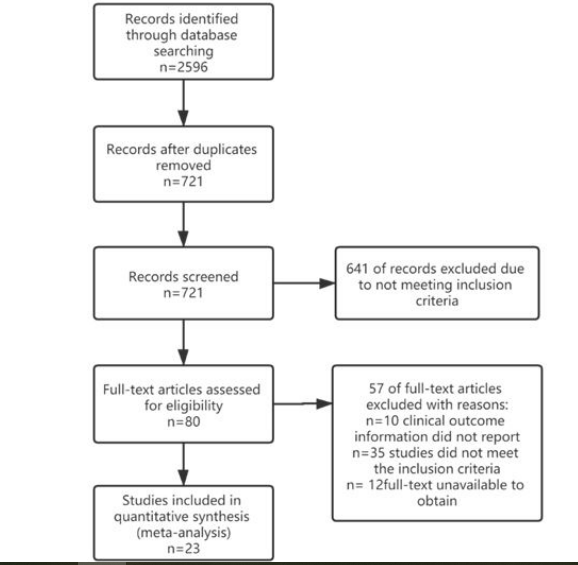 |
| Figure 1: Study selection using PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) guidelines. |
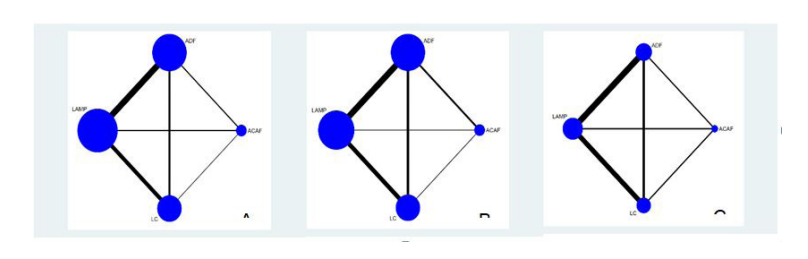 |
| Figure 2: Network of eligible comparisons for IR of JOA (A) postoperative complications; (B) Cobb's angle changes; (C) The lines' width is proportional to the number of trials comparing every pair of treatments, and the size of every circle is proportional to the number of randomly assigned participants (sample size) |
Study ID |
Surgical Appr oach |
Male/ Female |
Age (Mean |
Affected Segments |
Occupied Rate |
Sam ple Size |
IR of JOA |
Post operative Compli cations |
Cobb's Angle |
Time Points |
Type of OPLL (N) |
|||
Conti nuous |
Mixed |
Segm ental |
Circum scribed |
|||||||||||
2002 Tani[30] |
ACDF |
11/3 |
61.5±11.4 |
NA |
≥50% |
14 |
58.0±24.0 |
9 |
NA |
49.1m |
NA |
NA |
NA |
NA |
LAMP |
9/3 |
65.8±6.1 |
NA |
≥50% |
12 |
13.0±39.0 |
8 |
NA |
50.3m |
NA |
NA |
NA |
NA |
|
2007 |
ACDF |
15/12 |
58±NA |
NA |
56.6±NA |
27 |
51.0±26.7 |
8 |
NA |
6.0y |
14 |
7 |
2 |
4 |
LAMP |
51/15 |
57±NA |
NA |
44.4±NA |
66 |
54.0±27.7 |
1 |
NA |
10.2y |
20 |
36 |
7 |
3 |
|
2007 |
ACDF |
14/5 |
51.8±6.6 |
2.5±1.1 |
56±8 |
19 |
68.4±27.3 |
NA |
NA |
>12m |
NA |
NA |
NA |
NA |
LAMP |
30/10 |
62.6±10.3 |
4.1±1.3 |
55.9±14.3 |
40 |
52.5±30.0 |
NA |
NA |
>12m |
NA |
NA |
NA |
NA |
|
2011 Chen[34] |
ACDF |
14/8 |
57.2±NA |
3.3±0.3 |
55.4±8.2 |
22 |
63.2±15.2 |
5 |
NA |
>4y |
NA |
NA |
NA |
NA |
LAMP |
16/9 |
54.2±NA |
3.7±0.2 |
54.3±4.6 |
25 |
25.1±8.5 |
8 |
NA |
>4y |
NA |
NA |
NA |
NA |
|
LC |
19/9 |
55.3±NA |
3.5±0.2 |
58.2±6.4 |
28 |
43.5±12.7 |
7 |
NA |
>4y |
NA |
NA |
NA |
NA |
|
2012 Chen[35] |
ACDF |
63/28 |
48.7±1.4 |
2.7±0.2 |
43.6±1.1 |
91 |
68.0±2.7 |
16 |
NA |
>12m |
NA |
NA |
NA |
NA |
LAMP |
33/8 |
46.3±2.5 |
4.1±0.2 |
41.2±1.4 |
41 |
65.2±5.8 |
7 |
NA |
>12m |
NA |
NA |
NA |
NA |
|
LC |
19/13 |
52.6±1.7 |
4.2±0.1 |
47.1±1.1 |
32 |
50.8±6.4 |
12 |
NA |
>12m |
NA |
NA |
NA |
NA |
|
2012 Sakai[29] |
ACDF |
NA |
59.5±9.3 |
NA |
43.4±16.6 |
20 |
71.4±26 |
5 |
4.7±11.1 |
>5y |
NA |
NA |
NA |
NA |
LAMP |
NA |
58.4±9.6 |
NA |
46.9±16.1 |
22 |
55.3±29.6 |
0 |
5.6±11.3 |
>5y |
NA |
NA |
NA |
NA |
|
2013 |
ACDF |
36/32 |
54.4±12.8 |
NA |
NA |
68 |
80.6±9.7 |
5 |
NA |
>5y |
NA |
NA |
NA |
NA |
LAMP |
25/34 |
57.9±9.5 |
NA |
NA |
59 |
55.7±13.9 |
3 |
NA |
>5y |
NA |
NA |
NA |
NA |
|
2014 |
ACDF |
7/5 |
58.7±9.1 |
5.4±1.2 |
≥60% |
12 |
52.5±18.5 |
7 |
1.2±9.5 |
9.9y |
6 |
5 |
0 |
1 |
LAMP |
12/3 |
55.6±7.8 |
3.3±0.9 |
≥60% |
15 |
30.1±30.5 |
5 |
-7.2±7 |
10.9y |
4 |
10 |
0 |
1 |
|
2015 |
ACDF |
51/20 |
57.3±NA |
NA |
31.7±75.3 |
71 |
72.6±38.2 |
NA |
NA |
48m |
11 |
19 |
9 |
32 |
LAMP |
49/15 |
56.4±NA |
NA |
27.7±78.2 |
64 |
51.9±66.3 |
NA |
NA |
41m |
22 |
25 |
16 |
1 |
|
2015 Yuan[39] |
LAMP |
14/6 |
59±11.6 |
≥3 |
NA |
20 |
43.7±10.1 |
4 |
NA |
12m |
10 |
7 |
3 |
0 |
LC |
11/7 |
62±13.1 |
≥3 |
NA |
18 |
50.8±11.2 |
6 |
NA |
12m |
10 |
6 |
2 |
0 |
|
2016 Koda[40] |
ACDF |
10/5 |
57.7±NA |
NA |
43.8±96.7 |
15 |
72.5±28.6 |
14 |
-2.6±3.5 |
>12m |
NA |
NA |
NA |
NA |
LAMP |
12/4 |
60.3±NA |
NA |
43.5±90 |
16 |
14.4±37.1 |
1 |
-4.4±9.0 |
>12m |
NA |
NA |
NA |
NA |
|
LC |
14/3 |
65.0±NA |
NA |
34.1±92.7 |
17 |
43.6±20.2 |
2 |
0.8±9.2 |
>12m |
NA |
NA |
NA |
NA |
|
2016 Yoshii[41] |
ACDF |
31/8 |
61.1±8.5 |
2.7±1 |
58.8±8.3 |
39 |
61.6±28.2 |
24 |
4.1±7.1 |
44.5m |
NA |
NA |
NA |
NA |
LC |
18/4 |
60.6±12.8 |
3.4±1.1 |
57.1±7.2 |
22 |
55.8±18.2 |
5 |
0.2±6.2 |
37.2m |
NA |
NA |
NA |
NA |
|
2017 Huo[42] |
ACDF |
86/64 |
47.8±NA |
NA |
61.9±9.1 |
150 |
NA |
62 |
6.7±11.5 |
35.4m |
23 |
41 |
19 |
67 |
LAMP |
61/41 |
45.9±NA |
NA |
63.4±8.9 |
102 |
NA |
50 |
3.1±12.4 |
36.1m |
43 |
53 |
34 |
2 |
|
2017 |
LAMP |
26/6 |
59±10 |
≥3 |
49±12 |
32 |
46.3±15.8 |
10 |
-0.6±4.1 |
38m |
17 |
10 |
5 |
0 |
LC |
25/10 |
60±8 |
≥3 |
50±11 |
35 |
52.0±15.3 |
23 |
4.3±2.6 |
42m |
15 |
14 |
6 |
0 |
|
2017 |
LAMP |
30/8 |
60.9±8.5 |
≥3 |
NA |
35 |
38.8±18.3 |
5 |
6.6±13.4 |
35.2 |
NA |
NA |
NA |
NA |
LC |
25/10 |
64.6±10.6 |
≥3 |
NA |
38 |
46.3±23.9 |
4 |
-5.8±8.8 |
30.9 |
NA |
NA |
NA |
NA |
|
2018 Yang[21] |
ACAF |
21/13 |
58.4±8.3 |
2-4 |
83.2±13.7 |
34 |
80.9±8.9 |
2 |
NA |
10.1 |
NA |
NA |
NA |
NA |
ACDF |
19/17 |
58.6±10.8 |
1-3 |
74.5±10.2 |
36 |
70.1±20.7 |
8 |
NA |
12.4 |
NA |
NA |
NA |
NA |
|
2019 |
LAMP |
36/6 |
62.2±7.8 |
4-5 |
19.5±11.2 |
49 |
55.3±18.0 |
7 |
3.8±6.4 |
>24m |
11 |
24 |
14 |
0 |
LC |
33/16 |
59.1±8.5 |
4-5 |
53.8±12.2 |
42 |
47.8±24.0 |
8 |
7.2±8.5 |
>24m |
8 |
18 |
16 |
0 |
|
2019 |
ACAF |
19/5 |
56.3±10.6 |
1-3 |
54±15 |
24 |
NA |
2 |
9.8±7.5 |
>12m |
NA |
NA |
NA |
NA |
ACDF |
28/10 |
53.8±10.1 |
1-4 |
47±10 |
38 |
NA |
16 |
3.3±4.6 |
>12m |
NA |
NA |
NA |
NA |
|
2019 |
ACAF |
27/11 |
58.2±1.8 |
NA |
≥60% |
38 |
78.6±3.4 |
3 |
8.4±0.8 |
>12m |
NA |
NA |
NA |
NA |
LC |
22/11 |
58.1±2.3 |
NA |
≥60% |
33 |
64.5±3.0 |
5 |
-0.9±0.4 |
>12m |
NA |
NA |
NA |
NA |
|
2019 |
ACAF |
23/18 |
57.2±12.2 |
3-5 |
NA |
42 |
67.5±18.8 |
NA |
NA |
18.2m |
NA |
NA |
NA |
NA |
LAMP |
19/19 |
58.1±13.4 |
3-5 |
NA |
38 |
58.7±14.7 |
NA |
NA |
17.7m |
NA |
NA |
NA |
NA |
|
2019 |
ACDF |
12/5 |
55.2±12.1 |
1.2±0.4 |
37.5±12.4 |
17 |
59.9±33.8 |
4 |
-1.3±6.2 |
3.5y |
2 |
0 |
9 |
6 |
LAMP |
25/8 |
54.8±10.7 |
4.1±0.6 |
40.8±8 |
33 |
35.8±35.3 |
6 |
-1.9±6.4 |
4.5y |
6 |
6 |
13 |
8 |
|
2019 Yang[17] |
ACAF |
17/11 |
58.0±9.9 |
1-4 |
54.2±7.7 |
28 |
82.4±8.8 |
1 |
NA |
>6m |
7 |
11 |
10 |
0 |
ACDF |
21/10 |
58.7±7.9 |
1-3 |
51.5±11.2 |
31 |
71.9±12.4 |
7 |
NA |
>6m |
10 |
8 |
13 |
0 |
|
2020 Chen[16] |
ACAF |
23/16 |
54.6±11.2 |
3.8±0.4 |
72.4±17.6 |
39 |
60.1±9.2 |
15 |
6.9±6 |
>12m |
19 |
17 |
3 |
0 |
LAMP |
20/18 |
57.2±10.4 |
4.1±0.5 |
69.8±16.4 |
38 |
51.3±10.6 |
13 |
-8.8±7.1 |
>12m |
20 |
16 |
2 |
0 |
|
IR of JOA |
|||
ACAF |
-0.02 (-12.19, 13.03) |
-18.25 (-30.62, -5.82) |
-15.85 (-29.21, -2.49) |
0.02 (-13.03, 12.19) |
ADF |
-18.31 (-26.61, -10.66) |
-15.88 (-26.02, -6.14) |
18.25 (5.82, 30.62) |
18.31 (10.66, 26.61) |
LAMP |
2.41 (-6.32, 11.47) |
15.85 (2.49, 29.21) |
15.88 (6.14, 26.02) |
-2.41 (-11.47, 6.32) |
LC |
Postoperative Complications |
|||
ACAF |
5.55 (1.40, 24.34) |
1.59 (0.35, 7.04) |
2.48 (0.51, 11.89) |
0.18 (0.04, 0.71) |
ADF |
0.28 (0.11, 0.67) |
0.45 (0.14, 1.28) |
0.63 (0.14, 2.85) |
3.52 (1.49, 9.09) |
LAMP |
1.57 (0.58, 4.24) |
0.40 (0.08, 1.97) |
2.23 (0.78, 7.15) |
0.64 (0.24, 1.72) |
LC |
Cobb's Angle |
|||
ACAF |
-9.95 (-16.41, -3.60) |
-14.93 (-21.42, -8.74) |
-12.22 (-18.76, -5.90) |
9.95 (3.60, 16.41) |
ADF |
-4.95 (-9.28, -0.70) |
-2.25 (-7.33, 2.72) |
14.93 (8.74, 21.42) |
4.95 (0.70, 9.28) |
LAMP |
2.70 (-1.94, 7.23) |
12.22 (5.90, 18.76) |
2.25 (-2.72, 7.33) |
-2.70 (-7.23, 1.94) |
LC |
Items |
treatment |
Rank 1 |
Rank 2 |
Rank 3 |
Rank 4 |
IR of JOA |
ACAF |
0.5 |
0.49 |
0.01 |
0 |
ADF |
0.5 |
0.5 |
0 |
0 |
|
LAMP |
0 |
0 |
0.29 |
0.71 |
|
LC |
0 |
0.01 |
0.7 |
0.29 |
|
Postoperative Complications |
ACAF |
0.01 |
0.1 |
0.18 |
0.71 |
ADF |
0.93 |
0.07 |
0 |
0 |
|
LAMP |
0 |
0.15 |
0.61 |
0.24 |
|
LC |
0.06 |
0.69 |
0.2 |
0.05 |
|
Cobb's Angle |
ACAF |
1 |
0 |
0 |
0 |
ADF |
0 |
0.82 |
0.17 |
0.01 |
|
LAMP |
0 |
0.01 |
0.1 |
0.89 |
|
LC |
0 |
0.17 |
0.73 |
0.1 |




































