Open Access
Research Article
Max Screen
ISSN: 2639-930X
Copyright: © 2021 Nakanowatari T. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Purpose: Early rehabilitation after bipolar hemiarthroplasty (BHA) requires risk management for postoperative dislocation. Since April 2018, BHA has been performed at our hospital using a conjoined tendon-preserving posterior (CPP) approach, which preserves the piriformis and short rotator muscles (the gemellus superior, the obturator internus and the gemellus inferior) and dissects only the external obturator. Early rehabilitation for inpatients after BHA with CPP is conducted under precaution-free management for dislocation. The purpose of this study was to compare early post-surgery rehabilitation outcomes under precaution-free management for dislocation after BHA with CPP versus precautionary management for dislocation after conventional BHA
Methods: Data from a retrospectively reviewed, single institutional database of patients undergoing BHA after femoral neck fracture were utilized. A total of 35 patients who underwent BHA with the conventional posterior approach (control group) between April 2017 and March 2018, and 35 patients who underwent BHA with the CPP approach between April 2018 and March 2019 (CPP group), were continuously enrolled. Postoperative rehabilitation was conducted with protection of the hip joint to prevent dislocation in the control group, whereas no precautions for dislocation, as with rehabilitation after internal fixation of hip fractures, were taken in the CPP group. Rehabilitation outcomes were measured using the ability for basic movement scale II (ABMS II) and Barthel Index (BI) at the beginning of rehabilitation and at discharge. Linear mixed model (LMM) in split-plot analysis of variance (ANOVA) was used to determine the effect of group (CPP or control) and rehabilitation stage (beginning or end) on ABMS II and BI. A post-hoc Bonferroni’s multiple comparison test was used for statistical analysis.
Results: We found main effects of group (p < 0.001) and rehabilitation stage (p < 0.001) on ABMS II, but no interactive effect between them on ABMS II and BI. The estimated mean of ABMS II at the beginning and at discharge in the CPP group was significantly higher than in the control group (estimated mean difference, 2.8; 95% confidence interval: 0.9, 4.7; p = 0.005).
Discussion: BHA inpatients with CPP had better basic mobility function than conventional BHA inpatients in the acute postoperative phase. Precaution-free management for dislocation accompanied by surgical techniques for preserving hip external rotator tendons, such as CPP, might enhance the recovery process and improve early rehabilitation after BHA.
Keywords: Hip Hemiarthroplasty; Hip Precaution; Outcomes; Rehabilitation
Most elderly patients with displaced femoral hip fractures are treated with bipolar hemiarthroplasty (BHA) [1,2]. Early rehabilitation after BHA requires risk management for prevention of postoperative dislocation. Post-BHA patients are commonly prescribed movement restriction and mandatory use of protective devices to reduce the risk of dislocation [3]. However, such precautions are reportedly associated with a slower recovery process during rehabilitation in patients with BHA [4], and slower return to activities of daily living (ADL) and less satisfaction in patients with total hip arthroplasty (THA) [5].
The dislocation risk is reportedly influenced by the surgical technique use for BHA [6-8]. Using surgical approaches that preserve soft tissue during BHA is one of the key factors for reducing the dislocation risk. Recently, several surgical approaches to THA, such as the piriformis tendon preservation technique [9] and preservation of the external rotator from the piriformis muscle to the internal obturator muscle [10] have been reported as soft tissue preserving procedures.
Since April 2018, BHA has been performed at our hospital using a conjoined tendon-preserving posterior (CPP) approach, which preserves the piriformis and short rotator muscles (the gemellus superior, the obturator internus and the gemellus inferior) and dissects only the external obturator. Tetsunaga et al. [11] reported that patients who underwent BHA with CPP had excellent stability of the hip and no postoperative dislocation. We conduct hip precaution-free management for dislocation in the early rehabilitation period after BHA with CPP. Jobory et al. [12] reported that the rehabilitation personnel without precautions would use significantly less work effort during hospital stay. Therefore, we hypothesized that precaution-free rehabilitation after BHA with CPP enhances the recovery process, resulting in favorable motor function outcomes. The purpose of this study was to compare early post-surgery rehabilitation outcomes under precaution-free management for dislocation after BHA with CPP versus precautionary management for dislocation after BHA by the conventional approach.
Data from a retrospective, single institutional review of the medical records of patients undergoing BHA after femoral neck fracture were utilized. This clinical study was approved by the review board of the hospital. It is in agreement with the ethical guidelines of the Declaration of Helsinki and written Informed consent from all patient were obtained in accordance with the local ethical committee. A total of 37 patients who underwent BHA with the conventional posterior approach (control group) between April 2017 and March 2018, and 49 patients who underwent BHA with the CPP approach between April 2018 and March 2019 (CPP group), were continuously enrolled. Two patients in the control group who had postoperative dislocation while still in the hospital were excluded from this study. Fourteen patients in the CPP group who were managed taking precautions for dislocation were excluded from this study. No patients in the CPP group had postoperative dislocation (Figure 1).
All patients in both groups underwent rehabilitation under the guidance of a physical therapist, with weight-bearing being introduced gradually after surgery. In control group patients, a pillow was used to prevent hip adduction when patient was in the supine position, lying laterally or sitting in a wheelchair until they acquired independent walking, while this was not used for patients in the CPP group. Rehabilitation for patients in the control group was conducted under precautions to prevent dislocation by avoiding adduction and internal rotation of the hip motion. On the other hand, rehabilitation for patients in the CPP group did not involve any precautions for dislocation, as with standard rehabilitation after internal fixation of hip fractures.
For all patients, the revised version of the Ability for Basic Movement Scale (ABMS II) [13] was used to evaluate their basic mobility function. The ABMS II includes five items: “turning over in bed”, “moving from lying on the back to sitting on the side of the bed”, “remaining sitting”, “standing up from the bed”, and “remaining standing”. Each item is scored from 1 of 6 based on how much help is needed from another person or a special environment in completing the task. Individual scores of the five items are summed, with a maximum possible score of 30 (independent) and a minimum of five (totally dependent). The ABMS II form is shown in Appendix 1.
The Barthel Index (BI) is a standardized measure with 10 items that assess the patient’s level of independence and dependence in their ADL [14,15]. The 10 items comprising the BI focus on self-care (bathing, grooming, bladder management, bowel management, dressing, feeding, and toilet use) and mobility (transfers, ascending and descending stairs, and walking). The items are scored on a scale of 0 to 10, and individual scores of the ten items are summed to a maximum possible score of 100 (independent) and a minimum of 0 (totally dependent).
Both the ABMS II and BI were assessed by a physical therapist on the first day of postoperative rehabilitation and at discharge from the hospital.
The patients’ baseline characteristics were analyzed using a 2-sample t-test and χ2 analysis. Linear mixed model (LMM) in split-plot analysis of variance (ANOVA) was used to determine the effect of group (CPP or control) and stage of rehabilitation (beginning or end) on ABMS II and BI. The Split-plot model of the LMM included both patient identity and group as subject variables, and rehabilitation stage as a repeated variable. The LMM analyses were performed with ABMS II and BI as dependent variables, with both group and stage as fixed factors. If any baseline characteristics were significantly different between groups, the item was adopted as a covariable in LMM analyses in order to test parallel regression between independent variables and covariates. Bonferroni’s multiple comparison was used as a post-hoc test. When ANOVA showed significant interactions, further investigations were performed among groups and stages. When ANOVA showed significant main effects, further investigations were performed using estimated means between groups or stages. Significance was set at P < 0.05. Statistical analyses were performed with SPSS Ver. 24 software (IBM, Chicago, IL, USA).
Between-group comparisons of baseline characteristics are shown in Table 1. A significant difference between groups was found only in gender (p = 0.008). However, the interactions (group*gender, stage*gender, and group*stage*gender) were not significant for any of the outcomes (p = 0.153, p = 0.710, and p = 0.319, respectively). In particular, duration of rehabilitation was not significantly different between the two groups (p = 0.35).
The outcomes of ABMS II and BI measured on the first day of postoperative rehabilitation and at discharge are shown in Table 2. On LMM in the split-plot design, main effects of group and rehabilitation stage on ABMS II were significant (p = 0.005, p < 0.001, respectively), although the interaction between them on ABMS II was not significant (p = 0.364). The main effect of rehabilitation stage on BI was significant (p < 0.001), although the main effect of group and the interaction between them on BI were not significant (p = 0.638, p = 0.144, respectively). The estimated mean of ABMS II on the first day and discharge stages in the CPP group was significantly higher than in the control group (p = 0.005). The estimated means of ABMS II and BI in both the CPP and control groups at the time of discharge were significantly higher than those on the first day of postoperative rehabilitation (p < 0.001).
This is the first study to demonstrate the influence of precaution-free management following use of the CPP approach to BHA on rehabilitation outcomes. Patient groups in this case-control study were well matched and the baseline characteristics of gender unmatched patients were considered as covariates in the statistical analysis. We believe that the difference in ABMS II scores between groups was associated with whether or not precautionary management for dislocation after BHA was performed. Our findings suggest that precaution-free management accompanied by the CPP approach is a positive predictor of basic mobility function in the early post-BHA period.
The estimated means of ABMS II scores on both the first rehabilitation day and at discharge were significantly higher in the CPP group than in the control group. It appears that on the first day, the mean of ABMS II in the precaution-free rehabilitation group was higher than in the control group, and that this difference was sustained from the first rehabilitation day up to discharge. The between-group difference in ABMS II on the first day of rehabilitation could have also resulted from the difference in precautionary management provided by nurses before rehabilitation. Our result supports previous studies which reported hip precautionary management was associated with a slower recovery of mobility function after THA [12,16-18]. This suggests that the decision regarding whether or not to conduct precautionary management for dislocation is a significant factor determining mobility after BHA.
There were no statistically significant effects of group on BI in the early post-surgery period. One can suppose that the time period at which BI was measured after rehabilitation might have been too soon after surgery. Peak et al. [18] reported that recovery of most of the functional parameters, such as ADL, was noted beyond 3 weeks postoperatively in the non-precaution group. In addition, BI score in the control group was apparently higher than in the CPP group. The recovery process of ADL is often associated with multimorbidity [19], cognitive impairment [20], and in-hospital delirium[20]. Cognitive impairment, in particular, might be a potential confounding factor that is associated with both BI score and surgical indications for BHA. The CPP approach might lead to inclusion of patients with cognitive impairment in the surgical indications for BHA, due to the reduced dislocation risk after the procedure. Future studies should include follow-up for a longer period after surgery and details about cognitive impairment in the baseline characteristics.
Regarding duration of rehabilitation, there was no statistically significant difference between the two groups. In Japan, regional clinical pathways for hip fracture patients are commonly practiced with the aim of standardizing and optimizing medical care by cooperation among multiple medical institutions. Reportedly, regional clinical pathways for hip fracture patients are effective in reducing the postoperative length of hospital stay [21]. The regional clinical pathways were followed for all patients in this study, and the length of hospital stay and duration of rehabilitation were controlled. Therefore, our precaution-free management likely did not reduce the duration of rehabilitation, since this is typically determined by the regional clinical pathway.
The present study had some limitations. First, this retrospective case-control study might have included patients with potentially confounding factors, such as cognitive impairment. Second, it has been reported that there are various surgical techniques for preserving the hip rotator tendon in BHA. Additionally, BHA is commonly performed not only using the posterior approach but also using the anterior approach. Hence, the applicability of these findings to BHA performed through preservation techniques other than CPP remains questionable. Third, the precautionary management for dislocation in the control group conducted at our hospital might have been strict, i.e. patients in the control group were prescribed use of an abduction pillow when they were sleeping on their side and rolling over. Hence, the influence of precaution-free management for dislocation at other institutions where such stringent precautions are not taken might differ from our results. Finally, so far, only a small number of surgeons are proficient at performing CPP. However, it is believed that the CPP approach would be easy for surgeons with some experience in the posterior approach to BHA, because the CPP approach needs no specialized equipment. Future studies should include a larger number of patients and multi-institutional data.
Our study shows that basic motor function in the early rehabilitation period is better in patients under precaution-free management for dislocation after BHA with the CPP approach than in patients under precautionary management after conventional BHA. The results suggest that precaution-free management for dislocation accompanied by the CPP approach might enhance the recovery process and improve early rehabilitation after BHA.
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This work was supported by JSPS KAKENHI Grant Number 20K19381.

![]()

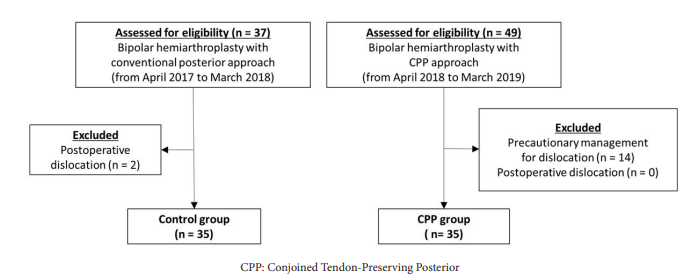 |
| Figure 1: Patient enrollment flowchart |
|
CPP group (n = 35) |
Control group (n = 35) |
p-value |
Age (year) (mean ± SD) |
78.1 ± 10.3 |
82.1 ± 9.0 |
0.09 |
Gender (%) |
|
|
|
Male |
42.9 |
14.3 |
0.01 |
Female |
57.1 |
85.7 |
|
Body mass index (kg/m2) (mean ± SD) |
21.5 ± 4.0 |
21.3 ± 3.5 |
0.77 |
Functional status prior to surgery (%) |
|
|
|
Independent |
77.1 |
85.7 |
0.50 |
Partially/totally dependent |
22.9 |
14.3 |
|
Dementia (%) |
11.4 |
17.1 |
0.38 |
Waiting period for rehabilitation (days) (mean ± SD) |
1.1 ± 0.3 |
1.1 ± 0.2 |
0.40 |
Duration of rehabilitation (days) (mean ± SD) |
14.6 ± 7.0 |
12.1 ± 4.5 |
0.35 |
|
CPP |
Control |
Estimated mean |
ABMS II |
|
|
|
First day |
16.0 (14.0-18.0) |
14.1 (12.8-15.5) |
14.9 (13.8-16.0) * |
Discharge |
25.1 (23.5-26.7) |
23.8 (21.7-25.9) |
23.0 (21.9-24.1) * |
Estimated mean at stages |
20.4 (19.0-21.7) * |
17.6 (16.2-18.9) * |
|
BI |
|
|
|
First day |
18.0 (13.2-22.8) |
13.9 (7.7-20.1) |
14.8 (10.1-19.6) * |
Discharge |
57.5 (48.5-66.5) |
65.4 (55.0-75.9) |
57.7 (52.9-62.5) * |
Estimated mean at stages |
37.2 (31.5-42.9) |
35.3 (29.5-41.1) |
|




































