Open Access
Research Article
Max Screen
ISSN: 2639-930X
Copyright: © 2021 Moussa K. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
The heel fat pad cushioning is the result of its structure, shape, thickness. Its morphological modifications due to changes in the amount or distribution of the loads normally sustained by the foot can be disturbed and can result in heel pain. The heel fat pad was found to have a crest on its anterior dorsal surface, flanges on both sides and posteriorly, and a thick portion that reached and covered the posterior surface of the calcaneus and the Achilles tendon insertion. Its anterior internal portion is thinner, and a lump of fat is consistently present in this region [1]. The heel fat pad has an about 1-inch thickness and is divided into sections by ligamentous “baffles” which help keep the fat pad from spreading out and thereby aid in keeping the cushion where it belongs.
Occasionally, they can get injured and these baffles become stretched and then the fat pad spreads out and lose its function which can make weight-bearing very uncomfortable.
Many doctors when confronted with pain in the heel region of the foot will fall back on the diagnosis of plantar fasciitis.
Patient history is the key to properly diagnosing heel fat pad syndrome and should include, time(s) of the day when the pain most frequently occurs, type(s) of the footwear used, type(s) of activity level at work and during leisure time, and any history of trauma to the calcaneus.
The patient may present with or complain of deep aching pain at the center of the calcaneus, pain at night, and resting pain aggravated by barefoot walking on hard surfaces or after a long period of ambulation or standing. Pressing with the thumb into the center of the heel should re-create the pain.
Both heel fat pad and plantar fascia can be the source of heel pain; however, patients with plantar fasciitis classically have a gradual onset of symptoms and feel their pain more on the inner side of the heel. Pain typically occurs with the first step in the morning and lessens with activity, although it may return with activity during the day or with certain activities such as walking upstairs. The anteromedial aspect of the plantar aponeurosis is the point of maximal tenderness in patients with painful heel syndrome. Ankle dorsiflexion may be limited secondary to pain, and pain may be elicited through passive dorsiflexion of the toes. MRI and ultrasound can identify pathologic thickening of the fascia and surrounding edema suggestive of the condition. Radionuclide scanning, as well as computed tomography scans, has also been used in this setting to identify unknown causes of persistent heel pain [4-6]. Ancillary tests have limited value and are generally not necessary in identifying patients with plantar fasciitis.
Measurement of the heel fat pad index (skin calcaneus height weight-bearing /non-weight-bearing) from the lateral foot x-ray demonstrated (Figure 1) that the fat pad height compressed 25 and 47 % in normal subjects and patients with subcalcaneal pain and soft flattened heel pads respectively [7]. The plantar fascia is best evaluated with sagittal and coronal MR imaging. On coronal images, the inferior edge of the fascia is straight and contrasts sharply with adjacent fat. On sagittal images, the normal fascia has a uniform thickness from its calcaneal origin through its proximal half, whereas more distally it progressively thins until it reaches its metatarsal insertions. Standard imaging protocols are (a) sagittal T1-weighted and STIR images and coronal proton-density and T2-weighted images [8].
MR imaging characteristics of plantar fasciitis include (a) fascial thickening that is often fusiform and typically involves the proximal portion and extends to the calcaneal insertion and (b) increased signal intensity of the proximal plantar fascia (Figure 2). Other MR imaging findings that indicate plantar fasciitis includes edema of the adjacent fat pad and underlying soft tissues [9].
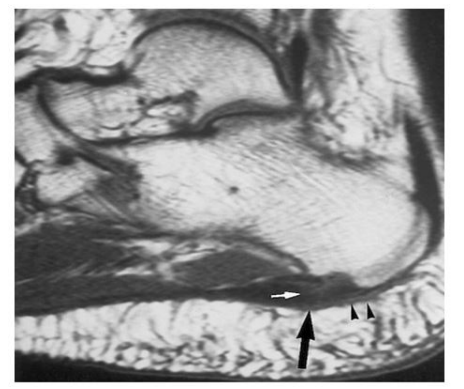
Heel pain may arise from the fat pad itself. For example, rupture of the fibrous tissue septa, which occurs mainly in obese elderly patients under the influence of ordinary weight-bearing or owing to loss of fat pad results in attrition of the fat pad with poor stress absorption [10]. A painful heel fat pad is often confused with plantar fasciitis. MR imaging can also help distinguish between these two conditions and in some cases of painful heel fat pad can demonstrate changes in signal intensity, with low-signal-intensity bands representing fibrosis and decreased height of the fat pad (Figure 3).
Other conditions to consider and rule out in the heel pain are tarsal tunnel syndrome, stress fracture, tumor, infection, and inflammatory arthritic conditions.
The management of the heel fat pad syndrome aimed at unloading the heel by avoiding aggravating activities. In an acute situation, the R.I.C.E. rule (Rest, Ice, compression, Elevation) should be applied and anti-inflammatory drugs are given [11].
Further treatment includes taping, heel cups or heel pad and the use of appropriate foot wear. Some other treatment may to consider would be laser, shockwave, and ultrasound.

![]()

 |
| Figure 1: The heel fat pad index |
 |
| Figure 2: MR images show marked thickening of the proximal plantar fascia (large arrows) with increased intrasubstance signal intensity (small arrows) |
 |
| Figure 3: Saggital MRI shows thinned out heel fat pad. Note that there is no signal in the plantar fascia or plantar muscles. Heel pad fat is relatively less in thickness and heel pad fat measures 1.3cm |




































