Open Access
Research Article
Max Screen
ISSN: 2639-930X
Copyright: © 2019 Padilla Colón CJ. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Sarcopenia is a syndrome which is characterized by the gradual loss of skeletal muscle mass and strength. The progression of sarcopenia can result in adverse outcomes such as physical disability, poor life quality and severe injuries that lead to death.
Objective: The purpose of this research study was to determine if a routine of strength training can be an effective prevention method for sarcopenia and if creatine consumption can be an efficient way to treat sarcopenia.
Methods: This is a descriptive type study, with a quasi-experimental design. The total population recruited for this study was 80 subjects, (n=80) between the ages of 65 to 79 years. The subjects were divided into three groups. The first group performed strength training only (n=34). The second group performed strength training and consumed creatine (5g) (n=20). The third group only consumed creatine (5g) and did not perform strength training (n=26).
Results: The combination of creatine with strength training reduced severe sarcopenia in women (-1.0% kg / m2, p < 0.05) and in men (-3.0% kg/m2, p < 0.001). Moderate sarcopenia in both sexes was also reduced (-2.0% kg / m2, p < 0.001). According to the results of this study, it was possible to determine that previous studies which suggest strength training as a treatment against sarcopenia, is very effective. However, the combination of strength training and the consumption of creatine can increase the prevention and treatment of sarcopenia.
Keywords: Strength Training; Creatine; Sarcopenia; Muscle Mass; Elderly
List of abbreviations: 1RM: 1-Rep Max; G: Grams; N: Subjects; TBW: Total Body Water; FFM: Fat Free Mass; FM: Fat Mass; NHANES: National Health and Nutrition Examination Survey; SMMI: Skeletal Muscle Mass Index; KG: Kilogram; M2 : Square Meter; SPSS: Statistical Package For The Social Sciences; +: More; -: Less; MM: Muscle Mass; NC: No Change; BMI: Body Mass Index
Sarcopenia, a musculoskeletal condition that results in the loss of muscle mass and function, is most prevalent in people who are 65 years and older. Aging is the product of many types of anatomical and physiological changes which lead to a substantial reduction in the function of the human body. The skeletal and muscular systems are largely affected by the process of aging and the deterioration of these systems can cause relative discapacity [1] in people. As time passes the elderly population becomes more affected by the loss of muscle mass and strength [2]. According to Cruz et al. [3], sarcopenia is a syndrome characterized by progressive and general loss of skeletal muscle mass and strength, which increases the risk of physical disabilities and mortality. Prevalences as high as 33% have been found in different elderly populations [4-6]. In addition, sarcopenia is associated with other health conditions such as: osteoporosis, type II diabetes and obesity [7-9]. The current data of sarcopenia has led to an interest in many research groups to determine the influence of sarcopenia in the lifestyle of older people, primarily on factors such as physical activity and nutrition [10,11]. Further study on sarcopenia is necessary because there is a need to develop effective interventions to prevent and treat this condition [12]. Physical inactivity is associated to the loss of muscle mass and strength, which suggests that an increase in the levels of physical activity can have positive effects [13]. Although, different methods of physical activity have been used, strength training has shown to have the greatest positive effects in general. Strength training is an effective method to treat and prevent sarcopenia by stimulating hypertrophy and increasing muscle strength [14]. In addition, strength training produces physiological adaptations that improve musculoskeletal health in aging, such as increased muscle mass, bone mass and strength [15]. In fact, it has been found that even individuals older than 90 years can increase their muscle conditioning through strength training [16]. Aside from strength training, ergogenic nutritional aids offer direct physiological benefits for exercise performance and recovery. There is evidence to support the beneficial effects of specific nutritional interventions in the elderly, such as creatine supplementation [17]. The combination of strength training and creatine supplementation could be an effective intervention to improve musculoskeletal health in aging [15]. This can be translated into the functioning of daily activities and improved quality of life [18]. Aging is associated with lower levels of creatine and phosphocreatine, specifically in skeletal muscle. The rates of phosphocreatine regeneration after exercise decrease by approximately 8% every decade after 30 years [19]. On the other hand, a recent review describes that the administration of the creatine supplement with strength training plays an important role in muscle health in the aging population. It has been found that its positive effect is not only found in the muscular area, but also increases bone mineral density and the index of bone biology [15]. Based on other publications, creatine had a beneficial effect on muscle mass in elderly individuals [15]. For this reason, the objective of the present study is to determine if strength training and creatine intake prevent sarcopenia in older people.
This is a descriptive study, with a quasi-experimental design (pre-test and post-test measurements). The total population included in this study was 80 subjects between the ages of 65 and 79 years. The recruitment process consisted in verbally approaching the subjects of a geriatric center in Puerto Rico to participate voluntarily in the study (41 females and 39 males). Each subject signed an informed consent accepting to participate in the study. This process was carried out after acquiring the necessary permits from the center’s ethics committee to begin the investigation. None of the subjects had participated in physical training programs or engaged in vigorous physical activity more than 3 times a week for 30 minutes a day, when recruited for study. No participant required the use of mobility assistance devices. Each subject underwent a thorough review, which included a personal interview at the geriatric center by a registered nurse and a medical evaluation. The exclusion criteria included: evidence of coronary disease; congestive heart disease; uncontrolled hypertension; chronic obstructive pulmonary disease; mellitus diabetes; renal insufficiency; greater orthopedic disability and smoker. Each subject was assigned randomly to one of three groups: the first group performed strength training (n = 34), the second group performed strength training and ingested creatine (5g / day) (n = 20). Finally, the third group did not perform strength training, but ingested creatine (5g / day) (n = 26). Both group # 2 and group # 3 ingested creatine monohydrate (5g / day). Group # 2 ingested the creatine 60 minutes before training and group # 3 at ingested the creatine at the same time as group # 2 (10:00 am). Group 1 and 2 performed strength training 3 days per week on non-consecutive days (Monday, Wednesday and Friday).
The measuring instruments used in this study were: 1) Bioelectrical impedance (OMRON Full Body Sensor Body Composition Monitor and Scale, Model HBF-514) to estimate the absolute muscle mass. This instrument allows the estimation of total body water (TBW) and, by assumptions based on the hydration constants of the tissues, the fat-free mass (FFM) is obtained and by derivation, the fat mass (FM), by means of a simple equation based on two components (FFM kg = total weight kg - FM kg). 2) To evaluate muscle strength the cybex system (free weights, 1RM and strength training) was used.
Since the population was composed of subjects with advanced age, the 1RM was used based on the modality of predicting a maximum repetition (Formula: 1RM = weight lifted / (1.0278 - (0.0278 x Nº of repetitions) [20]. Training after the test of maximum strength was applied according to the results of the 1RM test. Before beginning the 8 weeks of study, the subjects had to undergo an anatomical phase. The objective of this phase consisted in the progressive adaptation of muscles and especially of the insertions muscle in the bones, in order to easily withstand the increasingly heavy loads during the following days or phases of training, in addition, to work with the technique of strength exercises. The method used on the phase of anatomical adaptation and the entire 8 weeks of study was circuit training (free weights). The weight loads during the phase of anatomical adaptation remained very light (from 40 to 60 % of 1RM) and the exercises were performed with a high number of repetitions (10 to 15 repetitions), with a rest time of 2 to 3 minutes between the exercises. A series of each exercise (9 exercises) was performed during the first 2 weeks of physical conditioning (anatomical adaptation). In the next 2 weeks, 2 series of each exercise were performed. In the 8 weeks of the study, 2 and 3 series of each exercise were used. The first 2 weeks were performed at 40% of the results of 1RM, the third and fourth week of 50 to 60%, the fifth and sixth week of 65-75% and the seventh and eighth week at 75-85%. The exercise routine used in this study was: bench press with dumbbells, standing with dumbbell, dumbbell squats, bending knees in sitting position, dumbbell shoulder abduction, bending dumbbell elbows in standing position, extension of elbows with dumbbells in a sitting position, alternating extension of hips and short abdominal on the floor with slightly flexed knees. All these exercises were used in the anatomical phase and in the 8 weeks of study.
Based on the statistical analysis of the data from the NHANES III study in elderly men and women (> 60 years), we proceeded to identify the index or type of sarcopenia in the study sample. The skeletal muscle mass index (SMMI) was used using the absolute muscle mass and not the muscle mass of the extremities (absolute muscle mass / height2). In males: severe sarcopenia (< 8.50 kg /m2), moderate sarcopenia (8.51 - 10.75 kg / m2) and normal muscle (> 10.76 kg / m2) was observed. In women: severe sarcopenia (< 5.75 kg / m2), moderate sarcopenia (5.76 - 6.75 kg / m2) and normal muscle (> 6.76 kg / m2) was observed. All these results were measured using the criterion of muscle mass and bioelectrical impedance.
The results were collected in a template designed in Windows Excel 2010. The data that was obtained was summarized using descriptive statistics (frequency, mean ± standard deviation). The Kruskal-Wallis post-host test after Dunn was used for multiple pairwise comparisons of the study groups. P-values were adjusted using the Bonferroni correction method. Statistical analysis of the data was performed using “The R Project for Statistical Computing”.
Table 1 shows the physical and anthropometric characteristics of the participant three groups, shown in terms of mean and standard deviation.
All of the results were greater for men in strength increase, except for the group that took creatine without strength training. In this group there was a reduction in both sexes, and men demonstrated the greatest decrease (-2.9, p = 0.001) (Table 1). The correlation analysis demonstrated that the group which used the creatine along with strength training, obtained the highest percentage of increase in muscle strength after the training sessions (1RM, bench press) (r = .95, r2 = 1.00, p = 0.01). Strength exercise increased the amount of muscle mass more in men than in women (p = 0.001). The correlation analysis showed that the group which used creatine treatment in combination with strength training obtained the highest percentage of increase in muscle mass after the training sessions (r = .92, r2 = 1.00, p = 0.01).
As for maximum strength test (1RM), multiple comparisons were made between the study groups. In men, a significant difference was found in the comparison of those who did strength training (Group = 1) and those who did strength training with creatine consumption (Group = 2) (p = 0.0049) and also those who did strength training with consumption of creatine (Group = 2) and those who only took creatine (Group = 3) (p = 0.00096). When comparing the group that did strength training (Group = 1) with those who took creatine (Group = 3), no significant difference was found. In women, when comparing the group of those who did strength training (Group = 1) and those who only took creatine (Group = 3), a significant difference was found (p = 0.0062). The same was observed when comparing the group of strength training with consumption of creatine (Group = 2) with those that only took creatine (Group = 3) (p = 0.00028). No significant difference was observed between the strength training group (Group = 1) and the strength training group with creatine consumption (Group = 2) (p = 0.23).
In terms of muscle mass (MM), multiple comparisons were also made between the study groups. In men, a significant difference was found in the comparison of those who did strength training (Group = 1) and those who only took creatine (Group = 3) (p = 0.00023) and also in the comparison of those who did strength training with consumption of creatine (Group = 2) and those who only took creatine (Group = 3) (p = 0.0095). There was no significant difference between those who did strength training only (Group = 1) and those who did strength training with creatine consumption (Group = 2) (p = 0.88). In women, none of the comparisons resulted in a significant difference (p = 0.05).
According to the results presented in Figure 1, the group that performed strength training, under the degree of severe sarcopenia (Men- 8.0% to 7.0% kg / m2); (Women-16.0% to 15.0% kg / m2), showed a decrease in both sexes (-1.0% kg / m2) with a p = 0.001 and an effect by sex and training of 0.001. In the level of moderate sarcopenia, the results demonstrate that there were no changes in women (Pre- 24.0% kg / m2 and Post 24.0 kg / m2, p = 0.001) with a sex effect of 0.001, while men who were classified with moderate sarcopenia had a reduction of (-2.0% kg / m2, p = 0.002) and an effect by sex of 0.0001. The results for the normal muscle show an increase in the females of the study (+ 2.0% kg / m2, p = 0.001), while in men the increase in normal muscle was greater (+ 4.0% kg / m2, p = 0.0001).
The results presented in Figure 2 demonstrate the muscle mass increase when treated with creatine and strength training. The women who had severe sarcopenia demonstrated a reduction of muscle mass (-1.0% kg / m2, p = 0.050) while in men the decrease in muscle mass was greater (-3.0% kg / m2, p = 0.001) with an effect by sex of 0.001. In the group of moderate sarcopenia both sexes demonstrated a decrease of muscle mass (-2.0% kg / m2, p = 0.001) and an effect by sex and training of 0.001. In the classification of normal muscle mass, an increase was seen in both sexes (+ 4.0% kg / m2, p = 0.001) in women, while in men the increase was greater (+ 6.0% kg / m2, p = 0.001). According to these results we can see a relationship in the effect by sex of p = 0.001.
Figure 3 shows the results of the group that ingested creatine and did not perform strength training. In the condition of severe sarcopenia in men and women, both did not show changes (p = 0.001). In the condition of moderate sarcopenia, the results in men remained constant (20.0% kg / m2 , p = 0.001), while in females an increase was observed (+ 2.0% kg / m2 , p = 0.001). Finally, in the normal muscle there were no changes in men (17.0% kg / m2 , p = 0.001), and in women there was a decrease in normal muscle (-2.0% kg / m2 , p = 0.05). Both with an effect per sex of p = 0.002.
The correlation analysis demonstrated that the group who used creatine treatment along with strength training had a better effect in percentage change of the degree of sarcopenia (From severe sarcopenia to moderate sarcopenia to normal muscle after training and creatine treatment (r = .82, r2 = 1.00, p = 0.01).
Strength training is currently one of the most effective methods to combat sarcopenia by stimulating hypertrophy and increasing strength. Through this study it was possible to demonstrate that the investigations regarding strength training as a treatment against sarcopenia are still effective. As for example, these authors indicate that strength training has shown efficacy in the treatment and prevention of sarcopenia, increasing muscle mass and strength and better neuromuscular adaptation [21-25].
Typically, the strength increases associated with strength training have been much greater than the hypertrophic response. This data could be checked in our study to see how the increase in muscle strength was greater than gains in muscle mass. This can be supported by the research of Strasser et al. (2009) [26], where they showed that after 6 months of strength training 3 times a week the strength was increased by 15% more than the muscle mass for the leg press (p = 0.01), 25% for the bench press (p = 0.01) and 30% for chest halon (p = 0.001).
Like muscle strength, hypertrophy is significant when it comes to preventing sarcopenia. According to Binder et al. (2005) [27] three months of supervised strength training resulted in an increase of voluntary maximum strength and fat-free mass in thigh muscle and the entire body in older women and men. This study by Binder et al. (2005) [27] and others such as Liu and Latham (2009) [25] confirm what was presented in our study where increases in strength and muscle mass are appreciated using 2 to 3 training sessions per week after 6 weeks of study. Through our study we can reaffirm what was established by Burton and Sumukadas (2010) [28], that performing strength exercises in the elderly improves muscle mass and muscle strength.
Some results found in the literature on the effect of strength training in elderly people is clear [14,25]. When analyzing the studies of Rolland et al. (2011) [14] and Liu and Latham (2009) [25] when using strength training methods we can point out that there is similarity with the results in our study since strength training in the elderly caused a reduction in the loss of sarcopenia.
In this study, no cases of side effects were reported due to the treatment of strength training. This agrees with that established by Malafarina et al. (2012) [29], where I also use strength training without finding side effects in a normal older population.
Previous randomized controlled studies agree with what was established in our study on the importance of increasing the amount of work in training as time passes. In this study conducted by Steib et al. (2010) [30] showed a remarkable dependence on strength capacity to improve strength training intensity. In another follow-up study Ciolac et al. (2010) [31] subjected men (between the ages of 65 and 72) to 13 weeks of strength training. Finding increases in strength as a progressive adaptation to training. Strength training can cause muscle hypertrophy by working 3 times a week for 8 to 12 weeks under the circuit modality with an intensity of 70-90% of (1RM) emphasizing eccentric movements [23]. If the training period is longer, the effect increases steadily [32]. What this author agrees with, what was done in our study, since muscle mass was found using also 3 days of strength training per week within the 8-week study period.
Rawson and Venezia (2011) [33] found in their study that in older adults, creatine supplementation and strength training increase lean body mass, improve fatigue resistance, increase muscle strength and improve performance in the activities of daily life, more than strength training alone. Something similar was found in our study, since the greatest changes were obtained in subjects who combined the intake of creatine with strength training. Another study which supports our results was done by Gothshalk et al. (2002) [34], who verified the effects of creatine supplementation in physically active elderly people. The results indicated that creatine supplementation caused increases in muscle mass, maximum dynamic force and maximum isometric strength. The study establishes that these results contribute to the reduction of sarcopenia in elderly people.
Some studies, like ours, indicate that the greatest changes were observed in subjects who were treated with a creatine intervention. Brose et al. (2003) [35] showed that subjects who took creatine had a higher fat-free mass and greater strength. In another study, people who took creatine had a 3.3 kg increase in lean muscle mass compared to a 1.3 kg gain (kg) in the placebo group [36]. In another investigation, Brose et al. (2003) [36] were able to confirm that creatine supplementation helps stimulate exercise by improving total fat-free mass gain and gains in various isometric muscle strength indices. Candow et al. (2008) [37], established that the consumption of creatine in low doses helps to increase lean tissue mass and strength in bench press exercises. In our study we also found in the post test results an increase in muscle strength in the group that used creatine in combination to strength training. In another study, Dalbo et al. (2009) [38] suggested that the combination of creatine intake with strength training provides better results than training alone. Also, Bemben et al. (2010) [39] pointed out that creatine significantly increases muscle strength and increases muscle mass.
For many years it was not clear if the use of creatine supplementation without strength training can have an increase in strength and muscle mass in the elderly. According to the results of our study the use of creatine without strength training as well as a research published by Gotshalk et al. (2008) [40] showed minimal increases in the levels of muscle mass in a group of men (MM Pre- 31.4 ± 2.2, post 31.9 ± 2.0) and women (MM Pre- 29.5 ± 1.0, post 29.9 ± 1.2) of the study (p = 0.007). The increase was greater in men. Regarding the effect of creatine without strength training, a slight reduction in strength was observed in the results of both the men and women group of the bench press test. Bermon et al. (1998) [41], found no improvement in muscle strength results in those who used creatine without strength training. Rawson and Clarkson (2000) [42] also did not find improvements in muscle strength in the elderly population. In our study, the results demonstrated that the intake of creatine without strength training is not effective in preventing or reversing the sarcopenia.
Strength training could improve the adverse effects caused by the loss of strength and muscle mass, also known as sarcopenia. The combination of strength training with the intake of creatine can increase the benefits in preventing the sarcopenia. The intake of creatine without strength training does not produce significant increases in muscle strength or significant increases in muscle mass in the elderly population. The intake of creatine without strength training does not cause changes in the prevention and reduction of sarcopenia. Future research should examine the effect of the amount of creatine intake and its effect on the increasing age in the population aged 65 and older. Strength training is considered an effective method for the muscle mass loss so the elderly population with sarcopenia should have the alternative to perform this type of training. Also, health professionals can help this population by recommending the strength exercise.

![]()

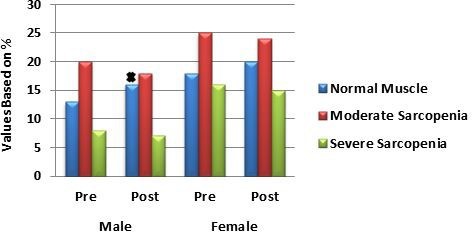 |
| Figure 1: Changes in the degree of sarcopenia through strength training. Values of 34 elderly subjects based on %, p < 0.05 and the effect by sex. Indicates higher increase. (N = subjects, % = percent) |
 |
| Figure 2: Changes in the degree of sarcopenia through the administration of creatine and strength training. The values of 20 subjects of advanced age, p < 0.05 and the effect by sex are presented in the figure and indicate a higher increase of muscle mass. (N = subjects, % = percent) |
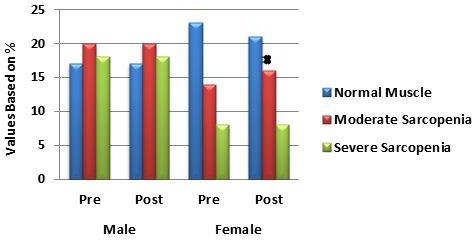 |
| Figure 3: Changes in the degree of sarcopenia through the use of creatine without strength training. Values of 26 elderly subjects, p < 0.05 and the effect by sex. Indicates increase. (N = subjects, % = percent) |
|
Strength Training |
Strength Training and Creatine Intake |
Creatine Intake Only |
|||||||||
|
Men (N=21) |
Women (N=13) |
Men (N=8) |
Women (N=12) |
Men (N=10) |
Women (N=16) |
||||||
|
Pre |
Post |
Pre |
Post |
Pre |
Post |
Pre |
Post |
Pre |
Post |
Pre |
Post |
Age |
71.7±1.1 |
NC |
71.9±1.4 |
NC |
68.9±1.9 |
NC |
68.4±1.3 |
NC |
67.8±0.8 |
NC |
73.6±1.2 |
NC |
Height (cm) |
163.6±3.7 |
NC |
149.4±9.1 |
NC |
173.1±3.2 |
NC |
165.6±1.8 |
NC |
158.0±1.4 |
NC |
147.5±7.8 |
NC |
Weight (kg) |
73.0±3.0 |
72.3±2.9 |
62.6±2.4 |
62.9±2.3 |
64.0±6.1 |
64.4±5.8 |
66.2±3.3 |
66.7±3.3 |
69.1±2.8 |
69.2±2.0 |
70.9±3.4 |
76.3±6.3 |
IMC |
27.6±0.8 |
27.8±0.7 |
27.7±1.3 |
28.8±1.4 |
27.9±0.9 |
28.0±0.8 |
27.3±1.3 |
28.5±1.5 |
27.8±1.1 |
28.5±0.9 |
30.4±1.4 |
34.1±1.3 |
%Fat |
31.6±1.5 |
28.8±1.5 |
31.6±2.1 |
30.7±1.9 |
29.3±1.4 |
26.3±1.4 |
28.8±1.6 |
28.9±1.6 |
33.9±1.2 |
35.1±1.1 |
42.0±3.2 |
43.4±3.1 |
IRM |
50.3±3.9 |
54.2±4.2 |
31.2±3.4 |
33.9±2.8 |
56.9±4.8 |
62.8±5.5 |
42.6±3.9 |
46.8±4.3 |
33.8±4.7 |
30.9±4.8 |
28.7±2.1 |
26.9±2.0 |
MM |
26.8±1.2 |
27.6±1.1 |
25.2±0.9 |
25.7±0.8 |
24.8±1.7 |
27.4±4.8 |
20.9±1.2 |
22.4±3.6 |
31.4±2.2 |
31.9±2.0 |
29.5±1.0 |
29.9±1.2 |




































