Open Access
Research Article
Max Screen
ISSN: 2639-930X
Copyright: © 2019 Mustofa KSM. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Purpose:Study purpose was to explore the efficacy of Neural Mobilization with conventional physiotherapy compare to only conventional physiotherapy for the treatment of radiating Low Back Pain (LBP).
Objectives:To determine the socio-demography of LBP and to analyze the efficacy of Neural mobilization in reducing pain and improving function by reducing disability.
Methodology:This study is an experimental design (RCT). Fourteen patients with radiating LBP simple random sampling selected than 7 patients were randomly assigned to Neural Mobilization with conventional physiotherapy group and 7 patients to the only conventional physiotherapy group. Numeric Pain Rating Scale (NPRS) was used to measure pain and Oswestry Disability Index (ODI) was used to measure disability. Statistical analysis was done by using Mann-Whitney U test
Results:Mean difference of pain between pre-test and post-test of experimental group and control group were 4.28 and 2.27 and mean difference of ODI score between pre-test and post-test of experimental group and control group were 30.51 and 9.81. Following application of treatment the study found that the experimental group showed a significant improvement (p <.05) in case of LBP
Conclusion:Study concludes that Neural Mobilization with conventional physiotherapy is more effective than conventional physiotherapy alone for patients with radiating LBP
Keywords: Neural Mobilization; Conventional Physiotherapy; Radiating Low Back Pain
Low Back Pain (LBP) is a widespread and costly problem in many countries; it is a common musculoskeletal disorder causing pain that could be acute, sub-acute and chronic. It affects 80% of people at some point in their lives [1].
Bangladesh is one of the highly populated developing countries in the world [2]. According to World Health Organization statistics, 10% of population in Bangladesh is disabled [3]. Low back pain is one of the most common causes of disability and the burden for the individual, society and as well as the National Health Service in the world [4]. Low back pain is the most common condition in the developed Western countries [5]. Approximately 80% of all human beings experience LBP in their lives [6]. It is the number one most common cause of activity limitation, the second most frequent cause of doctor’s visit and the third most common cause of surgical procedure in USA [7].
Low back pain may be radiated to the lower limb. The prevalence of leg pain, as a referred symptom associated with back pain has been shown to be approximately 35%, while true prevalence of sciatica is 2-5% [8].
According to Hoy et al., Low Back Pain is the global cause of personal, community and financial burden as it is one of the most common health problems [9]. LBP is of significant socioeconomic relevance because it may lead to a temporary loss of productivity, enormous medical and indirect costs, or even permanent disability [7].
LBP is one of the commonest causes of disability in the working population. Employees who are unable to work due to back pain spend a significant amount of time on sick leave, which impacts on productivity in the work place [10].
The incidence of LBP peaks in middle age and the most common age range is between 35 to 55 years, but it declines in older age. Men and women are equally affected but after 60 year often women report more low-back syndromes than men [11].
Pain in the low back area is a common phenomenon. Mechanical problems are the most common cause (around 90%) and a majority (70% to 85%) does not have a specific cause identified. Any injury to one of the intervertebral discs (disc tear, disc herniation), ligament and joint also causes pain [12]. The cause of LBP depends on different factors. Hills mention that the mechanical low back pain is the most common cause of work related occupational disability [6]. Low back pain also aggravated by poor sitting posture in both sedentary and manual workers [4]. Traumatic or degenerative conditions of the spine are the most common cause of low back pain although disk protrusion and herniation have been popularized as cause of LBP [11].
Neural mobilization is a gentle movement technique used by the physiotherapists to move the nerves. Neural mobilization of the nervous system, was described by Maitland in 1985, Elvey in 1986 and refined by Butler in 1991, is an addition to assessment and treatment of neural pain syndromes including lumber spinal syndromes [13].
Nee & Butler (2006) proved that the neurodynamic technique can be effective in addressing musculoskeletal presentation of neuropathic pain [14]. The study included that the peripheral neuropathic pain is because of injury to root or peripheral nerve trunk by mechanical or chemical stimuli. Clinical manifestation includes positive and negative symptoms. Positive symptoms reflect an abnormal level of exhibitions in the nervous system and include pain, paraesthesia, and dyesthesia. Negative symptoms indicate reduced impulse conduction in the neural tissue and hypoesthesia or anaesthesia and weakness.
Neural mobilization is a part of manual therapy that has been reported to be an effective intervention for certain condition including low back pain, sciatica and piriformis syndrome [15].
Neural mobilization technique often used clinically to restore nerve mobility and decrease pain [16]. Shacklock stated that the neuraxis, meninges and spinal canal forms a mechanical triad. The nervous system as a whole is a mechanically and physiologically continuous structure from the brain to the distal end of the peripheral nerves therefore, movement at one end affects the whole system and concluded that movement at the ankle joint helped in mobilizing the sciatic nerve proximally at lumbosacral level [17].
Butler stated that the neural system is a dynamic organ spanning the entire body. The mobility of this system is such that it can act dependently or independently of the structures it spans .When changes imparted in one area of the neural system it may affect the whole system [18].
Butler stated that clinicians use neural mobilization for the treatment of nerve root and peripheral nerve related symptoms in the low back and the lower extremity pain [13].
Neural mobilization has a great role in management of low back pain with radiculopathy and has long term effects for patient with non-specific low back pain.
Traditional exercise therapy program for lumber pain focuses on pain relief but neural mobilization viewed as another form of manual therapy that restore the mechanical function of impaired neural tissue [15].
Sahar found that neural mobilization in treatment of low back dysfunctions is effective in improving pain, reducing short term disability and promoting centralization of symptoms rather than lumbar mobilization treatment with exercise therapy [19].
Patients treated with neural mobilization and lumbar stabilization showed better VAS scores and Straight Leg Test scores compared to patients treated with active range of motion exercises and lumbar stabilization [20].
Butler stated that distal mobilization of the sciatic nerve affects the nerve roots at lower lumbo-sacral level [18].
Xavier and Farrel studied the effects of neural mobilization of sciatic nerve in 21 subjects, and concluded that treatment of the distal portion of nerve by neural mobilization relieved distal pain and score of Visual analog scale (VAS) was decreased to 70% [21].
The study of single-blind randomized controlled trial of thirty subjects (male 10, Female 20) by Allison et al., clearly demonstrated significant improvements in pain and disability in both experimental and control group. The Neural Mobilization group had significantly lower pain levels by compared to the articular mobilization treatment group [22].
Neural mobilization along with conventional treatment was found to be more effective for sciatica in relieving pain (t = 7.643) as well as improving the range of SLR (t = 5.848) than conventional treatment alone [23].
The study was designed using an experimental design quantitative research. According to DePoy & Gitlin the design could be shown by:
Experimental Group : R O1 X O2
Control Group : R O1 O2
The study was an experimental between two subject designs. Neural Mobilization and other Physiotherapy treatment were applied to the experimental group and only other Physiotherapy treatment was applied to the control group [24].
Experimental group:Participants involved in this group received conventional physiotherapy treatment along with neural mobilization to alleviate their pain.
Control group:Participants involved in this group received only conventional physiotherapy treatment to alleviate their pain. A pre-test (before intervention) and post-test (after intervention) was administered with each subject of both groups to compare the pain and functional ability of the subject before and after the treatment (Figure 1).
Musculo-skeletal Unit of Physiotherapy Department at CRP, Savar, Dhaka.
The study population was the patients diagnosed with radiating Low Back Pain attended in the Musculo-skeletal Unit of Physiotherapy Department at CRP, Savar, Dhaka.
The equation of the sample size calculation are given below
The actual sample size for this study was calculated as 246, but as the study was performed as a part of academic research project and there were some limitations. So that 14 samples was selected conveniently according to inclusion and exclusion criteria for this study. 7 participants were in experimental group and 7 participants in control group
Simple random sampling technique was used for this study:Subjects, who met the inclusion criteria, were taken as sample in this study. 14 patients with radiating Low Back Pain were selected from outpatient musculoskeletal unit of physiotherapy department of CRP, Savar and then 7 patients were randomly assigned to Experimental group comprising of treatment approaches of Neural Mobilization along with other Physiotherapy treatment and 7 patients to the only other Physiotherapy treatment for this study. The study was a single blinded technique. When the samples were collected, the researcher randomly assigned the participants into experimental and control group, because it improves internal validity of experimental research. The samples were given numerical number C1, C2, C3 etc. for the control group and E1, E2, E3 etc. for experimental group. Total 14 samples were included in this study, among them 7 patients were selected for the experimental group [received Neural Mobilization along with conventional physiotherapy treatment] and rest 7 patients will be selected for control group (receive only conventional Physiotherapy treatment)]
• Low Back Pain with radiation to lower limb caused by mechanical problem
• Age group:18-60 year [25]
• Male and female both were included
• Patients with clinical disorder (eg: acute disc prolapsed) where Neural Mobilization is contraindicated
• Diagnosis of secondary complications such as tumor, TB spine, fracture, dislocation and severe osteoporosis, Paget’s disease (secondary complicated cases could be more severe and may not respond to treatment)
• All sorts of infection (eg: Rheumatoid Arthritis, Ankylosing Spondylitis where active infection presence and treatment will not be effective)
• History of any malignant disease (which may spread out along with treatment)
• Cauda-equina lesions , Transverse myelitis (where bowel bladder incontinence presence)
• Surgery to the lumber spine (eg: disectomy, spinal fixation, laminectomy etc)
• Pregnant women
• Mentally retarded patient
• Patients those are taking pain killer to alleviate their low back pain
Data Collection Tools
• Record or Data collection form
• Consent Form
• Structured questionnaire. (Both open ended and close ended questionnaire)
• Numeric Pain Rating Scale - for measuring pain.
• Oswestry Disability Index (ODI)
Numeric Pain Rating Scale (NPRS):McCaffery, et al., used a numeric scale to rate the pain status experienced by patients. It is known as Numeric Pain Rating Scale. The scale is a 10cm long scale ranging from 0-10. Here a zero (0) means no pain, 1-3 indicates mild pain, 3-5 indicates that pain is in moderate state and 6-10 is worst possible pain feeling experienced by patients [26].
Oswestry Disability Index (ODI): This is a set of questionnaire that has been designed to provide information regarding how the patient’s back pain affects his/her ability to manage in everyday life
Data Collection Procedure:The study procedure was conducted through assessing the patient, initial recording, treatment and final recording. After screening the patient at department, the patients were assessed by a qualified physiotherapist. 5 sessions of treatment were provided for every subject. 14 subjects were chosen for data collection according to the inclusion criteria. The researcher was divide all participants into two groups and was code C1, C2, C3, C4, C5, C6, C7 for control group and E1, E2, E3, E4, E5, E6, E7 for experimental group.
Data was gathered through a pre-test, intervention and post-test and the data were collected by using a written questionnaire form which it formatted by the researcher. Pre-test was performed before beginning the treatment and the intensity of pain was noted with NPRS score and functional ability with ODI questionnaire form. The same procedure was performed to take post-test at the end of 5 sessions of treatment. Researcher provided the assessment form to each subject before starting treatment and after 5 sessions of treatment patient was instructed to put mark on the line of NPRS according to their intensity of pain. The researcher collected the data both in experimental and control group in front of the qualified physiotherapist in order to reduce the biasness. At the end of the study, specific test was done for statistical analysis.
Statistical analysis was performed by using Microsoft Office Excel 2013 and scientific calculator.
Statistical Test: For the significance of the study, a statistical test was carried out. Statistical analysis refers to the well-defined organization and interpretations of the data by systemic and mathematical procure and rules [24]. The U test was done for the analysis of the balance after six session treatment of both control and tail groups. Mann-Whitney U test is a non-parametric test that is simply compares the result obtained from the each group to see if they differ significantly. This test can only be used with ordinal or interval/ ratio data.
The formula of Mann-Whitney U test:
n1 = The number of the subjects in trail group
n2 = The number of the subject in control group.
nx = The number of the subjects of the group with larger rank total. Tx = The larger rank total.
Tx = The larger rank total.
Significant Level:In order to find out the significance of the study, the researcher calculated the “p” value. The p values refer the probability of the results for experimental study. The word probability refers to the accuracy of the findings. A p value is called level of significance for an experiment and a p value of < 0.05 was accepted as significant result for health service research. If the p value is equal or smaller than the significant level, the results are said to be significant.
Neural mobilization was applied by a neural mobilization technique certified physiotherapist to the patients of experimental group. Protocol is given in the Table-1 and Table-2.
According to McKenzie (1995) the treatment options are:
• Extension in lying
• Repeated extension in lying
• Extension in lying with self-overpressure
• Extension in lying with therapist-overpressure
• Sustained extension
• Extension in standing
• Extension mobilization
• Extension manipulation
• Rotation mobilization in extension
• Rotation manipulation in extension
• Sustained rotation
• Flexion in lying
• Flexion in standing
According to the directional preference these approaches were given to the patients. The patients who were given positive feedback in extension were given extension principle and the patient given positive feedback in flexion was given flexion principle [4].
Spinal Mobilization was given according to the Maitland Mobilization Grade in between Grade I-IV
Soft tissue technique was given by Deep Transverse Friction Massage (DTFM), Stroking and Effleurage techniques.
Neural Mobilization Procedure:Experimental group was given neural mobilization according to nerve involvement. Every patient of experimental group was given the sciatic nerve mobilization with the branch of tibial and peroneal nerve. Nerve mobilization techniques were performed with the patient in supine. The subjects remain relaxed and comfortable on the bed with feet uncrossed and arms at the side. The trunk and hips were in a neutral position Table 3.
Tibial Nerve Mobilization:The therapist position was next to the patient’s feet. The patient’s feet was dorsiflexed and everted. Then dorsiflexion and eversion were maintained while applying overpressure to knee extension and the symptoms were noted. Dorsiflexion, eversion and keen extension were maintained while passively raising the leg into hip flexion until the therapist felt the tension. To introduce additional traction (i.e. sensitization) into the proximal aspect of the sciatic nerve, hip adduction and internal rotation were added to the Straight Leg Raise.
Peroneal Nerve Mobilization:The therapist position was next to the patient’s feet. The patient’s foot was plantar flexed and inverted. Then plantar flexion and inversion was maintained while applying overpressure to knee extension and the symptoms were noted. Plantar flexion, inversion and knee extension were maintained while passively raising the leg into hip flexion until the therapist felt the barrier i.e. the point at which tension is initially felt. To introduce additional traction (i.e. sensitization) into the proximal aspect of the sciatic nerve, hip addition and internal rotation were added to the SLR.
The whole process of this research project was done by following the Bangladesh Medical Research Council (BMRC) guidelines and World Health Organization (WHO) Research guidelines. The proposal of the dissertation including methodology was approved by Institutional Review Board and obtained permission from the concerned authority of ethical committee of Bangladesh Health Professions Institute (BHPI). Again before the beginning of the data collection, researcher obtained the permission from the concerned authorities ensuring the safety of the participants. The researcher strictly maintained the confidentiality regarding participant’s condition and treatments.
The researcher obtained consent to participate from every subject. A signed informed consent form was received from each participant. The participants were informed that they had the right to meet with outdoor doctor if they think that the treatment was not enough to control the condition or if the condition become worsen. The participants were also being informed that they were completely free to decline answering any question during the study and were free to withdraw their consent and terminate participation at any time. Withdrawal of participation from the study would not affect their treatment in the physiotherapy department and they would still get the same facilities. Every subject had the opportunity to discuss their problem with the senior authority or administration of CRP and have any questioned answer to their satisfaction.
For this study 14 patients with radiating Low Back Pain were taken as sample from Musculo-skeletal outpatient unit of Center for Rehabilitation of Paralyzed (CRP), Savar to explore the effectiveness of Neural Mobilization for the treatment of radiating Low Back Pain.
In this study the results which were found have been shown in different bar diagrams, pie charts and Tables.
Variables in the study statistically significance at the following level of significance:
Mean difference in ODI between both groups in pre-test and post-test has been shown below in the bar chart (Figure 2).
The researcher interprets the results by using the values of pain intensity on NPRS that come from this study.
14 patients were enrolled and 7 patients were assigned to control group who receive only conventional physiotherapy. The rest of 7 patients were assigned to experimental group who received Neural Mobilization along with conventional physiotherapy. Mean difference of pain between pre-test and post-test of experimental group and control group were 4.28 and 2.27. Following application of treatment the study found that the experimental group showed a significant improvement (p <.05) in case of low back pain.
14 patients were enrolled and 7 patients were assigned to control group who receive only conventional physiotherapy. The rest of 7 patients were assigned to experimental group who received Neural Mobilization along with conventional physiotherapy. From them 7 patients have radiating pain up to thigh in experimental group and 6 patients had radiating pain up to thigh in control group
Mean difference between pre-test and post-test of experimental group and control group were 3.83 and 1.83. Following application of treatment the study found that the experimental group showed a significant improvement therapeutically but also showed not significant result statistically in case of radiating thigh pain.
14 patients were enrolled and 7 patients were assigned to control group who receive only conventional physiotherapy. The rest of 7 patients were assigned to experimental group who received Neural Mobilization along with conventional physiotherapy. From them 7 patients have radiating pain up to Leg in experimental group and 3 patients had radiating pain up to leg in control group.
Mean difference between pre-test and post-test of experimental group and control group were 4 and 2.58. Following application of treatment the study found that the experimental group showed a significant improvement therapeutically and showed significant result statistically (p <.05) in case of radiating leg pain.
The researcher interprets the results by using the values of disability on ODI that come from this study. Mean difference between pre-test and post-test of experimental group and control group were 30.51 and 9.81. Following application of treatment the study found that the experimental group showed a significant improvement in case of Disability.
The study was indicated a process that could be continuing to establish the result. Here the aim of this study could be achieved if the researcher could show effective support. The purpose of this study was to evaluate the effectiveness of the Neural Mobilization with conventional physiotherapy compare to only conventional physiotherapy for radiating low back pain.
In this experimental study 14 patients were enrolled and 7 patients were assigned to control group who receive only conventional physiotherapy. The rest of 7 patients were assigned to experimental group who received Neural Mobilization along with conventional physiotherapy. Each group attended for 5 sessions of treatment within two weeks in the Physiotherapy outpatient Unit of CRP, Savar in order to demonstrate the improvement. The outcome was measured by using Numeric Pain Measurement Scale (NPMS) for pain intensity and Oswestry Disability Index (ODI) for measuring disability. In this study there were total 14 participants. The mean age of experimental group was 42 years and the mean age of control group is 45 years.
Colakovic & Avdic in 2013 had a study on effects on neural mobilization on pain, straight leg raise and disability in patients with radicular low back pain. In their study there were 60 patients. The result of their study about age told that the mean age of experimental group was 42 years and the mean age of control group is 43 years [25].
The researcher found the male female ratio between 14 the patients, and 71% (n=10) were Male and 29% (n=4) were Female. Among them, In Experimental Group 36% (n=5) were Male and 14% (n=2) were Female and in Control Group 36% (n=5) were Male and 14% (n=2) were Female.
Colakovic & Avdic in 2013 in their study found 45% (n=27) Male and 55% (n=33) male. Among them, In Experimental Group 18.33% (n=11) were Male and 31.66% (n=19) were Female, and in Control Group 26.66% (n=16) were Male and 23.33% (n=14) were Female [25].
The researcher found significant improvement (p = <.05) of back pain in experimental group on NPRS. In Experimental group, the post-test Mean on NPRS was 2.27. Also there was significant improvement of pain in leg (p= <.05), as the post-test mean were consecutively 1.83 and 3 times more in experimental group than control group [26-30].
In 2011 Sahar had a study with 60 patients on Effectiveness of Neural Mobilization in treatment of Low Back Dysfunction. In his study he found significant improvement (p=0.06) of pain in experimental group on NPRS. In Experimental group, the post-test Mean on NPRS was 1.83 [19].
Kumar had a study on effectiveness of Neural Mobilization for the treatment of Low Back Pain with 30 patients. In his study he found significant improvement in case of Disability on ODI. Mean difference reducing disability between pre-test and post-test of experimental group and control group were 25.74 and 8.27 [16].
The result of the study have identified that the effectiveness of conventional physiotherapy with Neural Mobilization was better than the conventional physiotherapy alone for radiating Low Back Pain patients which was a quantitative experimental study. The result of the current study indicates that the conventional physiotherapy with Neural Mobilization can be an effective therapeutic approach for patient with radiating low back pain. Participants in the conventional physiotherapy with Neural Mobilization group showed a greater benefit than those in the only conventional physiotherapy group. The result indicate that the significant changes in both groups are due to the selection of a well- defined population of radiating low back pain patients using specific inclusion and exclusion criteria. It may be helpful for patient with radiating low back pain to increase return to normal daily activities, work and to measure longer term effects for determining cost effectiveness of Neural Mobilization in conjunction with conventional physiotherapy as an intervention for radiating low back pain.
We acknowledge Centre for the rehabilitation of the paralysed (CRP), Physiotherapy outpatient department of CRP for their contribution. We also acknowledge Neuro Orthopaedic Institute (Adelaide, Australia) who trained researcher regarding this effective technique of neural mobilization./p>

![]()

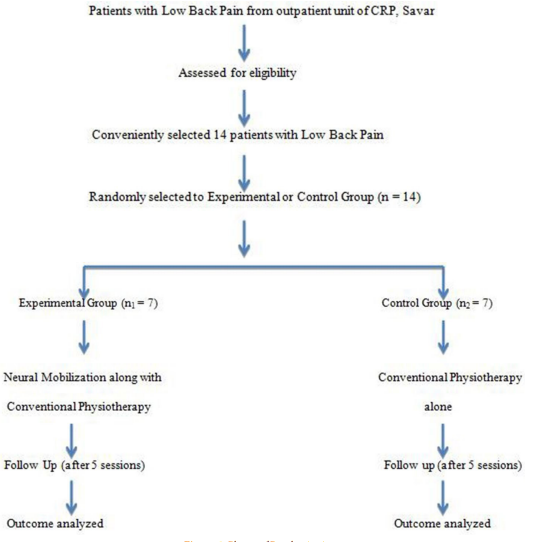 |
| Figure 1: Phases of Randomization |
 |
| Figure 2: Mean Difference in ODI Score in Both Groups |
Treatment option |
Duration/Repetition |
McKenzie Approach (Directional Preference) |
10 repetition in each session |
Lumber Mobilization (Maitland mobilization) |
5 minutes in each session |
IRR |
10 minutes in each session |
Soft tissue technique |
3 minutes |
Neural Mobilization |
5 repetition in each session |
Treatment option |
Duration/Repetition |
McKenzie Approach (Directional Preference) |
10 repetition in each session |
Lumber Mobilization (Maitland mobilization0 |
5 minutes in each session |
IRR |
10 minutes in each session |
Soft tissue technique |
3 minutes |
Nerve Mobilization |
Tibial Nerve |
Peroneal Nerve |
Hip |
Flexion with adduction and internal rotation |
Flexion with adduction and internal rotation |
Knee |
Extension |
Extension |
Ankle |
Dorsiflexion with eversion |
Planter flexion with inversion |
Experimental Group |
Control Group |
||
Subjects |
Age (Years) |
Subjects |
Age (Years) |
E1 |
40 |
C1 |
48 |
E2 |
45 |
C2 |
25 |
E3 |
45 |
C3 |
53 |
E4 |
46 |
C4 |
46 |
E5 |
50 |
C5 |
55 |
E6 |
45 |
C6 |
55 |
E7 |
26 |
C7 |
35 |
|
Mean Age= 42 years |
|
Mean Age= 45 years |
Sex |
Frequency |
Male |
71% (n=10) |
Female |
29% (n=4) |
Variables |
Acute |
Sub acute |
Chronic |
No pain |
Low back pain |
29% (n=4) |
21% (n=3) |
50% (n=7) |
0% (n=0) |
Thigh pain |
29% (n=4) |
14% (n-2) |
50% (n=7) |
7% (n=1) |
Leg pain |
29% (n=4) |
21% (n=3) |
50% (n=7) |
0% (n=0) |
Causes |
Frequency |
Trauma/injury |
14% (n=2) |
Bad Posture |
43% (n=6) |
Heavy weight lifting |
29% (n=4) |
Unknown cause |
14% (n=2) |
Control Group |
Back Pain |
Thigh Pain |
Leg Pain |
|||
Pre-test |
Post-test |
Pre-test |
Post-test |
Pre-test |
Post-test |
|
Mean |
6.14 |
3.57 |
5.16 |
3.33 |
6.43 |
3.85 |
Mean Difference |
2.57 |
1.83 |
2.58 |
|||
Experimental Group |
Back Pain |
Thigh Pain |
Leg Pain |
|||
Pre-test |
Post-test |
Pre-test |
Post-test |
Pre-test |
Post-test |
|
Mean |
6.42 |
2.14 |
6.14 |
2.29 |
6.14 |
2.14 |
Mean Difference |
4.28 |
3.85 |
4 |
|||
No. |
Variables |
Observed ‘u’ value |
Observed P value |
Level of significance |
1 |
Low back pain |
4 |
<.05 |
Statistically significant |
2 |
Radiating pain up to thigh |
23.5 |
|
Statistically not significant |
3 |
Radiating pain up to leg |
3 |
<.05 |
Statistically significant |




































