Open Access
Research Article
Max Screen
ISSN: 2639-9296
Copyright: © 2024 Miriam Gallo Afflitto. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Purpose:To describe a case of a 39-years-old man with marked scleral thinning secondary to proton beam therapy for choroidal melanoma.
Observations:The patient underwent multiple unsuccessful reconstructive surgical procedures complicated by failure and enucleation was finally suggested. However, he started improving following homologous serum drops administration.
Conclusions:Serum eye drops seem to be a promising strategy to enhance engraftment and could be proposed as standard of care to avoid graft failure even in the most severe cases. To the best of our knowledge, this is the first report describing this treatment strategy.
Keywords: Scleral melting; choroidal melanoma; homologous serum eye drop; graft failure; proton beam therapy
The most common malignant intraocular tumor in adults is uveal melanoma. The uveal tract, a layer underlying the sclera of the eye, includes the iris, ciliary body and choroid. Around 95% of uveal melanomas arise from the choroidal melanocytes [1, 2] , but is distinct from cutaneous melanoma in that it has different molecular drivers, metastatic patterns, and tumour-immune microenvironment [3, 4, 5]. UM incidence varies by sex, race, and country. Males have a 30% greater incidence than females.
In the United States, the annual incidence of ocular melanoma is approximately 6 per million, with a male predominance and a male-to-female ratio of 1.29. Important cytogenetic and genetic risk factors for melanoma development include chromosome 3 haplogroups, guanine mutations in the nucleotide-binding protein GNAQ/GNA11, and braca1-associated protein 1 (BAP 1) deletion [6-8].
The diagnosis of UM is based on clinical examination (slit lamp fundus biomicroscopy and indirect ophthalmoscopy) together with ultrasonography of the eye. UM can be missed unless the fundus is meticulously examined after full pupillary dilatation. Digital photography is most useful for documenting tumor size and location. When a choroidal tumor is large or peripheral, ultra- -widefield fundus cameras are especially helpful. In general, people who have had eye melanoma should have regular checkups throughout their lifetime. In general, people who have had radiation therapy or chose active surveillance are usually monitored every 3 to 6 months. Patients who had an eye surgically removed should receive a yearly eye examination.
The main purpose of treating primary uveal melanoma is to prevent distant metastasis and preserve the globe and vision. The treatment strategy for ocular melanoma should be individualized. Several therapies can control the growth of the local tumor and even conserve the vision of the affected eye [9, 10]. These include radiotherapies such as brachytherapy (plaque radiotherapy with Ru106 or I125), proton beam (PBRT), stereotactic radiotherapy and local resection [11].
Plaque brachytherapy is currently the most commonly used eye-preserving treatment for small to medium-sized uveal melanomas. Proton beam radiation therapy is indicated for tumors of significant size, challenging shape, and location, while removal of the eye is limited to advanced tumors [12, 13]. Enucleation and orbital exenteration are necessary in patients with massive tumors [11].
The most common ocular complications associated with radiotherapy include dry eye, scleral melting, cataract, radiation corioretinopathy, maculopathy, toxic tumor syndrome, optic neuropathy, neovascular glaucoma and rarely scleral melting. Sclera is not frequently involved due to its radioresistant nature of avascular and hypocellular tissue [14]. According to Pietro P. Radin et al. scleral necrosis seems to be related to a higher incidence of cataract, retinopathy, and maculopathy, because of higher radiation doses released to larger tumors [15].
Furthermore, scleral necrosis is rarely eye-threatening, except for perforation sequelae, which are estimated to occur in 4-8.5% of patients [14, 15]. Observation is recommended in these cases since half of them remain usually stable over time [14]. Multiple therapeutic options are today available including artificial lubrication with tears, gels, or ointments; prednisolone acetate 1% for of early onset cases; tissue glue; conjunctival/flap graft; amniotic membrane transplantation; scleral or corneal patch graft; dermal patch graft; vital Tenon’s fascia transposition; hyperbaric oxygen therapy; enucleation [14-17].
A recent study discovered that light-activated molecules, like the drug AU-011, appear promising for treating small choroidal melanomas without radiation. AU-011 is a first-in-class targeted therapy in development for the primary treatment of ocular melanoma. The therapy consists in the injection of viral nanoparticle conjugates that selectively bind to tumor cells in the eye and can be activated by a diode laser to destroy the target cells while sparing key structures in the eye, which may help preserve patients vision [18].
Despite successful local primary tumor treatment, approximately 50% of patients with UM will develop metastasis within 10 years of primary tumor diagnosis [19], preferentially in the liver and unfortunately there are limited therapeutic approaches for metastatic disease, including immunotherapy, which unlike cutaneous melanoma, has been mostly ineffective for patients with uveal melanoma. Several clinical and histological factors are associated with metastasis, including cell type, pigmentation, tumor size, ciliary body involvement, and intra- and extra-scleral extension [20].
The therapeutic possibilities are extremely limited in uveal melanoma with metastatic disease. A promising treatment modality is immunotherapy, particularly cytokine modulation and immune checkpoint blockade [21]. Compared to cutaneous melanoma (CM), the clinical benefit of immunotherapy for metastasis in the case of melanoma uveal is limited by its low mutation burden and “immune privilege,” particularly checkpoint blockade. Some more classic prognostic associations with histological type, size, localization and vascularity are known for some time, others, concerning tumor genetics, are under investigation. Recently the FDA approved Tebentafusp, a bispecific antibody engaging T cells with gp100 on HLA-A*02:01, as the first drug of its class to specifically treat metastatic UM [22].
We report on a case of a scleral melting after proton beam radiotherapy for uveal melanoma. The tissue weakness was successfully repaired with homologous serum eye drops after the third attempt with scleral patch grafting. In recent years the use of derivative eye drops from serum has gained wide acceptance for the treatment of ocular surface disorders. Liu L. described the epitheliotrophic potential of serum for the ocular surface due to its content of growth factors and vitamins [23].
Blood-derived eye drops have recently become more popular due to their properties that mimic the components of natural tears. According to the TFOS II report [24] they are indicated as a third-line option for severe dry eye disease. Blood-derived eye drops such as autologous serum (AS) or platelet-rich plasma (PRP) are composed of nutrients and growth factors that are not available in artificial tears. These biological tear substitutes contain substances P, fibronectin, platelet-derived growth factor, nerve growth factor, epidermal growth factor and transforming growth factor-β, which not only have anti-inflammatory properties but also initiate cell differentiation and also regulate the wound healing [25, 26]. There is clear evidence that blood-derived products are superior and more effective than artificial tears [27, 28] as their composition is similar to natural tears and autologous preparations.
The effects of blood-derived products on proliferation, vitality and migration of corneal epithelial cells have been well documented in the past by both in vitro and in vivo experimental studies[23, 29, 30]. In particular, these products have been used for the treatment of a variety of ocular surface diseases, including mainly dry eye disease, persistent corneal epithelial defect, corneal ulcer, chemical burn, recurrent corneal erosion and limbal stem-cell deficiency.
Homologous serum eye drops are obtained from patients' peripheral blood serum. 50-100 ml of whole blood is collected patient and is left for 2 hours at room temperature without any anticoagulant to achieve a complete coagulation. Next, the blood is centrifuged at 3000 g for 15 minutes to separate completely serum from solid components. The supernatant is then collected and diluted with balanced salt solution (BSS) at the desired concentration. Autologous serum can be stored at -20°C for various periods months, and the maximum retention interval varies depending on the local legislation of each individual country. It should be kept away from light to avoid degradation of vitamin A [31]. We describe a new approach to manage postoperative graft therapy.
A 39-years-old Causasian male with no other comorbidities presented to the Emergency Department complaining of non-specific visual disturbance in his left eye for the last three months. The left eye examination showed an inferotemporal choroidal melanoma with perilesional exudative retinal detachment. The ocular ultrasonography showed a maximal tumor base of 13.3 x 10.8 mm with a thickness of 8.1 mm. The right eye was unremarkable. The best corrected visual acuity (BCVA) was 20/20 in both eyes.
The patient was then referred to an ocular oncology center for radiotherapy treatment, after applying tantalum clips and intravitreal injection of triamcinolone acetonide (40 mg/ml). The patient was cortico-responder and antiglaucoma drops were prescribed to treat secondary ocular hypertension.
One year after proton beam radiotherapy, the diagnosis of radiation retinopathy was confirmed by fluorescein angiography and Aflibercept intravitreal injections with laser photocoagulation was performed on the peripheral non-perfusion and avascular retina.After seven months a conjunctival reaction in the area related to inferotemporal tantalum clip was observed and it was treated by topical steroids. Subsequently, due to the persistent granulomatous conjunctival reaction not responsive to medical therapy and after 2 days the patient underwent removal of a tantalum clip.
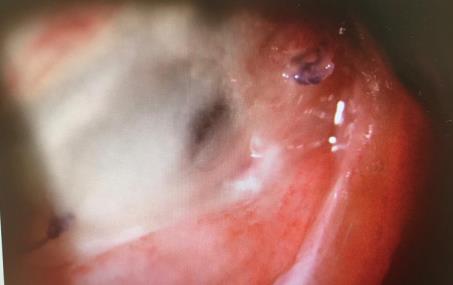
Three months later, an attempted conjunctivoplasty was performed for conjunctival suture dehiscence. After two years from proton beam radiotherapy he developed scleral melting (Figure 1) and he underwent wound curettage and scleral patch grafting
Unfortunately, thirteen days later, due to the failure of the previous surgical approach, the decision was made for an autologous oral mucosal graft combined with a scleral patch. The procedure failed again. After three weeks, for the observation of hypotony and enlargement of the area of scleral necrosis, a further scleral patch with amniotic membrane graft was performed. Homologous serum eye drops were prescribed postoperatively with the option of eye enucleation in case of failure. The patient administered the autoserum eye drops 8 times a day in the affected eye and examined every week with photography of the anterior segment for a month and then every 15 days.
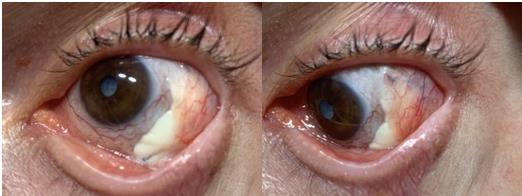
After one month of homologous serum eye drops administration, for the first time, we observed vascularization at the temporal edge of the scleral patch. In four months it progressively extended to almost the entire surface of the scleral flap (Figure 2) leaving uncovered the only nasal portion.
One year later the patient underwent total cataract surgery with intraocular lens implantation and intravitreal injection of Aflibercept, being the scleral flap fully vascularized and engrafted.
At his last examination, the choroidal melanoma remained stable, showing no signs of growth and the patient continued treatment with intravitreal injections of Aflibercept for radiation maculopathy. Furthermore the patient showed no signs of graft infection, necrosis or reoccurrence of inflammation (Figure 3) and the best corrected visual acuity (BCVA) was 20/63 in the treated eye.
Scleral necrosis subsequent to proton beam therapy for uveal melanoma is a rare complication, accounting for about 1% of cases. Predictive factors are tumor dimension 6 mm, anterior location, type and radiation dose applied to the sclera, ocular hypertension [14, 32].
Before the COMS was published, showing the equal effect of radiotherapy on patients’ life expectance, enucleation was considered the standard treatment for choroidal melanoma. Today, globe-preserving therapies are the choice to guarantee a better quality of life. Secondary enucleation in still used in case of complications like neovascular glaucoma, pain, persistent exudative retinal detachment, phthisis, functional loss or ocular inflammation. The drawbacks of a higher topical tumor control are worst cosmetical, psychological and quality of life aspects. [32, 33]
On average, scleral necrosis after radiation therapy appears in a range between 27 and 70.4 months, apart from some few cases of quicker appearance in the immediate postoperative period [14, 15, 34].
Pathophysiology is related to direct radiation effect on the sclera, inflammation and local ischemia related to surgical procedures and worsened by tumor necrosis [32].
Scleral necrosis is asymptomatic and its diagnosis is based on the clinical appearance. Differentiation from neoplastic recurrence with extraocular extension is not simple, but mandatory to avoid unnecessary enucleations [15, 32].
Ultrasound can be used to detect thinning, while ophthalmological examination should be performed to identify the presence of a blue discoloration in the Tenon’s capsule, an increased transillumination, or a progressive decrease in the intraocular melanoma thickness. Posterior necrosis can be difficult to detect during routine funduscopic examinations and it requires a high level of suspicion based on other clinical manifestations such as extreme hypotony and unexplained vision loss to confirm the diagnosis. [14, 15, 32].
Our case illustrates multiple strategies sometimes necessary to achieve local control of scleral thinning as a complication of uveal melanoma after radiotherapy. Specifically, this was managed using a primary conjunctivoplasty, scleral patch application, autologous oral mucosal patch graft plus scleral patch, and finally scleral patch plus amniotic membrane graft. Only serum eye drops appeared to be therapeutically effective and able of induce and provide a sustained vascularization and engrafting.
In our experience, homologous serum eye drops are able to promote the engraftment of the scleral graft. Further studies are needed to demonstrate its effectiveness and support its use as a protocol.
No funding or grant support
The following authors have no financial disclosures
All authors attest that they meet the current ICMJE criteria for Authorship
None

![]()

 |
 |
 |




































