Open Access
Research Article
Max Screen
ISSN: 2639-9296
Copyright: © 2021 Zhou M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background:This report describes a rare case of frosted-branch angiitis associated with poststreptococcal uveitis syndrome.
Case presentation: The case was a 7-year-old girl who had complained of bilateral blurry vision for 1 week. Five weeks earlier, she suffered from a flu-like episode with fever, sore throat, and skin rash, and received an irregular dose of oral amoxicillin for 4 days after a diagnosis of scarlet fever. Our clinical examination revealed bilateral panuveitis with frosted-branch angiitis. Systematic examinations were normal, except for an elevated anti-streptolysin O antibody titer (868.0 IU/ml) and an elevated white blood cell count (11.61 × 109 /L). The diagnose of poststreptococcal uveitis syndrome was made and systemic prednisone and penicillin were given. After treatment, the ocular inflammation and perivascular sheathing were markedly alleviated. The macular edema and subretinal fluid disappeared and visual acuity improved, but the defection of outer retinal structure on optical coherence tomography (OCT) scans persisted. The defection of interdigitation zone (IZ) on foveal persisted until one year after initial visit.
Conclusion:Poststreptococcal uveitis syndrome should be considered in the etiology of acute bilateral frosted-branch angiitis in children.
Keywords: Frosted-branch Angiitis; Poststreptococcal Uveitis Syndrome; Spectral Domain-Optical Coherence Tomography; Interdigitation zone
Poststreptococcal syndrome is believed to be an immunity-mediated sequela of a group a streptococcal infection. Rheumatic fever, glomerulonephritis, and polyarthritis are well-recognized features of this syndrome [1]. Poststreptococcal uveitis syndrome was relatively rare since it was first reported in 1991 [2]. The poststreptococcal uveitis syndrome tended to occur 2–4 weeks after the initial infection, and predominantly affected young patients with bilateral non-granulomatous anterior inflammation [3-6]. There are also cases of retinal vasculitis or papillophlebitis reported [7-10]. The present report describes a case of frosted-branch angiitis associated with poststreptococcal uveitis syndrome that developed 4 weeks after the initial streptococcal infection. The Spectral Domain- optical coherence tomography (OCT) and ultra-wide-field retinal imaging were used as follow-up tools. The recovery of retinal function and morphology were evaluated during 1-year follow-up.
A 7-year-old girl presented at the local clinic (Traditional Chinese Medicine Hospital, Zhangjiagang, Nanjing, Jiangsu Province, June 28, 2019) after complaining of bilateral blurry vision for 1 week. Five weeks earlier, she suffered from a flu-like episode with fever, sore throat, and skin rash, and received an irregular dose of oral amoxicillin for 4 days after a diagnosis of scarlet fever. The bilateral macular OCT scans were acquired and demonstrated dominant macular edema (Figure 1). The Benzylpenicillin sodium (50,000UI/kg/day, IV) and methylprednisolone (25 mg per day, IV) was prescribed. One week later, she came to our uveitis clinic with 20/100 OD and 20/200 OS. A slit-lamp examination showed bilateral mild conjunctival congestion, moderate flare and 2+cell reaction in the anterior chamber of both eyes. No synechiae were seen. Ophthalmoscopy revealed diffuse, white perivascular sheathing of the arteries and veins, tortuous and dilatated veins in both eyes (Figure 2). Fluorescein angiography showed extensive dye leakage from almost all vessels (Figure 2). OCT showed the resolution of the macular edema and subretinal fluid, but the disruption of the outer retinal structure remained (Figure 2).
Laboratory findings showed mildly elevated white blood cells (11.61 × 109/L). The results of a T-spot test and serological tests for syphilis, human immunodeficiency virus, hepatitis C virus, hepatitis B virus, toxoplasmosis, cytomegalovirus, varicella zoster virus, and herpes simplex virus were all negative. Her antinuclear antibody and antineutrophil cytoplasmic antibody levels were normal. The patient was HLA-B27-negative. However, her anti-streptolysin O (ASO) antibody titer was elevated (868 IU/mL; normal < 200 IU/mL).
Based on these findings, the subject was diagnosed with frosted-branch angiitis associated with poststreptococcal uveitis syndrome. She was given one injection of benzyl penicillin (800,000 IU) and systemic oral prednisolone at an initial dose of 1 mg/kg bodyweight/day, which was gradually tapered over 3 months. The ocular inflammation and perivascular sheathing were markedly alleviated by this treatment (Figure 3). One month after treatment, the patient’s visual acuity improved to 20/20 OD and 20/20 OS, her ASO titer was normal (68.9 IU/mL), and the intact ellipsoid zone (EZ) could be seen on OCT scan, but the interdigitation zone (IZ) was defected. At the 3-month follow-up, the IZ was still defect. Partial IZ (outside foveal) could been seen on OCT scan at 6-month follow-up. One year after treatment, the foveal IZ could been seen in both eyes (Figures 4 and 5) and no signs of recurrence were observed.
Poststreptococcal syndrome is believed to be an immunity-mediated sequela of a group a streptococcal infection [1]. Rheumatic fever, glomerulonephritis, and polyarthritis are well-recognized features of this syndrome [1]. Several cases [2-4] of poststreptococcal uveitis syndrome have been reported since it was first reported in 1991 [2]. In prior cases, poststreptococcal uveitis syndrome tended to occur 2–4 weeks after the initial infection, and predominantly affected young patients (96% of those affected were < 40 years of age and more than half were < 15 years of age), with bilateral nongranulomatous anterior inflammation, but rarely vitritis or retinitis [7-10]. The present report describes a case of frosted-branch angiitis associated with poststreptococcal uveitis syndrome that developed 4 weeks after the initial streptococcal infection.
Frosted branch angiitis occurs in young, healthy individuals who typically have acute bilateral visual loss, associated with anterior and posterior segment inflammation [11]. Fluorescein angiography demonstrates leakage of dye from the vessels, but no evidence of decreased blood flow or occlusion (Figure 2). Kleiner [12] classified the patients with the appearance of frosted branch angiitis into three subgroups-First are patients with lymphoma or leukemia [12] whose disease is due to infiltration with malignant cells. Second is the group of patients who have associated viral infections [13] or autoimmune disease [14]. Finally, there is the group of otherwise healthy young patients described acute idiopathic angiitis [15]. In our patient, a flu-like episode with fever preceded the ocular symptoms and her high ASO titer suggested a streptococcal infection. After treatment, her ASO titer decreased to a normal level. The diagnose of frosted branch angiitis associated with poststreptococcal uveitis syndrome was made. The immunological mimicry between the retinal S-antigen and the group A streptococcal M protein has been suggested to underlie the pathogenesis of poststreptococcal uveitis syndrome [16].
Patients with poststreptococcal uveitis syndrome and mild anterior uveitis respond well to topical steroids. If the posterior segment is compromised, a systemic corticosteroid should be administered (prednisolone 1 mg/kg/day) [17]. Sometimes, cyclosporin A and methotrexate may be used as an alternative treatment [18]. Clinical improvement and the absence of relapse can be corroborated by the reduction in the ASO titer. Antibiotics should be prescribed to patients with acute streptococcal infection (clinical or subclinical) or if a streptococcal reservoir is suspected [4,17]. Because the patient’s white blood cell count was slightly elevated and accompanied by elevated ASO, she was prescribed benzathine penicillin (800,000 IU as a single dose). One week later, systemic oral prednisolone, at an initial dose of 1 mg/kg bodyweight/day, was given and gradually tapered over 3 months. The patient’s ocular inflammation and perivascular sheathing were markedly alleviated by this treatment, her visual acuity improved, and her ASO titer returned to normal. The resolution of the macular edema and subretinal fluid was occurred one week after low doses of methylprednisolone (25 mg per day, IV) given, although the disruption of the outer retinal structure remained. This reminded the good prognosis of this disease. The recovery of outer retina structures was relatively delayed and the defection of IZ persisted until one year after treatment.
We suggest that poststreptococcal uveitis should be considered in the differential diagnosis of acute frosted-branch angiitis in children. The patient should be asked about any signs or previous clinical history of streptococcal disease, such as fever, sore throat, or recurrent tonsillitis, and the ASO titer should be measured.
This study was approved by the Ethics Committee of the Eye and Ear Nose Throat Hospital of Fudan University, Shanghai, China and all procedures conformed to the tenets of the Declaration of Helsinki.
The written informed consent was obtained from the child’s father; Consent to publish has been obtained from the child’s father.
All data generated and analyzed in this study are included within this manuscript.
The authors declare that they have no competing interests.
This work was supported by research grants from the Shanghai clinical three-year action plan-major clinical research project (SHDC2020CR2041B) for design, data collection and analysis; The Youth Project of the National Natural Science Fund (81800846) for article design, write, language modification and publication.
RPG performed the data acquisition and prepared the manuscript. RPG and BYL gave suggestions on the manuscript. MZ and QMS did the surgery and participated in design of the study and revision of the manuscript. All authors read and approved the final manuscript.
Not applicable.

![]()

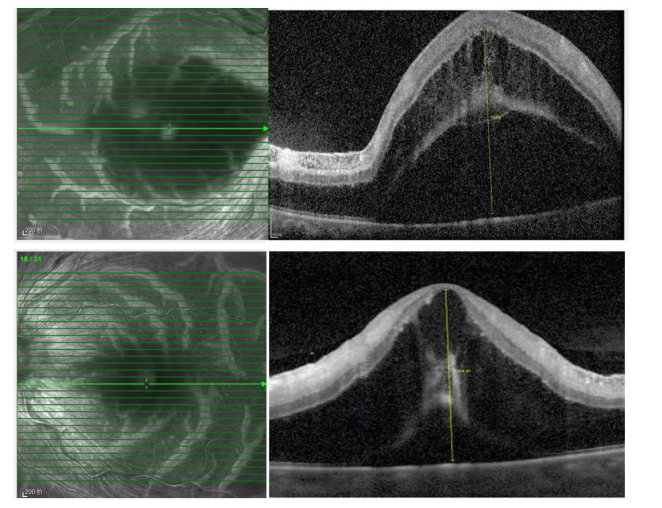 |
| IR: Infrared; OCT: Optical Coherence Tomography Figure 1: The IR and OCT images at initial visit demonstrated prominent macular edema and subretinal fluid on the both eyes |
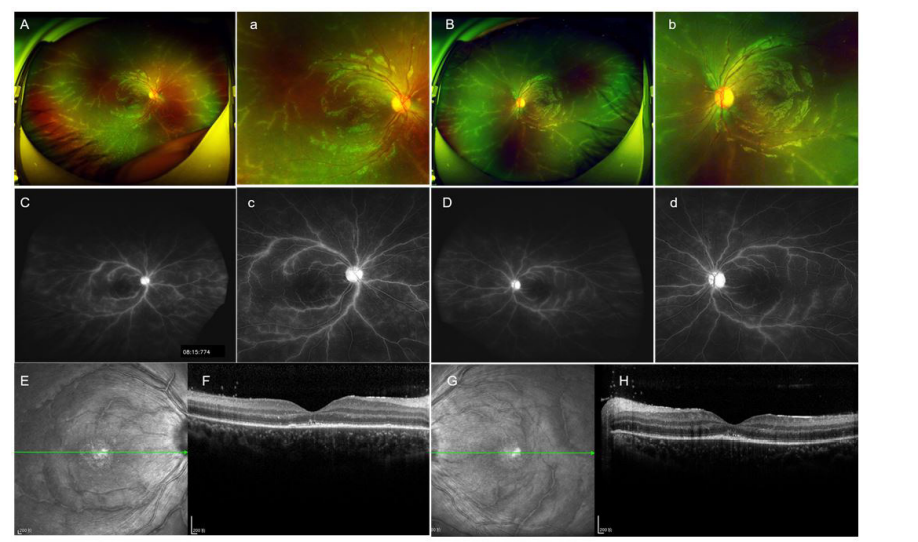 |
| IR: Infrared; OCT: Optical Coherence Tomography Figure 2: The fundus examinations on the first visit in our hospital (A and B) wide-field fundus images showed white retinal perivascular sheathing in both eyes; (C and D) wide-field fluorescein angiographic images demonstrated extensive leakage from the retinal vessels in the late phase; a-d were the magnification of A-D, respectively; (E, F, G and H) IR and OCT images showed resolution of the macular edema and subretinal fluid, but the disruption of the outer retinal structure remained |
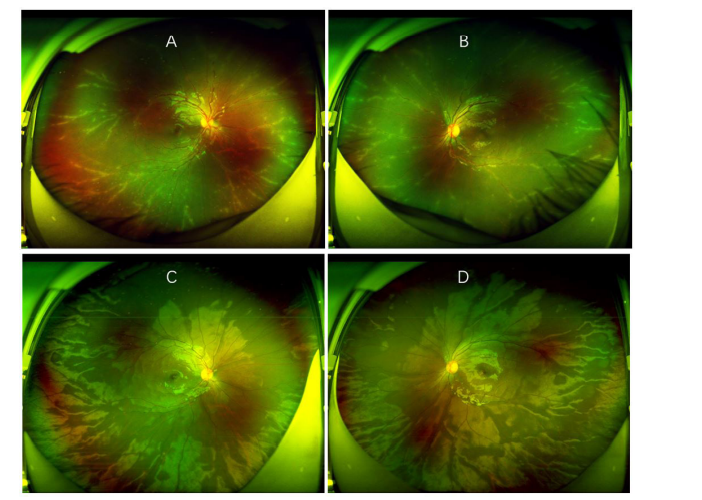 |
| Figure 3: The wide-field fundus images of both eyes during follow-up (A and B) and (C and D) were 1 week and1 month after benzyl penicillin combined oral prednisolone treatment, respectively. The perivascular sheathing was markedly alleviated at 1 week after treatment and disappeared at 1 month |
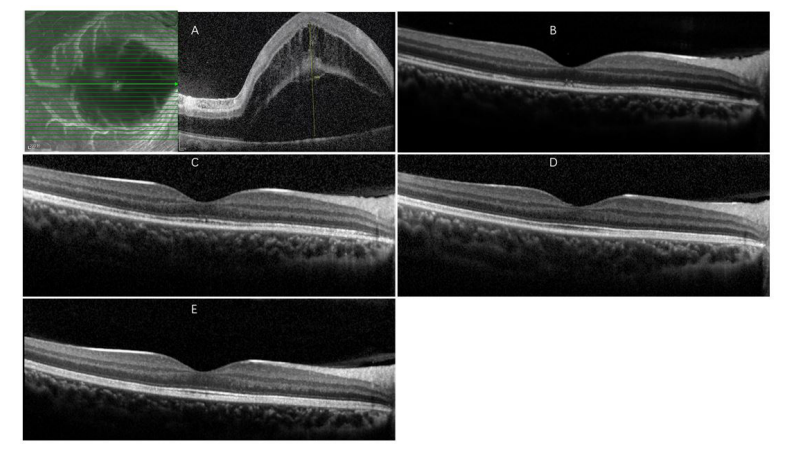 |
| OCT: Optical Coherence Tomography; IZ: Interdigitation Zone; EZ: Ellipsoid Zone Figure 4: The OCT images of right eye during 1year follow-up time (A) first visit to local hospital; (B) 1 month after benzyl penicillin combined oral prednisolone treatment; (C, D and E) were 3months, 6months and 1year after treatment, respectively. One month after treatment, the intact EZ could been seen on OCT scan, but the IZ was defected. At 3-month follow-up, the IZ was still defect. Partial IZ (outside foveal) could been seen on OCT scan at 6-month follow-up. One year after treatment, the foveal IZ could been seen |
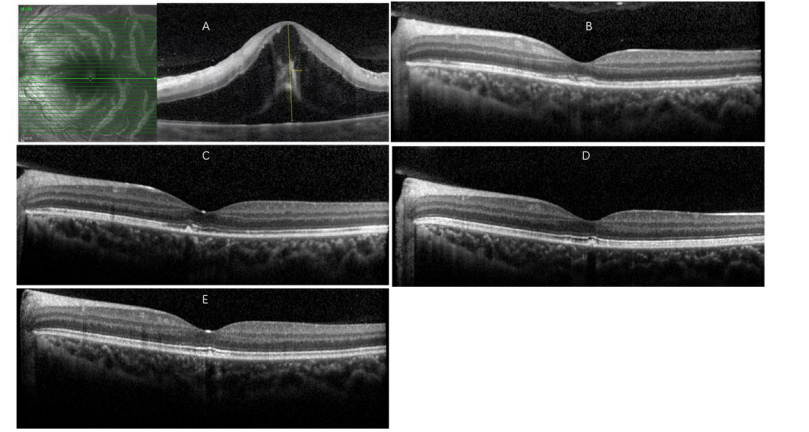 |
| OCT: Optical Coherence Tomography; IZ: Interdigitation Zone; EZ: Ellipsoid Zone Figure 5: The OCT images of left eye during 1year follow-up time (A) first visit to local hospital; (B) 1 month after benzyl penicillin combined oral prednisolone treatment; (C, D and E) were 3months, 6months and 1year after treatment, respectively. One month after treatment, the intact EZ could been seen on OCT scan, but the IZ was defected. At 3-month follow-up, the IZ was still defect. Partial IZ (outside foveal) could been seen on OCT scan at 6-month follow-up. One year after treatment, the foveal IZ could been seen |




































