Open Access
Research Article
Max Screen
ISSN: 2767-9292
Copyright: © 2024 Münevver Kıyak. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Objective:This study was explored the impact of Nihavent theme on decreasing of adaptation difficulty in patients with Alzheimer’s disease.
Materials and methods: The study was conducted with a total of 30 patients, 15 patients in the intervention group and 15 patients in the control group. Before the application, The Descriptive Characteristics Data Form and Assessment Scale of Adaptation Difficulty for the Elderly were administered to both groups. The patients in intervention group had music sessions for 12 weeks. Patients in the control group received standard care but did not participate in the specific intervention. One week after the music session completed, the Assessment Scale of Adaptation Difficulty for the Elderly was re-administered to both groups.
Results:The Assessment Scale of Adaptation Difficulty for the Elderly pre-test mean score; of the intervention group was 1.43 ± 0.44 and of the control group was 1.51 ± 0.58. The Assessment Scale of Adaptation Difficulty for the Elderly posttest mean score; of the intervention group was 0.66 ± 0.24 and of the control group was 1.29 ± 0.59. It was determined that there was a significant difference (p< 0.05) between the Assessment Scale of Adaptation Difficulty for the Elderly pre-test mean scores and post-test mean scores of intervention group.
Conclusion:It was determined that the music played had a positive effect on decreasing adaptation difficulty of the Alzheimer’s patients.
Keywords: Alzheimer’s disease; adaptation difficulty; music; nursing care
In the early stages of Alzheimer's disease, memory loss and cognitive decline are the primary symptoms. As the disease progresses, it can lead to personality and behavioral changes, psychological problems, an inability to perform mental activities, impairments in perception and judgment, speech and motor difficulties. Depending on the affected areas of the brain, patients may experience agitation, anxiety, depression, apathy, irritability, abnormal motor activity, and sleep disturbances. These can significantly hinder patient adaptation with care and treatment, creating substantial challenges. To overcome these challenges and ensure proper treatment and care, patients need to adapt to their caregivers, medical treatment and social environment [1, 2].
Music composed of simple harmonic motions has both physiological and psychological benefits for our bodies. Music helps patients strengthen their interpersonal relationships, express their emotions more easily, and utilize coping mechanisms for dealing with illnesses. It also reduce psychotic symptoms in patients, ensure patients adaptation the treatment and care. Additionally, music enhance social interaction and improve the quality of life for individuals [3-5].
Numerous studies have investigated the effects of music on Alzheimer's patients. In a study by Gómez-Gallego et al. (2021), patients were divided into three groups: active music intervention, receptive music intervention and a control group. Music therapy was applied twice a week for 45 minutes for 12 weeks. The study found that the active music intervention group showed a greater improvement in cognitive deficits, behavioral symptoms and functional status compared to both the receptive music intervention and control groups [6]. Lyu et al. investigated the effects of music therapy on cognitive function and well-being in Alzheimer's patients. The study assessed participants' short-term and long-term memory by testing their ability to recall 15 spoken words immediately and after 30 minutes. The results indicated that music therapy improved memory and language ability in patients with mild dementia, while in patients with moderate or severe dementia, it reduced psychiatric symptoms (delusions, hallucinations, agitation/aggression, dysphoria, anxiety, euphoria, apathy, abnormal motor activity) and caregiver burden [7].
In a study by Innes et al. Alzheimer's patients were subjected to 12 weeks of music therapy. The results indicated that the patients improvement in memory function (executive functions, working memory, processing speed and attention), psychological state and cognitive performance [8]. In a study by Liu et al. 50 Alzheimer's patients were randomly assigned to either an intervention or control group. The intervention group received 60-minute group music sessions with percussive instruments once a week for 12 weeks. The control group received relaxation and reading sessions for the same duration and under the same conditions. The results showed a significant decrease in anxiety levels in the intervention group after the music sessions, while no significant change was observed in the control group [9].
Nihavent theme has a relieving, delightful and refreshing effect on listeners [10]. In line with this, the Nihavent theme was chosen for this study. This study aimed to determine the effect of the Nihavent theme on decreasing adaptation difficulty in Alzheimer's patients.
This is a randomized- controlled, pre-test, post-test, experimental study explored the impact of the Nihavent theme on decreasing of adaptation difficulty in patients with Alzheimer’s disease.
This study was conducted an Alzheimer Elderly Care Center in Eskisehir-Turkey.
The study population consisted of 40 patients with middle and advanced stage Alzheimer’s disease staying at the Alzheimer Elderly Care Center in Eskisehir-Turkey. The research participants were individuals who fulfilled all the predetermined inclusion criteria. A power analysis was performed, and minimum sample size was calculated as sevenfor 0.05 alpha value and 98% power level. The study employed a sample of 30 patients, equally divided into an intervention group (n=15) and a control group (n=15).
Power analysis was repeated with the results of the study, and a power level of 0.9668 was achieved with 30 patients.
The inclusion criteria included Alzheimer’s patients over the age of 18 who were conscious able to communicate and active (active elderly individuals were defined as those who could carry out daily activities such as eating, going to the toilet, and walking on their own).
Individuals were excluded from the study in case of changes in their medical diagnosis, consciousness, medical treatments or if they had a changing in emotional state (sadness, crying) during the application. To maintain focus on the specific effects of the intervention, individuals with complex conditions like cancer were not included in the study
Data collection tools included the Descriptive Characteristics Data Form which was created by the investigator in accordance with the relevant literatüre [11, 12], Emotional Status Evaluation Form [13] and Assessment Scale of Adaptation Difficulty for the Elderly (ASADE).These were all used as data collection tools. A validityand reliability study of ASADE was conducted by Şişman and Kutlu (Cronbach’s alpha value 0.93) [12]. A CD including instrumental songs in Nihavent theme, sound system and computer were used for the application. A written consent form was used to obtain patient consent for the study.
This form was created by the researchers as a result of literature review. It is a form consisting of a total of 10 questions to obtain data about the patients' socio-demographic characteristics (age, gender, educational status, marital status, child), diseases and care status (presence of chronic disease, time of diagnosis, duration of stay in the nursing home) [11,12].
This form was created by the researchers as a result of literature review. It is a form consisting of 6 items that includes negative psychological and behavioral states (agitation, aggression, euphoria, irritability, abnormal motor behaviors, crying) that may occur in patients during music sessions. It was created to evaluate these negative situations that may arise in patients during sessions and to prevent patients from being affected by these situations [13].
This scale was developed by Şişman and Kutlu in 2016 to determine the adaptation of elderly individuals and its validity and reliability were determined. Cronbach's alpha value of the scale is 0.93. It is a likert-type scale consisting of 24 items questions. In the scale, the elderly individual is discussed in four dimensions: “Role and self-actualization mode, interdependence mode, physiological status mode and self-concept mode ". Role and self-actualization mode; it is the situation in which an individual shows the behaviors that the society expects from him, depending on the position he has in the society.
Interdependence mode; it is the dimension that covers the individual's relationships with people and deals with birth, love and appreciation situations in his life. Physiological status mode; it includes the individual's physical responses to environmental factors (oxygen, nutrition, elimination, activity and rest, protection). Self-concept mode; it is the state of respect and feeling valued that the individual shows towards himself. The lowest average score that can be obtained from the scale is 0 and the highest is 3. As the score an individual gets from the scale decreases, the level of compliance increases [12].
Prior to the study, utilizing inclusion criteria, nurses at the institution identified patients suitable for inclusion in the study. The patient list created. The patients were randomly selected from the list and the intervention and control groups were determined by the researcher. The 30 patients included in the study were simple randomly method divided into two groups by the investigator: 15 patients in the intervention group and 15 patients in the control group. The investigator met with the study group before the application and provided information about the methods and purpose of the study.
The “Descriptive Characteristics Data Form” and “Assessment Scale of Adaptation Difficulty for the Elderly” were administered to both groups through face-to-face interviews. Due to the change in consciousness in Alzheimer's patients, assistance was received when filling out the scales from the nurse and health personnel who were working in the institution. Prior to the music session, participants in the intervention group received detailed information regarding its purpose. The computer and sound system were provided by the researcher. The music sessions implemented for 12 weeks in total and there were twice per week (Mondays and Wednesdays), and each music session lasted 50 minutes. The patients in the intervention group were taken to another sitting room in the institution for the music sessions. Patients in the control group received standard care but did not participate in the specific intervention. During the sessions, changes in emotional status were observed in patients, and no negative reactions were encountered. A week after the music session completed, the “Assessment Scale of Adaptation Difficulty for the Elderly” was re-administered to both groups (Figure 1).
Consultancy and support was obtained from the Alzheimer's specialist neurologist in conducting the study.
Data was analyzed using the SPSS statistical package program. In addition to descriptive statistical methods (frequency, percentage, mean, standard deviation) to evaluate the study data, the Shapiro Wilks test was used to examine the normal distribution. Mann Whitney U test was used for between-group comparisons of parameters, and Wilcoxon Friedman test was used for within-group comparisons. Results with p-values less than 0.05 were considered statistically significant.
Of the total, 53.8% of the patients in the intervention group were women. A total of 73.3% were primary school graduates, and 20.0% were middle school graduates. A total of 93.3% of the patients were single, 86.7% had children, and the mean age was 81.67 ± 6.78 years. In the control group, 73.3% of the patients were women. A total of 46.7% were primary school graduates, and 33.3% were middle school graduates. A total of 86.7% of the patients were single, all had children, and the mean age was 78.73 ± 12.23 years. There were no significant differencesin the socio-demographic characteristics (gender, educational status,marital status, children, age) of the patients between the experiment and control groups, and the demographic characteristics of both groups were similar (p > 0.05).
A total of 80.0% of the patients in the intervention group had chronic diseases other than Alzheimer’s disease. Approximately 73.3% of the patients had been diagnosed with Alzheimer’s for the past 3-9 years, and the mean period of stay in the elderly care center was 28.73 ± 23.40 months. A total of 60.0% of the patients in the control group had chronic diseases other than Alzheimer’s disease. Approximately 86.7% of the patients had been diagnosed with Alzheimer’s for 10-17 years, and the mean period of stay in the elderly care center was 28.00 ± 14.10 months. There were no statistically substantial divergence between the groups in terms of chronic disease and the period of stay in the elderly care center (p>0.05), and the characteristics of both groups were similar. However, there was a statistically significant difference in the time of diagnosis between the intervention and control groups (p=0.03).
The mean pre-test score of the intervention group for ASADE was 1.43 ± 0.44 and the mean pre-test score of the control group was 1.51 ± 0.58. There were no statistically substantial divergence in mean ASADE pre-test scores between the intervention and control groups (p=0.838). While the mean post-test score of the intervention group was 0.66 ± 0.24, the mean post-test score of the control group was 1.29 ± 0.59. There was a statistically substantial divergence in mean ASADE post-test scores between the intervention and control groups (p=0.001). There was a significant difference between the mean ASADE pre-test and post-test scores of the intervention and control groups (p< 0.05). When ASADE scores of both groups were examined, it was observed that the decrease in the mean scores of the intervention group was more significant compared to the mean scores of the control group (Table 1).
Role and self-actualization mode:In the intervention group, the mean pre-test and post-test scores of the Role and Self-Actualization mode sub-dimension were 1.97 ± 0.41 and 1.24 ± 0.37, respectively. As for the control group, the mean pre-test and post-test scores were 2.04 ± 0.48 and 1.83 ± 0.52, respectively. There was a substantial divergence between the mean pre-test and post-test scores of both the intervention and control groups (p< 0.05).
For the Role and Self-Actualization mode sub-dimension of ASADE, the mean pre-test score was 1.97 ± 0.41 in the intervention group and 2.04 ± 0.48 in the control group. There was no substantial divergence between the two groups in terms of ASADE Role and Self-actualization sub-dimension pre-test scores (p=0.806). Interestingly, the mean post-test score for the Role and Self-actualization mode sub-dimension was 1.24 ± 0.37 in the intervention group and 1.83 ± 0.52 in the control group. There was also a substantial divergence in ASADE Role and Self-actualization sub-dimension post-test scores between the groups (p=0.004) (Table 2).
Interdependence mode:In the intervention group, the mean pre-test and post-test scores of the interdependence mode sub-dimension of ASADE were 1.32 ± 0.64 and 0.29 ± 0.30, respectively. There was a substantial divergence between the pre-test and post-test scores of the intervention group. As for the control group, the mean pre-test and post-test scores were 0.98 ± 0.78 and 0.83 ± 0.62, respectively. There was no substantial divergence between the interdependence mode pre-test and post-test scores of the control group (p=0.243).
For the interdependence mode sub-dimension of ASADE, the mean pre-test score was 1.32 ± 0.64 in the intervention group and 0.98 ± 0.78 in the control group. There was no substantial divergence in the ASADE interdependence mode sub-dimension pre-test scores (p=0.187) between the intervention and control groups. On the other hand, the mean post-test score for the interdependence mode sub-dimension was 0.29 ± 0.30 in the intervention group and 0.83 ± 0.62 in the control group. There was a substantial divergence in ASADE interdependence sub-dimension post-test scores between the two groups (p=0.013) (Table 2).
Physiological status mode:In the intervention group, the mean pre-test and post-test scores of the physiological status sub-dimension of ASADE were 1.03 ± 0.51 and 0.48 ± 0.44, respectively. As for the control group, the mean pre-test and post-test scores were 1.55 ± 0.83 and 1.07 ± 0.89. There was a substantial divergence between the mean pre-test and post-test scores in either of the two groups (p< 0.05).
For the physiological status sub-dimension of ASADE, the mean pre-test score was 1.03 ± 0.51 in the intervention group and 1.55 ± 0.83 in the control group. There was no substantial divergence in ASADE physiological status sub-dimension pre-test scores between the groups (p=0.061). The mean post-test score for the physiological status sub-dimension was 0.48 ± 0.44 in the intervention group and 1.07 ± 0.89 in the control group. There was a substantial divergence in ASADE physiological status sub-dimension post-test scores between the groups (p=0.045) (Table 2).
Self-concept mode:In the intervention group, the mean pre-test and post-test scores of the self-concept sub-dimension of ASADE were 0.80 ± 0.58 and 0.17 ± 0.22, respectively. There was a substantial divergence between the pre-test and post-test scores in the intervention group (p=0001). As for the control group, the mean pre-test and post-test scores were 1.22 ± 0.68 and 1.10 ± 1.08. There was no substantial divergence between the pre-test and post-test scores in the control groups (P = 0.357)
For the self-concept sub-dimension of ASADE, the mean pre-test score was 0.80 ± 0.58 in the intervention group and 1.22 ± 0.68 in the control group. There was no substantial divergence in ASADE self-concept sub-dimension pre-test scores between the intervention and control groups (p=0.081). The mean post-test score for the self-concept sub-dimension was 0.17 ± 0.22 in the intervention group and 1.10 ± 1.08 in the control group. There was a substantial divergence in the ASADE self-concept sub- -dimension post-test scores between the groups (p=0.003).
While there were no statistically substantial divergence between the mean pre-test scores of the intervention and control group in ASADE sub-dimensions, there was a substantial divergence between the mean post-test scores of the groups in all ASADE sub-dimensions (p< 0.05) (Table 2).
In the intervention group, there was a significant difference in gender, presence of chronic diseases and age over 75 between role and self-actualization mode and the interdependence sub-dimension scores (p< 0.05). There was a significant difference in physiological status sub-dimension scores with respect to gender, presence of chronic diseases, and ages between 75-84 (p< 0.05). Additionally, there wasa significant difference in self-concept sub-dimension scores with respect to gender, presence of chronic diseases, and age (75-84 and >=85) (p< 0.05).
The result of the present study indicates decrease in adaptation difficulty in both the intervention and control groups. The decrease in the mean scores of the intervention group was more significant compared to that of the control group. The decrease in adaptation difficulty in both groups suggest that there may be a possibility of an intervention for the patients other than the present application or an external factor resulting in a decrease of adaptation difficulty. The control group's interactions with other patients throughout the day, the television programs they watched and their communication with visiting relatives may have positively impacted their mental state and motivation. It is thought that mental recovery and increase motivation may increase adaptation. Additionally, improved sleep quality and duration within the control group could have decreasing their adaptation difficulty. However, it was not possible to evaluate the influence of these external factors during the research period. The decrease in adaptation difficulty was more pronounced in the intervention group compared to that of the control group, indicating that the music played to the intervention group had a positive effect on decreasing patients’ adaptation difficulty. This result is consistent with other studies mentioned in the literature. Garcia-Navarro et al. as a result of their systematic review study, they reported that the stress, anxiety and depression levels of patients receiving music therapy decreased [14]. In study by Tang et al. standard care was provided for the control groupand music was played for the intervention group in addition to being given standard care. Based on the results of the study, improvement in behavioral problems such as apathy were observed in patients from the intervention group [15]. Feng et al. determined that in the music therapy they applied to 121 Alzheimer's patients, there was a decrease in the depression and anxiety symptoms of the patients [16]. Lyu et al. conducted a study on 298 Alzheimer’s patients. The participants were divided into a lyric reading, a singing and a control group. It was expressed that there was a significant improvement in enhancing mental function and wellbeing in the patients in the intervention group [7].
The results of this study highlighted a significant decrease in ASADE sub-dimension mean scores asobserved in the intervention group. This indicated that music may have induced a positive effect on decreasing patients’adaptation difficulty in the intervention group. In the control group, there was a significant decrease in the role and self-actualization mode and physiologicalstatussub-dimensions. This was attributed to the occasional fluctuations in psychological and physiological status for the different stages of Alzheimer’s disease [17]. The results also suggested that patients in the intervention and control groups may have been exposed to a possible other application during the study period that was out of the study’s control.
In the present study, there was a significant difference in the interdependence sub-dimension scores of the intervention group compared to those of the control group. Positive communication between individuals, establishing friendships, and being able to solve the problems they experience in society are discussed in the interdependence sub-dimension. One of the main factors that increase adaptation in Alzheimer’s patients is establishing effective communication. In this context, eliminating the factors that will prevent communication with the patient is of vital importance. In particular, anxiety and concerns of the patient should be addressed and an environment of trust should be established [18]. The present study was carried out in an environment where the patients felt safe and were familiar with the conditions within the institution. This provided an environment of positive communication with other people during the music session. In addition, the soothing and calming effect of music on the patients enabled them to communicate positively within their environment. This may explain the significant difference in the interdependence sub-dimension in the intervention group.
In the present study, a significant improvement was observed in the self-concept sub-dimension scores of the patients in the intervention group. The concept of self is defined as how an individual evaluates themselves while considering all the features that exist within them. The positive or negative emotions that an individual attributes to this concept reveals self-esteem. Self- -esteem is also defined as a person’s overall sense of self-worthor personal value. Individuals with high self-esteem generally feel that they are accepted and deemed important by society and are of useto the society in which they live. Individuals with low self-esteem may see themselves as worthless and inadequate [19]. Yılmaz, investigated the relationship between depression and self-esteem in 33 elderly individuals aged 60 and over who were living in a nursing home and found symptoms of depression in 75% of the participants. The author concluded that as the level of depression in the elderly increased, the level of self-esteem decreased [20]. It can be argued that the significant reduce in the self-concept sub-dimension of the intervention group was the result of the positive effects of music on psychological symptoms such as depression.
The results of study indicated that the mean scores of ASADE sub-dimensions were statistically significant in both female and male patients in the intervention group. This indicates that the music played to patients positively affects adaptation difficulty in both genders. These results suggest that gender is not a factor that changes the effectiveness of music. These results are consistent with other studies in the literature. İşıkcı et al. in a study conducted with 60 undergo colonoscopy of patients (30 men and 30 women), it was determined that gender did not change the effect of music [21]. There are currently no studies in the literature demonstrating that gender and age are factors that change the effect of music on Alzheimer’s patients.
In the present study, the mean age of patients in the intervention group was 81.67 years. This is similar to other studies conducted with patients who had Alzheimer’s disease. Moreno-Morales et al. in a meta-analysis evaluating the effects of music in patients with Alzheimer type dementia, it was determined that the patients included in the studies is between 75-90 years old [22]. In the present study, the rate of patients in the intervention group with chronic diseases was high. This is attributed to the increased prevalence of chronic diseases at old age [23]. The most common chronic diseases in old age include heart diseases, hypertension and diabetes [24]. This is consistent with the literature as the most common chronic diseases in patients of the intervention group were hypertension and diabetes in the present study. Chronic diseases adversely affect the day-to-day lives of the elderly, decrease their quality of life, and increase the burden of care. Elderly people who do not perform day-to-day activities in their daily lives feel inadequate, and may result in the emergence of psychological problems. Depression is the most common health problem in individuals affected with chronic diseases [25]. The significant difference observed in the ASADE mean scores of the patients in the intervention group with chronic diseases suggests that the psychological symptoms associated with chronic diseases may have decreased with the effect of music.
The study's findings revealed that the Nihavent theme had a positive effect on decreasing the adaptation difficulty of patients with Alzheimer’s disease. Adaptation difficulty decreased in all ASADE sub-dimensions in the intervention group. Interestingly, a decrease in adaptation difficulty was observed in role and self-actualization mode and physiological status sub-dimensions in the control group
In light of the findings, to optimize nursing care for Alzheimer's patients, pre-assessments of their adaptation levels are crucial. Integrating music sessions featuring Nihavent theme into care plans holds therapeutic promise. Health institutions should empower nurses by providing resources and training for organizing such sessions. Further research with larger samples is essential to solidify the efficacy of the Nihavent theme. Additionally, comparative studies investigating the impact of both verbal and non-verbal music on Alzheimer's patients should also be.
Alzheimer's Elderly Care Center is one of the limited number of centers in the province. Different studies and applications can be carried out in this center. In order not to affect the results of the research, it was emphasized throughout our study that the sample group did not make any application to the nursing home management and employees other than routine applications. In addition, help was received from the nurses and care staff working in the institution to verify the answers given by the patients to some questions in the scales used.
This research project was granted ethical approval by the “X” Clinical Research Ethics Committee Presidency on the12th of April 2018. Institutional approval was obtained from the an Alzheimer Elderly Care Center in Eskisehir-Turkey, on January 17th 2018.
All participants in the study provided their written agreement to participate after being fully informed.
No potential conflicts were identified by the authors.
This research was conducted without external funding

![]()

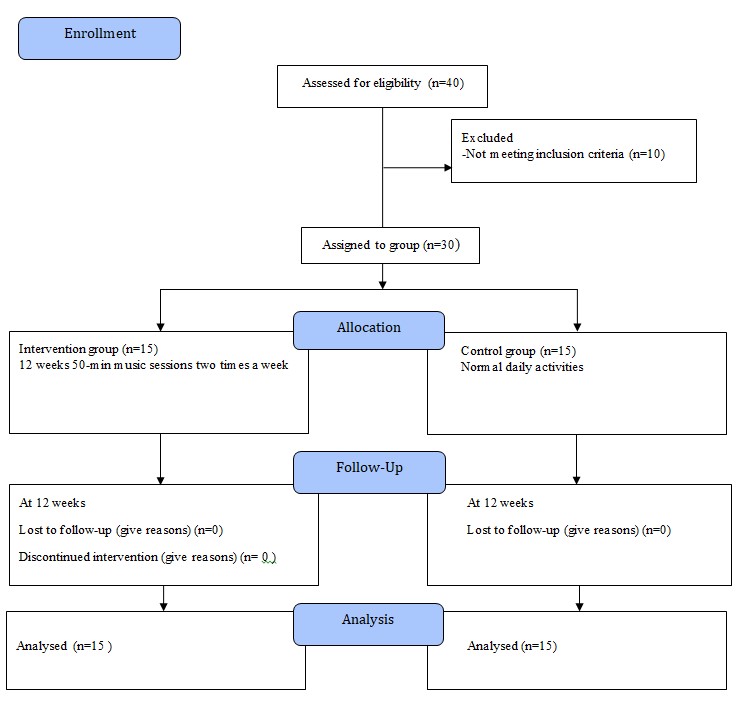 |
| Figure 1: Research flow chart |
|
Mean ± Standard DeviationMedian (Q1 – Q3) |
* |
||
Pre-Test |
Post-Test |
|||
Study group |
Intervention (n=15) |
1.43±0.44 1.29 (1.17 - |
0.66±0.24 0.67 (0.58 - |
0.001 |
Control (n=15) |
1.51±0.58 1.50 (1.04 - |
1.29±0.59 1.25 (0.88 - |
0.008 |
|
p*(intergroup) |
0.838 |
0.001 |
|
|
ASADE Sub-dimensions |
Mean± Standard DeviationMedian (Q1 – Q3) |
p* (between follow-ups) |
||
Pre-Test |
Post-Test |
|||
Role and Self- Actualization Mode |
Intervention (n=15) |
1.97 ± 0.411.89 (1.78 |
1.24 ± 0.371.33 (1.11 |
0.001 |
Control (n=15) |
2.04 ± 0.482.00 (1.67 |
1.83 ± 0.521.89 (1.33 |
0.042 |
|
p* (intergroup) |
0.806 |
0.004 |
|
|
Interdependence Mode |
Intervention (n=15) |
1.32 ± 0.641.14 (0.86 |
0.29 ± 0.300.14 (0.00 |
0.001 |
Control (n=15) |
0.98 ± 0.780.86 (0.00 |
0.83 ± 0.620.57 (0.29 |
0.243 |
|
p* (intergroup) |
0.187 |
0.013 |
|
|
PhysiologicalMode |
Intervention (n=15) |
1.03 ± 0.511.00 (0.50 |
0.48 ± 0.440.25 (0.25 |
0.001 |
Control (n=15) |
1.55 ± 0.831.50 (1.00 |
1.07 ± 0.890.75 (0.50 |
0.003 |
|
p* (intergroup) |
0.061 |
0.045 |
|
|
Self-concept Mode |
Intervention (n=15) |
0.80 ± 0.580.75 (0.25 |
0.17 ± 0.220.00 (0.00 |
0.001 |
Control (n=15) |
1.22 ± 0.681.00 (0.75 |
1.10 ± 1.080.50 (0.25 |
0.357 |
|
p* (intergroup) |
0.081 |
0.003 |
|
|




































