Open Access
Research Article
Max Screen
ISSN: 2767-9292
Copyright: © 2021 Brantmeier C. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Self-assessment (SA) of English speaking ability by patients has been an important reference for the health workforce, and in the past 10 years, research examining health literacy in the USA has continued to emphasize the patient. In the current study, 338 Health Care Workers (HCWs) (82% female and 63% nurses) reported on their current communications with patients (one year into the COVID-19 pandemic) and recalled what communication was like at the onset of the pandemic. Through SA as a way for HCWs to analyze communication, this study investigated information available from community and healthcare facilities, oral communication with patients, and the training of healthcare professionals. Results indicated a significant difference between perceptions when comparing current reports (one year into the pandemic) with concurrent recall of conditions at the beginning of the pandemic time (p < .001); however, the majority disagreed that health information access was sufficient even at the later point. Respondents indicated a significant improvement on the following metrics: feeling prepared to discuss knowledge of COVID-19 with language diverse patients and feeling that patients understood what individual words meant in the context of discussing COVID-19. A majority of HCWs had received training on communication and were interested in further training.
Keywords: Language Diverse Patients; Nursing Education; Communication; Training; Self-Assessment
Much attention has been given to the health disparities foregrounded and exacerbated by the COVID-19 pandemic. Race, ethnicity, and socioeconomic status have all been implicated as driving forces of differing health outcomes. Health literacy, or an individual’s capacity to acquire and use new health information [1] is an additional strong predictor of health status [2]. AbdelLatif [3] recently cited [4] Paasche-Orlow’s 2005 report that 26% of all people living in the USA have low general health literacy. Prior to COVID-19, many postulated that language is one of the most significant, and yet underexplored, social determinants of health, and one which deserves increased attention in our medical system [5,6].
Language diverse patients, especially those who speak a language other than English at home, are a growing percentage of the USA population [7]. Numerous studies have shown that these individuals are at a higher risk for low health literacy compared to patients who primarily speak English [8,9]. As such, language diverse patients are at higher risk of poor health outcomes [9] and, unsurprisingly, have been disproportionately impacted by the COVD-19 pandemic [10-12]. Recently, Nyashanu et al [13] examined the challenges faced by frontline workers in health and social care during the COVID-19 pandemic and concluded that there was a lack of pandemic preparedness in terms of challenges enforcing social distancing, shortage of PPE and more, that lead to anxiety and fear. The present study adds to this research by illuminating related challenges about preparedness through an examination of HCWs, perceptions of communication about COVID-19 with language diverse patients.
Prior studies of health literacy have focused on the ability of individual patients to understand health-related information presented to them [1,8,14,15]. This emphasis on patients’ health literacy, however, does not sufficiently emphasize the role and responsibility of health systems in communication. The present study attempts to shift the focus away from the patient’s language ability by examining HCW’s perceptions and self-assessments of communication. The way in which information is presented, in both oral and written form, substantially influences what patients are able to learn and understand. Moving forward, our focus should include the responsibility of the health system to effectively communicate with all patients [9,14].
The COVID-19 pandemic offers an interesting lens through which to analyze healthcare communication not only because of the disparities that it continues to highlight, but also because of the rapid evolution and time-sensitive dissemination of healthcare information that it has required. At the beginning of the COVID-19 pandemic, health policies and information changed at unprecedented rates. Our study was designed to shed further light into the ability of the healthcare system to appropriately communicate with patients, and specifically to compare this communication at two time points: what HCWs recalled about the onset, and one year into, the COVID-19 pandemic.
To date, it appears that no study has examined the perceptions and self-assessment (SA) of HCWs’ communication with language diverse patients. In this interdisciplinary study, we attempt to offer a new dimension to prior work on the intersection of language and health communication. For the purposes of this study, a language minority patient is a patient who uses a language other than English as their dominant language in their home.
Data taken from the Migration Policy Institute’s State Immigration Data Profiles reveals that in Missouri, in 2019, the total foreign-born population was 259,650 people, with 34.5% indicating that they speak English less than “very well.” Of the total U.S. born population in Missouri, 0.6% indicated that they speak English less than “very well.”
There are approximately 2.8 million people living in the St. Louis metro area. In 2017-2018, the area had approximately 5,640 foreign-born people (immigrants, refugees and foreign students) [16]. The most recent figures reported by the International Institute of St. Louis, the leading refugee resettlement agency, indicate that refugees arriving to the St. Louis region represented 15 different languages in 2019 and 14 different languages in 2020. Recent demographic data from Missouri Department of Elementary and Secondary Education (DESE) 2020 indicates an enrollment of 10,352 students who were identified as Limited English Proficiency (LEP) for the St. Louis metro area, which includes the city of St. Louis.
Comparing current reports (one year into the pandemic) with concurrent recall of conditions that existed at the beginning of the pandemic, our study addresses four main research questions:
1) How do health care workers rate the COVID-19 resources for language diverse patients provided by the community and their healthcare facilities (posters, billboards, etc.)?
2) How do health care workers assess their own preparedness to communicate about COVID-19 with all patients? How do they asses their actual oral interactions with language diverse patients/clients when discussing COVID-19?
3) How do health care workers assess the specific strategies or techniques they used to facilitate discussions about COVID-19 to language diverse patients?
4) Are healthcare providers interested in continued training on communication tools and strategies for interactions with language diverse patients/clients?
After a review of the literature on health literacy across the disciplines of medicine and applied linguistics, a tailored, theory-based SA instrument was developed to examine the perceptions of HCWs about communication with language diverse patients at the onset of, and one year into, the COVID-19 pandemic. The preliminary survey was piloted with 15 HCWs to assess for the total amount of time spent to complete the survey and to provide feedback on any ambiguities or clarifications with survey items. Ultimately, the survey was condensed to 72 questions. It took approximately 10-12 minutes to complete. We used 5-point Likert response scales for all questions in order to encourage precision in rating and approach consistency with equal intervals. The survey was initially sent out without offer of compensation, and three weeks after dissemination, a $10 gift card incentive was added to increase participation. The questions were categorized as follows: Demographics, Information Available for Language Minorities, Oral Communication with All Patients, Communication with Language Minority Groups, Reading and Writing with Language Minorities, and Training for Healthcare Professionals. Demographic questions included self-reported age, gender, race, ethnicity, medical profession, division affiliation, healthcare facility affiliation, use of languages other than English at and outside of work, experience working abroad, and information about the provider’s patient population.
The survey was prefaced by a letter briefly explaining the study, the length and online nature of the survey, and the following definitions: 1) for the purposes of this study, the term ‘language minority’ refers to those who use a language other than English as the dominant language in their home, and 2) “a health care worker is one who delivers care and services to the sick and ailing either directly as doctors and nurses or indirectly as aides, helpers and laboratory technicians” [17]. Participants were also informed that participation was optional, and that all responses would be anonymous and analyzed in an aggregated form for research purposes in order to inform the development of training modules and procedures that account for differences in communication with language minorities. A copy of the survey is available from the lead author upon request. The Washington University in St. Louis Institutional Review Board approved this study, #202102133.
We recruited participants via email outreach to division heads, department chairs, unit supervisors, and other healthcare leaders at seven different hospitals, clinics and healthcare facilities in the St. Louis region. Each email briefly explained the study and requested approval to distribute an online survey to health care workers in their respective division, unit, or program. These healthcare leaders sent the survey out electronically to potential respondents during a period of 6 weeks, (February 22nd, 2021, to April 5th, 2021), approximately one year after the onset of the COVID-19 pandemic.
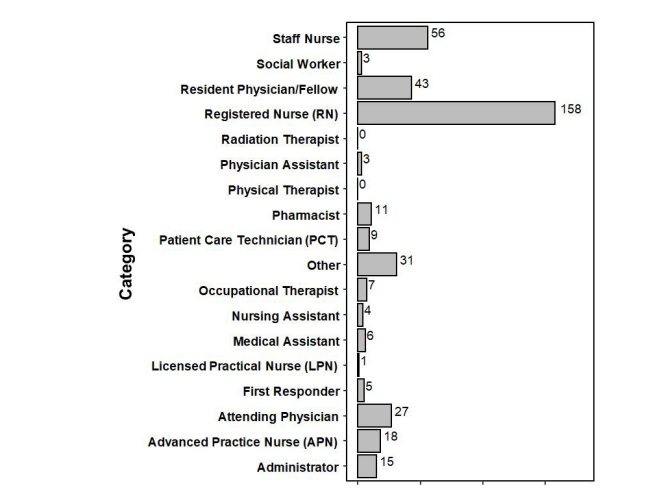
A total of 576 healthcare workers ages 18 – 75 or older from the St. Louis region responded to the online survey. Respondents that had more than 20% missing survey data or spent less than three seconds per question on average were removed from the final data set. Ultimately, 338 respondents were used for final data analysis. Participants were asked to indicate their profession and division/unit (multi-select from list). The largest responding groups consisted of nurses: registered nurses (158) and staff nurses (56). Regarding discipline/department or division, the largest group responding came from pediatrics (127). Respondents were also asked to self-report other demographic factors, such as race and ethnicity. The largest group by race was White Caucasian, followed by Asian and then Black/African American. A total of 13 respondents were Hispanic/Latino. Graph One shows the sample group by profession.
The data were analyzed using R Version 4.0.5 (R Core Team 2021). The survey items relevant for the first three research questions asked respondents to consider their current communications with patients and also to recall what was true about those communications when the pandemic began. Accordingly, these data were examined using a repeated measure analysis of variance (ANOVA). Because a large sample size will produce statistical significance for trivial differences, we also report Cohen’s d effect sizes. These are standardized mean differences; Cohen (1988) suggests the following descriptive thresholds for magnitude of d: small (d = 0.2), medium (d = 0.5), and large (d = 0.8) (see Table 1 for the survey question groupings, as well as the means, standard deviations, Cohen’s d and p-value of the ANOVAs for each research question). See Table 1 for ANOVA results for survey question groupings.
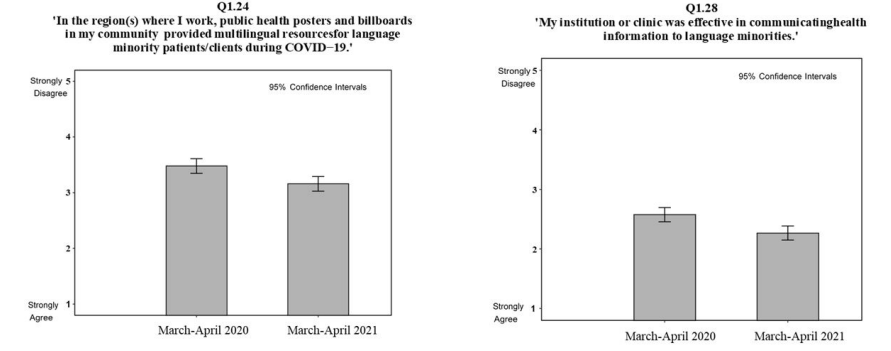
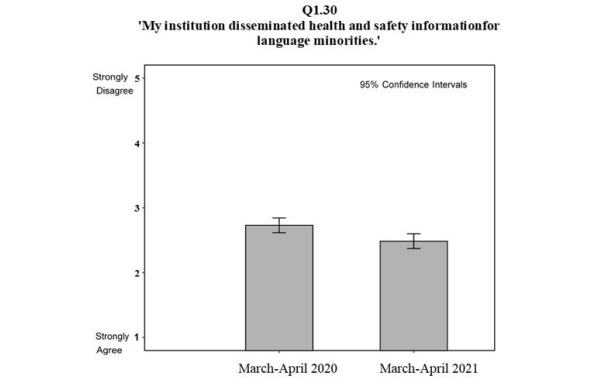
To assess COVID-19 resources for language diverse clients and patients, health care workers rated resources provided by the community and their healthcare facility (survey questions 1.21 – 1.30). Overall, findings revealed a significant difference by time (onset and one year later) for communication provided by the community and healthcare facilities. More specifically, respondents felt access to information about the pandemic, including on a public health and institution/clinic level, was significantly better one year after the onset of the pandemic (p < .001). Figure 1 illustrates specific items within this overall theme. For the question about public messages including sufficient information for language minority individuals, respondents reported feeling neutral and one year later somewhat agree, and this same trend is seen for the item about the community billboards. Respondents also felt that communication at the institutional and healthcare facility level improved over time, and these ratings were actually more favorable than those at the community level. Notably, even one year into the pandemic, the majority of healthcare workers disagreed or strongly disagreed that health information access was sufficient.
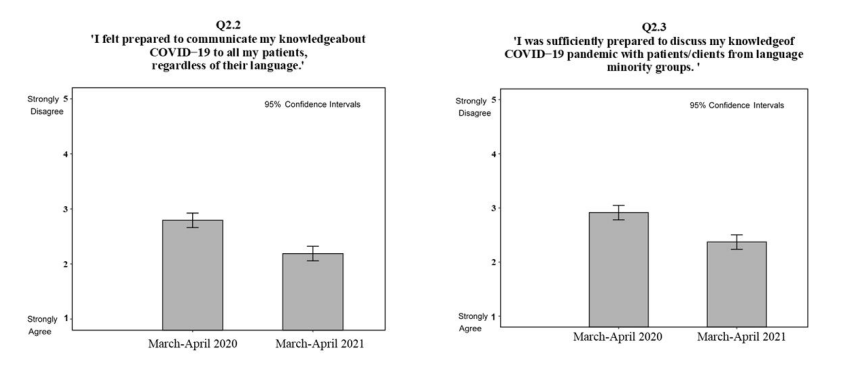
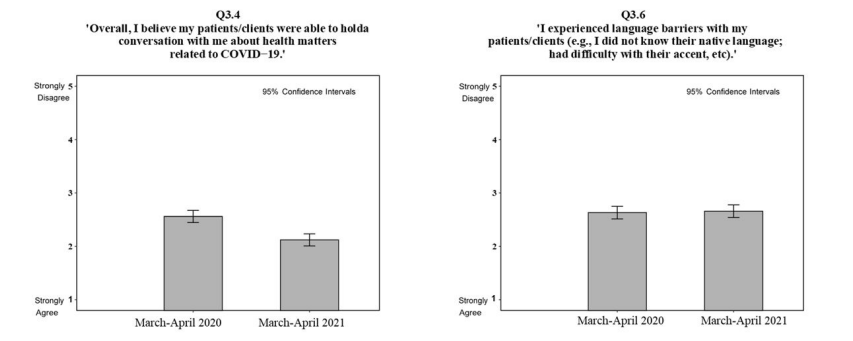
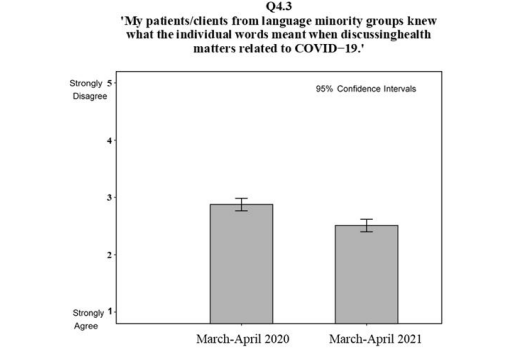
Figures 2 and 3 show that respondents did not agree or strongly agree that they felt prepared to communicate knowledge about COVID-19 to all patients (survey questions 2.2, 2.3, 3.2 – 3.6, 4.2 – 4.8). Rather, at the onset they felt neutral and then one year later felt somewhat better, but once again, respondents never indicated that they strongly agreed that they were prepared to communicate. Respondents did indicate a significant improvement in feeling prepared to discuss their knowledge of COVID-19, specifically, with their language diverse patients/clients, and in feeling that their patients understood what individual words meant in the context of discussing COVID-19 (survey questions 4.9 – 4.13). It is important to note that respondents felt that language/ communication barriers did not change significantly from the onset of the pandemic to one year later; at both times points, they indicated neutrality or agreement regarding experiencing language barriers with patients (see item 3.6 below).
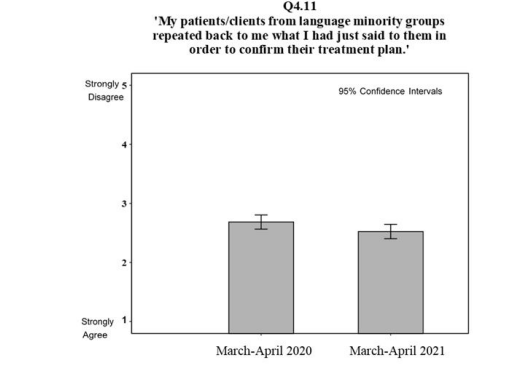
While findings revealed that specific strategies and techniques to discuss COVID-19 with language diverse patients improved over time, findings reveal that healthcare workers did not give high ratings at either time point for the item “patients from language diverse groups asked questions for clarification” (Figure 3, survey question 4.8). Results also indicated that healthcare workers did not agree that patients repeated back to confirm understanding of both diagnosis and treatment plans (Figure 3, survey questions 4.10 and 4.11). More specifically, while the reported use of a ‘teach-back’ technique was significantly higher one year into the pandemic, the magnitude of the change was small, with only a minority of healthcare workers giving high ratings for asking patients and clients from language diverse groups to repeat back their treatment plan to confirm understanding (Figure 3, survey questions 4.10 and 4.11). Encouragingly, a majority of providers did report agreement with someone being available to assist with language interpreting in instances of communication breakdown at both time points, and this measure improved from the beginning of the pandemic to one year later (Table 1, survey question 4.13).
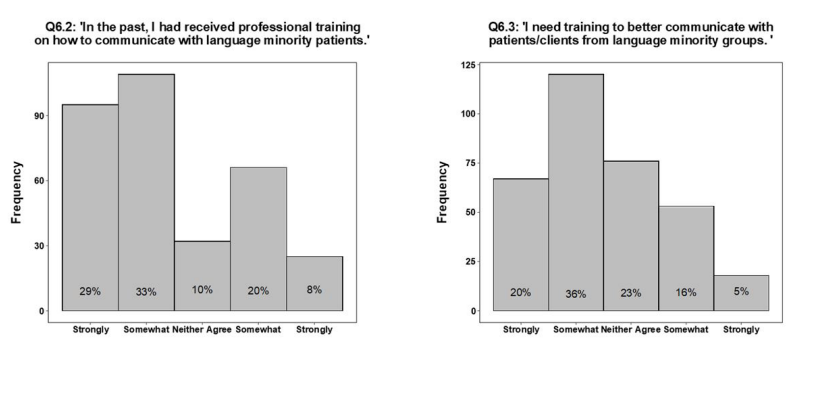
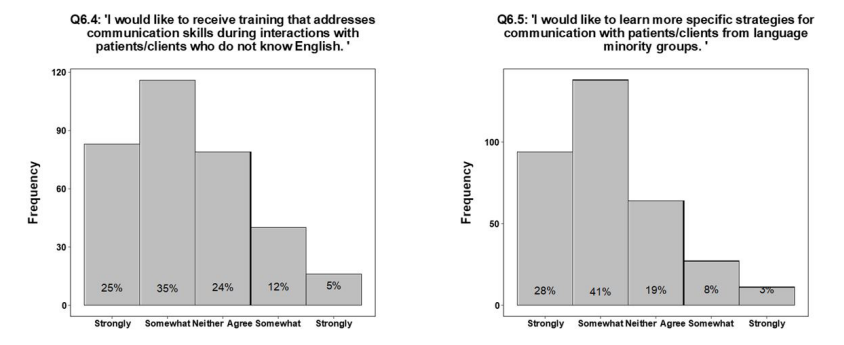
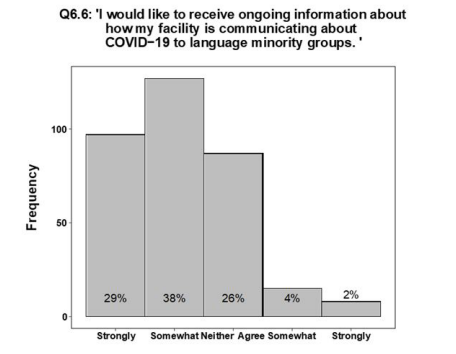
As indicated in Figure 4, survey question 6.2, 62% of the respondents agreed or strongly agreed that they had received training in the past on how to communicate with language minority patients, and on the question (Figure 4, survey question 6.5) 69% of the respondents indicated that they would like to learn more specific strategies for communication with language minority groups. More specifically, as revealed in Table 1, HCWs felt most strongly about learning specific strategies for communication with language diverse patients (M = 2.17, SD = 1.03) and receiving ongoing information about how facilities are communicating about COVID-19 to language diverse groups of patients (M = 2.13, SD = 0.97), although they were also favorable toward receiving professional training on how to communicate with language minority patients (M = 2.44, SD = 1.30), receiving training to better communicate with patients/clients from language minority groups (M = 2.51, SD = 1.14) and receiving training that addresses communication skills during interactions with patients/clients who do not know English (M = 2.37, SD = 1.12).
Health literacy has long focused on the patient’s capacity to understand information. Equally important, however, is the effectiveness of health institutions and healthcare providers in conveying information in an accurate and accessible way that takes into account the needs of individuals from various backgrounds, including those who prefer or only speak a language other than English. Identifying individuals with communication needs does not necessarily improve communication and health outcomes, as a patient’s health literacy may vary depending on the medical problems, the healthcare providers, and the system providing the care [1]. This issue has been foregrounded by the rapidly changing information landscape of the COVID-19 pandemic. Overall, the present study demonstrates that in the St. Louis region, HCWs perceived improved communication with language diverse patients one year into the COVID-19 pandemic as compared to the onset. While perceived improvement over time is crucial, it is important to highlight that the actual level of perceived communication with language diverse patients is not given high ratings. Additionally, a key finding from this study is that most HCWs indicate that the community and their facilities were indeed aware of the needs of COVID-19 resources for language minorities and provided an increasing amount of communication resources over time. Respondents also indicated positive and responsive leadership/initiatives to ensure equal healthcare access during a public health crisis in the St. Louis area. The dissemination of health messages between the community and patients as well as between healthcare facilities and patients has been critical during COVID-19, especially because the alternative strategies for communicating health information suggested by prior researchers [1,18] included discussion groups, informal information meetings, and lectures - all in-person strategies that were not feasible during COVID-19. Modifying and simplifying the language of health information as well as identifying reliable sources is critical; and consequently, the national-level COVID-19 Health Literacy Project was launched to support patients by providing fact sheets and materials in multiple languages with easy-tounderstand details for everyone across the USA.
Findings also indicate that HCWs felt more confident about their preparedness to communicate with patients as time progressed during the pandemic. To attend to communication concerns nationwide, Lancet provided a COVID-19 resource center that included up-to-date information to support HCWs [19]. Results of the survey items in the present study that specifically address the SA of actual oral interactions with patients during COVID-19, including e-health meetings, show increased ratings compared to what was recalled to have been true at the beginning of the pandemic. However, respondents indicated neutrality or agreement with experiencing language barriers with patients. The corresponding implications for this finding are that HCWs’ methodology for oral communication should include modifications to their immediate oral interactions and strategies to improve quality. It is encouraging to see that HCWs reported an increase of ratings for items that addressed patients asking questions for clarification one year after the onset of the pandemic. However, it should be noted that the magnitude of increase was not large. This finding blends with prior work by Chen et al [8] who found that Chinese patients were not likely to questions their doctors’ or nurses’ advice. In order for language diverse patients to be actively involved in making healthcare choices while navigating the complex healthcare system, it is imperative for patients to ask questions about diagnosis, treatment plan, and more; and it is also crucial that HCWs have the ability to recognize language and communication challenges with patients and to adapt communication approaches and healthcare plans accordingly.
In the present study, while HCWs generally indicated favorable communication with language diverse individuals, the majority (69%) also indicated that they would be interested in learning more specific strategies for communication with language diverse patients. Interestingly, this was true even of those who reported that they had received professional training in the past. Healthcare workers do not feel prepared (Q3.6) and are interested in additional trainings (Q6.3-6.6). These data indicate the need and demand among healthcare workers to receive communication trainings. This training will need to be multifaceted, as healthcare communication involves multiple modalities. It should include instruction regarding written materials in multiple languages and in-person or remote interpretation. Training should include strategies on how to effectively collaborate with medical interpreters (both in-person and phone-based or video-based). Multiple simulations and curricula have been developed for medical students and residents [20-26] as well as dental providers [27] to teach interpreter best practices. However, this training is not yet present in all medical schools or residencies, and is not always provided in the context of an interdisciplinary team. Prior studies have outlined the benefits of Interprofessional Education as a means to improve the quality of care [28], and the present study highlights the need to include communication and language as part of the interdisciplinary efforts. Additionally, findings of the present study underscore the need to offer this type of education to providers who are no longer in training. A direction for future research should include an analysis of the standards of accreditation and practice for health professionals, similar to the recent work by Bogossian & Craven [28], in order to examine whether or not current trainings include strategies and best practices for communications with linguistically diverse patients. Another related area of recent interest has been ensuring that bilingual providers who choose to speak a language other than English with patients are undergoing appropriate certification prior to doing so [29,30]. This is particularly important given the increase in medical Spanish being taught in medical schools in the USA.
In the present study, the majority of survey respondents were nurses. Singleton et al [31] noted that the nursing literature offers little assistance in integrating language and cultural considerations into nursing efforts, and the present study underscores that nurses want additional training. Nurses and all HCWs can learn how to adapt communication approaches, such as modifying language and soliciting additional information, as well as facilitating immediate comprehension checks. This may seem daunting, as HCWs already are over-burdened and often under-resourced; however, if the institution recognizes the issues with communication and encourages teams of HCWs to form partnerships with existing experts on language acquisition and use, this training could be collaborative and informative. It is also important to note that communication with children differs from adults, and therefore nurses from the specialty pediatrics may have very different experiences and needs that could be addressed in training.
The present study emphasizes the need for medical professionals to learn about self-assessment in perceived competency and to develop communication strategies and tools accordingly. Given the findings of the current study, a future investigation could examine the existing knowledge that HCWs have about the theory and research on language acquisition and use and how to attend to immediate language needs so that corresponding implications for training modules are developed and include principled strategies about how to modify oral output so that it is immediately more comprehensible to the patient. Examining the perspectives of healthcare workers about communication with language minorities is merely the start. Future research should go beyond this study and investigate the perception of both patients and clients about actual communication. A future study may want to ask both healthcare workers and patients to complete a follow-up questionnaire immediately following a visit so that their perceptions of the same communication can be compared. A criterion-referenced SA instrument could be developed and utilized so that HCWs know how to self-diagnose their own strengths and weaknesses in actual situations. A survey of HCW and patient perceptions would report important information that could also be used as the foundation for a mixed-methods study that would include interviews with healthcare workers to further explore perceptions, create curricula for HCWs to improve care, and inform e-health services.
An important limitation of the present study is that respondents were asked to recall perceptions from one year ago, which may lead to memory bias. Additionally, the survey required HCWs to collapse all language diverse patients into one category. A future study may be needed to look at the differences within and between language groups, as some languages, such as Spanish, have sound-to-letter correspondence with English, while other languages, such as Chinese, do not. Careful examinations of differences by language group may yield corresponding implications for practice. Finally, although the present study did reveal an increase in perceptions of communication quality with language diverse patients during COVID-19, it remains unclear whether the resources and communications were accessible, beneficial, and sufficiently timely. A future study could examine these specific details [32-46].
Certain groups in the USA are at higher risk for having limited English language abilities, such as individuals who do not speak English at home. Language diversity is a commonly overlooked component of diversity, and should be emphasized as an aspect of initiatives aimed at decreasing bias and discrimination in healthcare going forward. One goal of the present study is to promote self-reflection amongst health care workers on the role of communication with patients from language diverse groups. Another goal is to inspire future research and practice changes during this global public health emergency and beyond. We end with a quote often utilized in the literature on health literacy: “The problem with communication is the illusion that it has occurred” (George Bernard Shaw).

![]()

 |
   |
| Figure 2: RQ1 |
   |
| Figure 3: RQ2 |
  |
| Figure 4: RQ3 |
   |
| Figure 5: RQ4 |
Question Groupings |
Survey Questions |
Mean (SD) |
Mean (SD) |
Cohen’s D |
P-value |
Information Available for Language Minorities |
1.21 'In the region(s) where I work, language minorities had sufficient access to information |
3.21 (1.17) |
2.48 (1.01) |
0.67 |
<0.001 |
|
1.22 'In the region(s) where my patients/clients come from, language minority groups were able to obtain up−to−date and real−time information about the constantly changing situation of |
3.23 (1.15) |
2.57 (1.03) |
0.60 |
<0.001 |
|
1.23 'In the region(s) where I work, public health messages about COVID−19 included sufficient information so that patients/clients from language minority groups could understand |
3.23 (1.22) |
2.72 (1.16) |
0.43 |
<0.001 |
|
1.24 'In the region(s) where I work, public health posters and billboards in my community provided multilingual resources for language |
3.48 (1.24) |
3.16 (1.23) |
0.26 |
<0.001 |
|
1.26 'Language interpretation service hotlines were available for my patients/clients in my |
2.51 (1.14) |
2.23 (1.05) |
0.20 |
<0.001 |
|
1.27 'My institution or clinic had a plan to communicate health information to language |
2.51 (1.18) |
2.21 (1.10) |
0.26 |
<0.001 |
|
1.28 'My institution or clinic was effective in communicating health information to language |
2.58 (1.16) |
2.27 (1.05) |
0.28 |
<0.001 |
|
1.29 'My institution or clinic had resources or staff on hand to help me communicate with |
2.13 (1.15) |
1.99 (1.06) |
0.13 |
<0.001 |
|
1.30 'My institution disseminated health and safety information for language minorities.' |
2.73 (1.09) |
2.49 (1.03) |
0.23 |
<0.001 |
Oral Comm with All |
2.2 'I felt prepared to communicate my |
2.79 (1.33) |
2.19 (1.12) |
0.49 |
<0.001 |
|
2.3 'I was sufficiently prepared to discuss my knowledge of COVID−19 pandemic with |
2.91 (1.30) |
2.37 (1.18) |
0.44 |
<0.001 |
|
3.2 'I believe that my patients/clients had the ability to orally communicate with me about |
2.38 (1.14) |
2.06 (0.97) |
0.30 |
<0.001 |
|
3.3 'Overall, I believe that my patients/clients knew what the individual words meant when |
2.79 (1.19) |
2.31 (0.98) |
0.44 |
<0.001 |
|
3.4 'Overall, I believe my patients/clients were able to hold a conversation with me about health |
2.56 (1.15) |
2.12 (0.95) |
0.42 |
<0.001 |
|
3.5 'My institution had screening questions that were used to identify individuals who were likely |
2.62 (1.24) |
2.41 (1.20) |
0.17 |
<0.001 |
|
3.6 'I experienced language barriers with my patients/clients (e.g., I did not know their native language; had difficulty with their accent, etc).' |
2.63 (1.10) |
2.66 (1.10) |
-0.02 |
0.19 |
|
4.2 'My patients/clients from language minority groups seemed satisfied with our discussions |
2.70 (0.96) |
2.47 (0.93) |
0.25 |
<0.001 |
|
4.3 'My patients/clients from language minority groups knew what the individual words meant when discussing health matters related to |
2.87 (1.04) |
2.51 (0.96) |
0.37 |
<0.001 |
|
4.4 'My patients/clients from language minority groups were able to hold a conversation with me about health matters related to COVID−19.' |
2.80 (1.11) |
2.44 (0.98) |
0.35 |
<0.001 |
|
4.5 'I felt prepared to communicate about necessary PPE with individuals from language |
2.55 (1.16) |
2.15 (1.03) |
0.37 |
<0.001 |
|
4.6 'I felt prepared to communicate about social distancing with individuals from language |
2.48 (1.18) |
2.08 (1.01) |
0.36 |
<0.001 |
|
4.7 'I felt prepared to communicate about contact tracing with individuals from language minority groups.' |
3.03 (1.22) |
2.66 (1.20) |
0.32 |
<0.001 |
|
4.8 'My patients/clients from language minority groups asked me questions about COVID−19 |
2.60 (1.13) |
2.50 (1.11) |
0.10 |
0.003 |
Communication with Language Minority |
4.9 'If a patient/client from a language minority group did not understand me, I was able to modify my language so that they understood |
2.50 (1.11) |
2.36 (1.06) |
0.12 |
<0.001 |
|
4.10 'My patients/clients from language minority groups repeated back to me what I had just said to them in order to confirm their understanding |
2.74 (1.08) |
2.58 (1.02) |
0.15 |
<0.001 |
|
4.11 'My patients/clients from language minority groups repeated back to me what I had just said |
2.68 (1.08) |
2.51 (1.03) |
0.15 |
<0.001 |
|
4.12 'My patients/clients from language minority groups were able to give me all the information I needed to know.' |
2.78 (1.10) |
2.59 (1.04) |
0.18 |
<0.001 |
|
4.13 'During the visit, when my patients/ clients from language minority groups did not understand or when there was a breakdown in |
2.24 (1.05) |
2.12 (0.99) |
0.11 |
<0.001 |




































