Open Access
Research Article
Max Screen >>
ISSN: 2393-9060
Copyright: © 2018 Volp ACP. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Interferon gamma (IFN-γ) is associated with the inflammatory responses modulation, which could culminate in chronic metabolic diseases. In this context, the aim of the present study was to evaluate the effect of the acai (Euterpe oleracea Mart. mart.) pulp consumption on the anthropometric, clinical and biochemical parameters in women clinically healthy, with IFN-γ, respectively, smaller and higher than 5 pg/mL. Twenty four women in G1 (with IFN-γ concentrations smaller than 5 pg/mL) and sixteen in G2 (with IFN-γ concentrations greater than 5 pg / mL), consumed 200g per day of acai pulp during four weeks. Anthropometric and body composition measurements, biochemical and clinical data were evaluated before and after the intervention. After the intervention, there were significant reductions in diastolic blood pressure (p=0.035) and in plasma leptin concentrations (p=0.006) of G2 volunteers, while G1 volunteers did not present significant changes in these parameters. The acai pulp consumption during four weeks did not change metabolic homeostasis in the volunteers with IFN-γ smaller than 5 pg/mL and promotes a potential protective effect to metabolic diseases in that with IFN-γ higher than 5 pg/mL.
Keywords:Subclinical Inflammation; Acai; Interferon Gamma; Flavonoids; Inflammatory Mediators
List of abbreviationsInflammation; Acai; Interferon Gamma; Flavonoids; Inflammatory Mediators3) List of abbreviantions: % BF: Body Fat Percentage; BMI: Body Mass Index; COX-1: Cyclooxygenase 1; COX-2: Cyclooxygenase 2; FFQ: Food Frequency Questionnaire; HDL: High Density Lipoprotein; HOMA-IR index: Homeostasis Model of Insulin Resistance; IFN-γ: interferon gamma; IL-18: Interleukin 18; JAK: Janus Kinases; LDL-c: Low Density Lipoprotein; NK: Natural Killer; PASW: Predictive Analytics SoftWare; PCR: C-Reactive Protein; STAT: Signal Transduction and Transcription Activation; TNF: Tumor Necrosis Factor Interleukin 15 (IL-15); WC: Waist Circumference
Acai (Euterpe oleracea Mart.), the fruit of the acai palm tree, native to Amazon (Brazil), is considered typical and popular in this region [1]. In recent years, it has gained popularity due to health benefits provided by its phytochemical composition, especially by the bioactive elements presence, such as: polyphenolic compounds, flavonoids and anthocyanins [2].
The beneficial effects of polyphenols and their subclasses on the health have been demonstrated with antioxidant and anti-inflammatory effects exerted by these compounds, with a consequent role in the prevention of the inflammatory metabolic diseases. They favor the regression of oxidative stress mediators and inflammatory mediators, such as: C-reactive protein (CRP),tumor necrosis factor (TNF), interleukin 15 (IL-15) and interleukin 18 (IL-18), resulting in the modulation of the subclinical inflammation [3-18].
IFN-γ (interferon gamma), proinflammatory cytokine and primary product of T and natural killer (NK) cells, is related to the generation of the inflammatory responses and, for this reason, is considered the master regulator of the systemic subclinical inflammation, since it is associated to the development of metabolic diseases (i.e: type 2 diabetes, atherosclerosis and obesity [19].
In this way, IFN-γ higher concentrations in plasma relate to body weight gain, adiposity excess, hyperglycemia and atherosclerosis [1]. Studies show that higher IFN-γ concentrations is associated with obesity in humans and rodents and that T cells from adipose tissue of obese rats, after in vitro stimulation also produced higher IFN-γ amount compared with that extracted from lean animals [20,21,26]. On the other hand, the suppression of this mediator promotes the inverse effect in animals. It favors the body weight reduction, associated with the decrease of food intake, due to leptin modulation and insulin sensitivity improvement [21].
In this perspective, IFN-γ, as a subclinical inflammation marker, has a crucial role on the metabolic diseases. So, if it used in clinical practice in order to measure the subclinical inflammation degree, could contribute to metabolic changes prediction, which could result in low-grade systemic inflammation, with consequent development of metabolic diseases [27].
Therefore, find the ways to inhibit subclinical inflammation and its associated metabolic changes is essential. Studies in vivo and in vitro have shown the positive effect of acai (Euterpe oleracea Mart.) on the inflammatory chain, since it inhibits a production of reactive oxygen species, besides to inhibiting the activity of cyclooxygenase 1 and 2(COX-1 and COX-2), TNF and NF-kB [28,29]. In humans, the consumption of 100g of acai pulp for 30 days in overweight patients reduced total cholesterol, low density lipoprotein (LDL-c), glycaemia and insulin, showing efficient on the reduction of metabolic syndrome risk factors [30].
Thus, we evaluated the effects of daily acai consumption on the anthropometric, body composition, clinical and biochemical parameters during four weeks in women clinically healthy with IFN-γ concentrations smaller than 5 pg/mL (G1), considered in inflammatory homeostasis and women with IFN-γ concentrations greater than 5 pg / mL (G2) in plasma.
This study consisted of a self-controlled nutritional intervention, whose inclusion criteria were healthy women aged between 18 and 35 years-old, with body mass index (BMI) between 18,5 and 29,9 kg/m2. The exclusion criteria were illiteracy, changes higher than 10% in body weight two months before starting the study, allergies or eating disorders, restrictive dietary pattern (i.e.: vegetarian diet, Atkins diet), use of nutritional supplements or chronic medication (except contraceptives), be elite athletes, present acute inflammatory, infectious or chronic diseases, be pregnant, lactating or smoker.
One hundred and twenty five women were assessed for eligibility, of these 42 fulfilling the inclusion criteria and 40 completing the study (Figure 1). Each participant signed the consent form in duplicate. The study was approved by the Human Research Ethics Committee of the Federal University of Ouro Preto (UFOP), Minas Gerais, Brazil (CAAE 0062.0.238.000-10).
The clinical trial, randomized, consisted of stratifying the participants into two groups, according to IFN-γ in plasma concentrations: IFN-γ <5 pg/mL (G1) and IFN-γ > 5 pg/mL (G2). Such stratification was based on that used by Calder et al., which shows that, usually, there is no normal range of inflammatory mediators concentrations, but there is a general range considered normal that can be clinically used [27].
Subsequently, the volunteers daily consumed 200 grams of acai pulp for four consecutive weeks in a free-living situation. The participants were oriented to maintain their lifestyle, including their usual diet throughout the experiment (Figure 2).
This study was based on three stages: selection and preparation of the individuals; the beginning of intervention and the end of the nutritional intervention.
In the first meeting, participants were instructed about the trial period and were submitted to: fasted blood samples collection; blood pressure and anthropometric measurements and Food Frequency Questionnaire (FFQ) application. At the end of 4 weeks, anthropometric and blood pressure data, fasting blood sample and FFQ were collected again.
The previously validated food consumption frequency questionnaire containing 86 food items was applied before and after the experimental period in order to verify the food intake standard of the participants’ usual diet [31]. The dietary nutrients intake was calculated by Avanutri & Nutrição software (Tres Rios, Brasil).
The body weight was measured using a Welmy® digital scale (W200-A model). The BMI was calculated as recommended by the World Health Organization [32].
The body composition was represented by the body fat percentage (% BF), determined by horizontal tetrapolar electric bioimpedance (Biodynamics, model 310e) [33,34]. The waist circumference (WC) was measured by Frisancho methodology [32,33].
Systolic and diastolic blood pressure was measured in triplicate obeying a 5 minutes-interval between measurements by Omron® pressure apparatus (HEM-705CP model). Fasting blood samples collection were performed before and after nutritional intervention by venous puncture of the antecubital region using a vacuum system. Glucose, insulin, total cholesterol and fractions and triacylglycerols were evaluated by colorimetric enzymatic method (Metrolab® spectrophotometer, 2800 model) (Figure 3). LDL-c concentrations were calculated according to Friedewald equation [35]. It was used Ultrasensitive Insulin test (Acess® Immunoassay System) to evaluate fasting insulin, determined by chemiluminescent immunoassay. To determine insulin sensitivity, it was used the Homeostasis Model of Insulin Resistance (HOMA-IR index) [36].
IFN-γ, TNF, CRP and leptin were determined by enzymatic immunoassay using specific commercial kits (MILLIPLEX® MAP; Millipore Corporation, Billerica, MA, EUA) with sensitivity of 0,03 IU/mL to IFN-γ, 0,1 pg/mL to leptin, 118 ρg/mL to TNF and 0,27 μg/mL to CPC.
The data distribution normality was tested by the Kolmogorov-Smirnov test and presented as mean ± standard deviation for those parametric variables and as median and interquartile range for the non-parametric variables. In addition, all variables were compared by the paired t-student test and Wilcoxon paired test to analyze the effect of the intervention. The comparisons between the means and basal medians of the groups were made by the t-Student (parametric) and U-Mann-Whitney (non-parametric) tests. For all statistical tests, it was adopted P <0.05 is considered significant. For data analysis was used the Predictive Analytics SoftWare (PASW) Statistics software.
The study included 40 volunteers, 24 belonging to G1 and 16 to G2, with mean age of 22.8 years ± 3.2 and 25.1 years ± 2.8, respectively. Table 1 shows the anthropometric, body composition, clinical, biochemical and inflammatory characteristics at baseline and after intervention as a function of IFN-γ in plasma concentrations.
In the baseline state, there were differences between groups for high density lipoprotein (HDL) and TNF. HDL was higher in G1 than G2, and TNF was reduced in G1 when compared to G2, whereas the other parameters did not differ between groups.
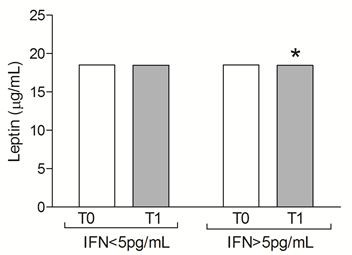
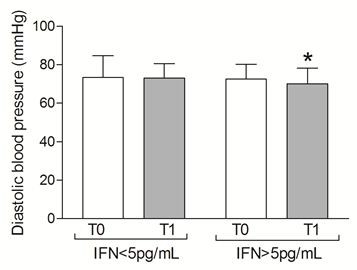
After nutritional intervention with acai pulp, G2 group presented reduction in leptin concentration, as well as decreased the diastolic blood pressure, while G1 did not present changes remaining in metabolic homeostasis.
After consumption of acai, there was no difference in the intake of calories, proteins, lipids, cholesterol, carbohydrates, fibers, linoleic acid, linolenic acid, oleic acid and ratio ω-3: ω-6 (data not shown; p>0,05).There was also no change in the total antioxidant capacity of the diet. As volunteers were instructed to maintain their eating habits throughout the study, possibly the acai pulp was included in place of other foods, such as fruits and juices rich in other flavonoids, carotenoids, and other compounds or pigments with bioactive properties that also have high antioxidant power, thus not altering the dietary nor the total antioxidant capacity of the diet.
In order to verify the effect of acai pulp consumption regarding a specific inflammatory biomarker in clinically healthy women, it was carried out a nutritional intervention to evaluate the anthropometric, clinical and biochemical changes in women with IFN-γ greater and less than 5 pg/mL. Our results showed that the daily consumption of 200g of acai pulp for 30 days promoted beneficial alterations in the biochemical parameters of inflamed women with IFN-γ concentrations higher than 5 pg/mL since there was a significant reduction in diastolic blood pressure and leptin concentrations. The effect of acai pulp consumption on G1 volunteers contributed to the maintenance of their metabolic homeostasis Such result was expected, since interventions with fruits rich in flavonoids are strongly associated with the modulation of inflammatory markers concentrations , as well as on the maintaining of anthropometric parameters, such as body weight, waist circumference, waist-hip ratio, body composition and reduction of biochemical parameters including total cholesterol, LDL, triacylglycerol, blood glucose, blood pressure and insulin [8-10,12,15,16,18,30,37-46]. Thus, in the present study, the acai pulp could be contributed for maintaining the metabolic homeostasis, with consequent prevention of metabolic changes. Literature shows associations between food patterns rich in anthocyanins with the prevention of chronic diseases, such as: diabetes type 2, hypertension, cardiovascular diseases and obesity [47-49].
It was observed that diastolic blood pressure and leptin concentration were smaller in G2 after the intervention with acai pulp. In fact, studies showed that high IFN-γ concentrations can modulate the angiotensinogen production and sodium reabsorption, promoting hypertension in dose-dependent way, by Janus Kinases (JAK) pathways activation and signal transduction and transcription activation (STAT) [50]. In this context, the hypertension prevention in patients with high IFN-γ concentrations is favorable. Studies show beneficial results of nutritional interventions with fruits rich in flavonoids on the blood pressure modulation. As Igwe et al. analyzed the effect the consumption of juice from an anthocyanin-rich Japanese plum variety (Queen Garnet plum, QGP) in 12 adults older (65+ years) and 12 adults younger (18-45 years) that resulted a significant reduction in BP and cardiovascular responses was observed in both age groups which was more obvious in the older age group on the single dose for systolic BP, diastolic BP, mean arterial pressure, and heart rate [46]. As in Novotny et al. study, in which the intervention with cranberry juice resulted in diastolic blood pressure reduction in control subjects 12 [12]. Additionally, daily doses of the same juice (500 mL/4 weeks) resulted in 3 mmHg reduction in systolic blood pressure in men metabolically healthy (comparing with baseline) [51]. Basu et al. observed that blueberry consumption (50 g freeze-dried blueberries, approximately 350 g fresh blueberries) reduced systolic and diastolic blood pressures about 6% e 4%, respectively, in individuals with metabolic syndrome [52]. In healthy individuals or with some cardiovascular risk factor, Erlund et al. pointed that supplementation with blueberries reduce systolic and diastolic blood pressures [53]. These results corroborate animal’s studies, as Mykkanen et al. study, in which rats fed with wild blueberries and high fat diet presented 10% of reduction in the systolic blood pressure compared with that received only high fat diet. In the same study, it was find positive correlation between IFN-γ concentrations and blood pressure [54].
The hypertension pathophysiological mechanism is multifactorial and includes oxidative stress, inflammation renin-angiotensin hyperactivation [55,56]. A possible mechanism of blood pressure control regarding the flavonoid-rich fruit interventions may be associated with the reduction of the angiotensin converting enzyme, as suggested in works using pomegranate juice in humans and and in in vitro study with polyphenols [57,58].
On the other hand, studies have shown that interventions with fruits rich in flavonoids had no effect on blood pressure in humans, such as the intervention with bluebarries in obese men and women with insulin resistance did not modify their blood pressure both in the placebo and blueberries groups [18,39,40,44,59].
In the subclinical inflammatory process context, reducing leptin concentration is satisfactory, since there are evidences of positive correlation between leptin and IFN-γ. Leptin can stimulate NK cells to express cytokines, inducing the inflammation amplification [60,61]. In mononuclear cells of 20 healty individuals (7 females and 13 males), intracelular IFN-γ expression was significantly elevated after leptin administration [61]. So, the effect of acai pulp consumption reflect positively on the reduction of leptin concentration in G2, favoring the metabolic homeostasis and contribuiting to prevent future complications. Corroborating our results, studies observed that leptin concentrations were reduced in animals submitted to anthocyanins intervention during 12 weeks [62]. Sweet cherries-purified anthocyanins inhibitted the leptin release in male rats fed with high fat diet [63]. In vitro, the effect of freeze-dried cranberries on H2O2-inflamed mature adipocytes significantly reduced the leptin expression and release [64].
Other possible mechanism of acai pulp protection is associated with its cellular protection properties. Since acai is rich in anthocyanins, which is a class of flavonoids derived from polyphenols; according to Navarrete et al. the polyphenols action on celular protection derived from transcription fator inhibiton, such as STAT and NF-kB with consequent modulation of the pro-inflammatory cytokines [7,11,25,49]. This possibly reflect on the blood pressure and leptin concentration modulations, as well as in clinical, biochemical and anthropometric parameters making feasible the metabolic homeostasis, as seen in G1, also developing protective effect to chronic diseases [65-67].
The acai pulp consumption during 4 weeks exerted a modulator effect on diastolic blood pressure and leptin concentration in women clinically healthy with IFN-γ plasm concentration higher than 5 pg/mL, reflecting its beneficial metabolic effect. Additionally, this intervention did not promote any metabolic change in volunteers with IFN-γ plasm concentration smaller than 5 pg/mL, predisposing to the metabolic homeostasis in them. These results provide new insights for a better understanding about the effects of acai pulp consumption in humans in a subclinical inflammation context, serving as a base to future studies.
The authors are grateful to all the volunteers who participated of this study, to Federal University of Ouro Preto (UFOP), to Coordenação de Aperfeiçoamento do Ensino Superior do Ministério da Educação do Brasil (CAPES), to Conselho Nacional de Pesquisa e Desenvolvimento Científico (CNPq) and to Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) for financial support.
Coordenação de Aperfeiçoamento do Ensino Superior do Ministério da Educação do Brasil (CAPES), Conselho Nacional de Pesquisa e Desenvolvimento Científico e Tecnológico (CNPq) and Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) for the financial support, by means of following grants: CDS-APQ-04495-10 (Edital Programa Primeiros Projetos- 15/2010) e 475417/2013-5 (Edital Universal -14/2013), which enable this work.
SFG: conducted the fieldwork, data collection, laboratory processing of samples, statistical analysis, wrote and edited the manuscript; TFC: data collection, laboratory processing of samples, statistical analysis and edited the manuscript; FLPO: guided the statistical analysis and edited the manuscript; FCS; JFA; RNF: guided the fieldwork, managed the laboratory processing and edited the manuscript; ACPV: project leader, general coordinator, held financial management, designed the study, supervised the fieldwork, managed the laboratory processing and edited the manuscript. All authors read and approved the final manuscript.

![]()

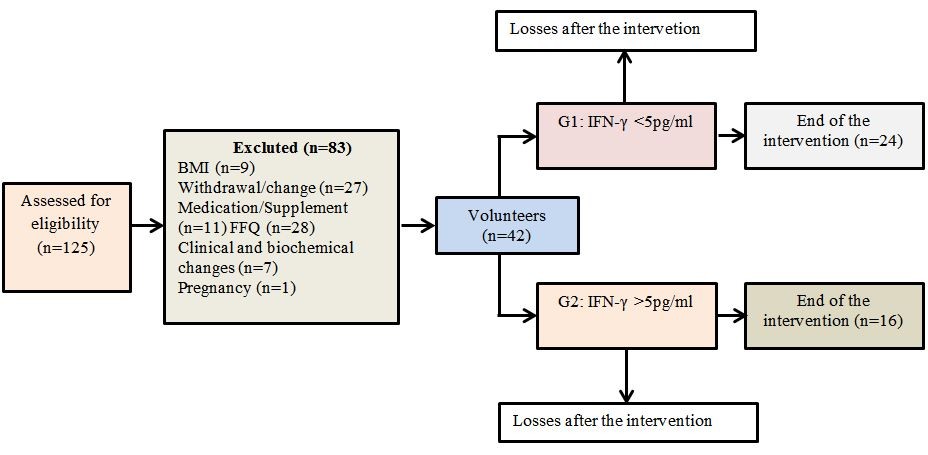 |
| Figure 1:Flow diagram of volunteers |
 |
| IFN, Interferon gamma; T0: Baseline characteristics (before the intervention). T1: Final characteristics (after the intervention). Data are presented as mean and standard deviation, and were analyzed with Normality test: Kolmogorov- Smirnov, p<0.05 and paired t-Student. *p=0.035. |
 |
| IFN, Interferon gamma; T0: Baseline characteristics (before the intervention). T1: Final characteristics (after the intervention). Data presented as mean and standard deviation, and were analyzed with Normality test: Kolmogorov- Smirnov, p<0.05 and paired t-Student. *p=0.006 |
|
|
IFN<5pg/mL (n=24) |
IFN>5pg/mL (n=16) |
||||||||||
Variable |
T0 |
T1 |
p*a |
T0 |
T1 |
p*a |
p*b |
||||||
Anthropometric and body composition parameters |
|||||||||||||
Body weight, Kg |
68.65±14.58 |
69.2(57.3-87.5) |
0.144 |
62.7±11.85 |
59.5(51.5-70.8) |
0.613 |
0.199 |
||||||
BMI, Kg/m2 |
25.05(20.85-29.0) |
25.44(21.9-31.2) |
0.310 |
21.8(20.9-27.5) |
21.9(20.5-26.4) |
0.825 |
0.590 |
||||||
Waist circumference, cm |
76.72±10.23 |
79.3±10.7 |
0.116 |
73.6±5.96 |
72.9±6.5 |
0.258 |
0.235 |
||||||
Truncal fat, % |
54.83±5.08 |
55.5±5.97 |
0.193 |
52.7±6.07 |
55.4±4.65 |
0.472 |
0.256 |
||||||
Body fat (BIA), % |
32.5±5.06 |
35.54±4.97 |
0.08 |
30.6±5.53 |
30.3±4.2 |
0.396 |
0.279 |
||||||
Clinical parameters |
|||||||||||||
Systolic blood pres- sure, mmHg |
106.1±12.6 |
106.3±10.6 |
0.09 |
105.1±12.1 |
100.8±12.1 |
0.248 |
0.808 |
||||||
Diastolic blood pres- sure, mmHg |
73.3±11.3 |
73.01±7.6 |
0.424 |
72.5±7.7 |
70.12±8.06 |
0.035 |
0.803 |
||||||
Biochemical parameters and inflammatory mediators |
|||||||||||||
Glucose, mg/dL |
79.12(75-81.5) |
79.8±7.26 |
0.879 |
78.5(75-85.3) |
79.7±5.7 |
0.671 |
0.579 |
||||||
Insulin, μIU/mL |
6.6±2.3 |
6.84±2.91 |
0.229 |
5.76±2.03 |
5.9±2.2 |
0.954 |
0.214 |
||||||
HOMA-IR |
1.4±0.5 |
1.47(0.8-1.6) |
0.318 |
1.17±0.54 |
1.08±0.5 |
0.551 |
0.308 |
||||||
Cholesterol, mg/dL |
192.6±34.3 |
185.70±22.2 |
0.498 |
182.2±33.9 |
187.5±39.3 |
0.176 |
0.353 |
||||||
Triacylglycerol, mg/dL |
75.5(60.2-102.5) |
96.53±35.3 |
0.225 |
68(39.5-96.5) |
73.1±33.3 |
0.684 |
0.241 |
||||||
LDL, mg/dL |
106.2±29.9 |
97.6±31.6 |
0.263 |
107.6±32.5 |
109.9±34.9 |
0.645 |
0.891 |
||||||
HDL, mg/dL |
69.2±12.4 |
72.4±13.3 |
0.942 |
60.1±13.7 |
63.04±13.4 |
0.203 |
0.04 |
||||||
TNF, pg/mL |
5.45±1.87 |
5.31±2.1 |
0.545 |
7.35±3.03 |
7.86±2.7 |
0.951 |
0.03 |
||||||
CRP, μg/mL |
20.39±12.23 |
21.1±13.2 |
0.702 |
11.5±10.6 |
10.6±7.7 |
0.805 |
0.01 |
||||||
Leptin, μg/mL |
18.517±0.0005 |
18.498±0.0005 |
0.340 |
18.505±0.0003 |
18.471±0.0003 |
0.006 |
0.383 |
||||||
T0: Basline characteristics (before the intervention); T1: Final characteristics (after the intervention); BMI: Body Mass Index; BIA: Electrical Bioimpedance; HOMAIR: Homeostatic Model of Iinsulin Resistance; LDL: LDL cholesterol; HDL: HDL cholesterol; TNF: Tumoral Necrosis Factor; CRP: c-Reactive Protein. Data presented as mean � standard deviation or median (Q1-Q3) according parimetry.Normality test: Kolmogorov- Smirnov, p<0.05 |
|||||||||||||




































