Open Access
Research Article
Max Screen
ISSN: 2393-9060
Copyright: © 2024 Rossana G Iannitti. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Gestational diabetes mellitus (GDM) is associated with an increased maternal and fetal risk of complications. Other than lifestyle modifications and diet, little prevention can be done towards this maternal complication. Through a preclinical approach and a retrospective clinical trial, we investigated the effects of maternal supplementation with a nutraceutical composition based on resveratrol (RSV) and alpha-lipoic acid (ALA) on insulin resistance and GDM status. The combination of RSV with ALA displayed a synergistic action to reduce sterol regulatory element-binding protein 1 (SREBP-1) in human epatic cell line HEPG2. The retrospective clinical analysis, showed that the treatment lead to a lower insulin necessity (15.0% vs, 37.5%, p =0.02), a lower daily insulin requirement (11 ± 2 UI vs. 14 ± 3 UI, p < 0.0001), and lower fasting glucose level in pregnant women with GDM. The results also show lower neonatal complications and lead to no associated risk of adverse effects. The mechanistic sinergy of RSV with ALA on AMP- Activated Kinase (AMPK) and SIRT via sterol regulatory element-binding transcription factor 1 (SREBF1) could be the key to its benefical effects shown and may offer important benefits for the prevention of high risk maternal and fetal complications such as GDM and preclampsia.
Keywords: Gestational diabetes mellitus, maternal BMI, resveratrol, alpha-lipoic acid
List of Abbreviations:ACC-2: acetyl-CoA carboxylase 2; ALA: alpha-lipoic acid; AMPK: AMP-Activated Kinase; BCS: Biopharmaceutical Classification System; BMI: Body Mass Index; GDM: Gestational Diabete Mellitus; GLUT-4: Glucose transporter type 4; HAPO: Hyperglycemia and Adverse Pregnancy Outcome; IR: Insulin Resistance; IUGR: intra-uterine growth restriction; MO: maternal obesity; OGTT: Oral Glucose Tolerance Test; RSV: Resveratrol; SD: Standard Deviation; SREBF1:sterol regulatory element-binding transcription factor 1; SREBP-1: sterol regulatory element-binding protein 1.
Gestational Diabetes Mellitus (GDM) is defined as “glucose intolerance with onset or first recognition during pregnancy” [1]. Approximately 10% of all pregnancies are complicated by GDM, which includes hyperglycemia, insulin resistance (IR), and fetal anomalies. GDM is usually detected using an oral glucose tolerance test (OGTT) between 24 to 28 weeks of gestation, but guidelines and the diagnostic criteria vary among countries and between major societies worldwide [2], making estimates of prevalence difficult.
GDM is highly associated with obesity. Obesity is a growing major public health problem worldwide. In 2016, the estimated age-standardized prevalence of obesity and overweight among adult women of the European Region was 24.5% and 54.3%, respectively [3]. This prevalence is expected to continue rising in the next years [4]. Overweight (body mass index (BMI) 25.0-29.9 kg/m2 ) or obesity (BMI ≥30.0 kg/m2 ) are the most important modifiable risk factors for GDM. Indeed, the risk of developing GDM is up to 5-fold higher in morbidly obese women, when compared to women with normal body weight [5].
Due to the severe complications it causes to both mother and fetus, GDM is a serious problem worldwide. GDM has potentially serious short- and long-term consequences as demonstrated by Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study [6]. GDM is associated with various adverse maternal, fetal, and perinatal outcomes, including preeclampsia, preterm delivery, cesarean section delivery, fetal macrosomia, neonatal hypoglycemia, and Neonatal Intensive Care Unit admission. All these complications can be reduced by early diagnosis and treatment of GDM. HAPO study demonstrated a correlation between early pregnancy fasting glucose levels and earlier onset of GDM.
RSV (trans- 3,5,4′-trihydroxystilbene), a naturally occurring polyphenolic compound, is able to improve GDM indicators. Indeed, RSV was found to be useful in improving glucose metabolism and insulin tolerance, regulating blood lipids [7,8] and plasma adipokines, and modulating embryonic oxidative stress and apoptosis [9,10]. In particular, from a mechanistic point of view, RSV decreases glucose absorption in the gut by suppressing alpha-amylase activity and reducing the functionality of the Na+ /glucose cotransporter in small intestine epithelial cells [11].
Moreover, RSV promotes glycogen formation in the liver, through AMP-activated protein kinase (AMPK) pathway, playing a critical role in maintaining glucose balance, by promoting glucose transport through the translocation of Glucose transporter type 4 (GLUT4) to the plasma membrane in an insulin-independent manner [11]. Besides, RSV has been found to boost insulin secretion in pancreatic β-cells through SIRT1 activation [12,13] and to improve insulin sensitivity by promoting muscle and fat cells glucose uptake. Additionally, RSV strengthens insulin signal receptiveness in skeletal muscle by promoting GLUT4 membrane insertion via SIRT1, AMPK, and AKT activation, thereby preventing elevated blood sugar levels and enhancing insulin resistance management [14,15]. Furthermore, RSV can ameliorate the GDM complications by reducing oxidative stress, the effects on placentation, and the adverse effects on embryonic development [9]. In the same way, ALA was widely used for this indication, considered as a safe and effective adjunctive antidiabetic agent with insulin sensitizing activity. From a mechanistic point of view, ALA modulates the expression of AMPK in the hypothalamus and peripheral tissues. Noteworthy, AMPK activation in skeletal muscle improves insulin sensitivity by increasing glucose uptake and fatty acid oxidation, as already mentioned for RSV [16]. Is worthy of note that AMPK is also pharmaceutical target of well- known oral hypoglycaemic agents such as metformin and peroxisome proliferator-activated receptors (PPAR) gamma agonists.
RSV can display benificial effects in human health, the action however may depend on the pharmaceutical formulation, concentration and by synergistic effects with other nutracetical or pharmaceutical combinations. Moreover, also ALA improves insulin sensitivity, by virtue of the reduction in triglyceride accumulation in skeletal muscle [17] as a result of AMPK driven inactivation of acetyl-CoA carboxylase 2 (ACC-2 or β) and further increase in long fatty chain acid oxidation [18,19]. From a clinical point o view, ALA was reported to be used in dosages from 100 mg to 300 mg/die for the management of diabete mellitus as well as GDM [20-22]
All these promising informations from literature prompted us to evaluate retrospectivly the effects of a neutraceutical product containing RSV and ALA, Vitamins and minerals in pregnant women with GDM.
This retrospective cohort study collected recorded parameters from singleton prenancies at “San Pio” clinic in Vasto from September 2022 to February 2023. We considered pregnant patients with gestational diabetes mellitus (GDM) primarily managed with physical exercise and diet
The inclusion criteria were: age between 25 and 40 years, gestational age at enrollment between 24 and 28 gestational weeks, with a diagnosis of GDM. The diagnosis of GDM is made if there is at least one abnormal value (≥92, 180 and 153 mg/dL for fasting, onehour and two-hour plasma glucose concentration respectively), after a 75 g OGTT. Exclusion criteria were: pre-existing diabetes mellitus, cardiovascular diseases, chronic hypertension, autoimmune diseases, thyroid disease, age < 25 or > 40 years.
Patients were consecutively considered with a 1:1 ratio between cases and controls. The Control Group was primarily managed with physical exercise and diet, while the Study Group also recieved a food supplement (EgregiaTM, distributed by S&R Farmaceutici S.p.A) containing trans-resveratrol (62.5 mg) and alpha-lipoic acid (100 mg) (Revifastlipo®), polydatin (12.5 mg), magnesium (39 mg), folic acid (200 mcg) and vitamin D (12.5 mcg). These patients took the supplement with a daily dose of two tabs/day for 2 weeks followed by 1 tab/day until childbirth (Figure 1
The following variables were collected: age, pregestational BMI, rate of nulliparous patients, and mode of delivery (vaginal birth/cesarean section). The primary study outcome was the incidence of insulin requirement. Secondary outcomes were daily insulin requirement, fasting glucose level, postprandial glucose level, and incidence of large for date fetus.
Statistical software SPSS 28.0.1.1 (SPSS Inc., Chicago, IL, USA) was used for data analysis. All continuous variables were tested for normality with the D’Agostino-Pearson test. Normally distributed variables were expressed as mean ± standard deviation (SD), while not normally distributed variables were reported as median and interquartile range (IQR). The t-test or the Mann- Whitney test was used for comparison as appropriate. Qualitative variables were expressed as number and proportions and were compared with the Chi-square test or the Fisher’s exact test as appropriate. All the collected variables and outcomes were compared between cases and controls in a bivariate analysis.
A total of 80 singleton pregnancy patients with GDM were considered in this retrospective clinical trial (Figure 1). The mean ± SD age was 32.8 ± 5.1 years in the control group and 31.9 ± 4.7 years in the study group (RSV + ALA). The mean ± SD pregestational BMI was 26.6 ± 3.4 in the control group and 27.5 ± 3.6 in the study group (RSV + ALA). A total of 23 (57.5%) patients were nulliparous in the control group, while 15 (37.5%) patients were nulliparous in the study group. Cesarean section was performed in 11 (27.5%) patients in the control group and in 9 (22.5%) patients in the study group (RSV + ALA) (see Table 1). It should be noted that patient demographics were not significantly different between the two groups, paving the way for a fair and unbiased comparison of results (Table 1). Table 2 reports the outcome comparison between cases and controls. Patients with RSV/ALA supplementation presented a lower insulin require (15.0% vs. 37.5%, p = 0.02), a lower daily insulin requirement (11 ± 2 UI vs. 14 ± 3 UI, p < 0.0001), and lower fasting glucose level (87 ± 4 mg/dL vs. 93 ± 5 mg/dL, p < 0.0001).
The management with physical exercise, diet and nutraceutical support are often considered a first approach to manage GDM. This retrospective study shows how a nutraceutical combination based on RSV and ALA can reduce the levels of fasting glucose and insulin requirements and may have promising advantages in preventing GMD.
RSV is a natural polyphenol with numerous benifical health benefits. Previous studies in the animal model and in humans have reported that RSV improves the indicators of GDM by improving glucose metabolism and insulin tolerance, regulating blood lipids and plasma adipokines, and modulating embryonic oxidative stress and apoptosis. RSV can ameliorate the GDM complications by reducing oxidative stress, improving mitochondrial activity, reducing the effects on placentation and reducing the adverse effects on embryonic development [9,10,23]. Metabolic dysfunction and oxidative stress can also be associated with prevention and improvement of GDM, maternal obesity (MO), and intra-uterine growth restriction (IUGR) in fetoplacental and offspring metabolic health. This approach holds potential to mitigate developmental programming-related risk of chronic diseases, serving as a probable intervention for disease prevention also for the child [10]
Based on the ability of RSV to activate SIRT1 pathway in several cell models, our previous in vitro data from our laboratory showed the biological effects of RSV alone and in combination with ALA in HEPG2 cell line model. HEPG2 cell cultures were treated with 3 µM of RSV alone and in combination with 500 nM of ALA. After 24 hours of treatment the trascriptoma was investigated by using the PCR array with a selected pool gene involved in cell metabolism. Our data displayed that RSV decreased the expression of SREBF1 also known as SREBP-1 and that this expression was further reduced by co-treatment with ALA (supplemental Figure 1). Since SREBP-1 is involved in GDM [24], these in vitro results may also further underling the potential positive action of the combination of RSV with ALA and its benefits in metabolic complications such as GDM.
However, RSV is also known for its poor pharmacokinetic properties, mainly due to its physico- chemical behaviour (water solubility). Considering RVS's low solubility in water and high membrane permeability, it is a second class molcule based on the biopharmaceutical classification system (BCS) [25] and the main site of absorption is in the intestine through passive diffusion or active transport via ABC (ATP-dependent binding cassette) transporters [26]. Because of these conditions, it is often not easy to replicate in vivo the in vitro tests, or rather the opportunity to exploit the whole pharmacodynamic profile of RSV in vivo is not obtained [27].
For these reasons, we focused our attention on retrospectively analyzing the effects of a supplementation with a source of RSV, that is supported on magnesium dihydroxide (RSV@MD, tradename REVIFAST®), to guarantee improvements in the dissolution rate of RSV and a fast gastric absorption, thus gaining better pharmacokinetic properties and riproducibile biological and clinical data [28,29,26]. This specific source of RSV has already been studied with other active food supplement ingredients (es. red yeast rice, inositols) and have already been shown to ameliorate the cardio-metabolic function [30,31] and fertility in both males and females [32,33].
The mechanistic sinergy existing between RSV and ALA on AMPK/SIRT via SREBF1 could be the key to its benefical effects shown in this article in GDM (graphical abstract, Figure 2).
The nutraceutical studied in this clinical trial also contained magnesium and vitamin D. While there is some indication that vitamin D supplementation could reduce the risk of pre- eclampsia and increase length and head circumference at birth, further rigorous randomised trials are required to confirm these effects [34]. Epidemiological studies have reported discrepant findings on the relationship between folic acid intake during pregnancy and risk for GDM [35]. Furthermore, although less well known, the potential connection between magnesium and gestational diabetes is noteworthy. Magnesium is one of seven essential macrominerals which plays an important role in many physiological functions. A recent meta-analysis revealed that serum magnesium levels are lower in patients with GDM than in healthy pregnant women, and this discrepancy was most pronounced in European populations and during the third trimester [36]. Hypomagnesemia during pregnancy is prevalent and associated with increased GDM risk, especially in women followed by more plasma magnesium decrement during pregnancy [37].
The wider implications of GDM is a higher incidence of maternal morbidity in pregnancy in term of hypertensive disorders such as preclampsia [38]. Preclampsia, is a severe pregnant complication, mainly characterized by insufficient trophoblast invasion, impaired uterine spiral artery remodeling, placental hypoxia and ischemia, and endothelial dysfunction. Several studies showed that SIRT1 might play a vital role in the pathogenesis of preeclampsia. In fact, SIRT1 modulators such as RSV [39] and ALA [40] may be promising candidates for the prevention of these high risk maternal complication.
Current evidence is uncertain on the potential benefit and safety of RSV supplementation in pregnant women. This retrospective study shows that a RSV and ALA nutraceutical combination decreases the incidence of GDM. We speculate that this nutraceutical intervention taken during the last trimester can alter the impact of maternal BMI or GDM status, reducing both the requirment of insulin or neonatal complications, with no associated risk of adverse events and can possibly offer important preventative benefits towards high risk maternal and fetal complications
Human epatic cell line (Hep G2 [HEPG2]) was cultured at 37°C with 5% of CO2 in Dulbecco’s modified Eagle medium (DMEM; Euroclone) containing 10% fetal bovine serum (Euroclone), 200 mM glutamine, and 100 U/mL penicillin/streptomycin (Life Technologies). Cells were cultured in 75 cm2 cell culture flasks (Falcon, Corning) seeded at density of 1.5 × 104 cell/cm2 After adherence (24 hours after plating), cells were treated with (3µM) of RSV for 24 hours.
RNA from HEPG2 cells was extracted using the Trizol (Invitrogen) method according to the manufacturer’s instructions. For gene expression, RNA was reverse-transcribed into first-strand cDNA using the Kit RT2 First Strand and analyzed with PCR Array Lipoprotein Signaling & Cholesterol Metabolism (Qiagen) using RT2 SYBR Green ROX FAST Mastermix as a reagent (Qiagen) and Real- Time RotorGene 100 (Qiagen) following the manufacturer’s instructions. To normalize mRNA levels, the ACTB, GADPH and RPLP genes was assessed at the same time. The results were expressed as fold change comparing untreated, RSV (3µM) and RSV plus ALA (500 µM) treated cells
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships. RGI and GC are employees of S&R Farmaceutici S.p.A.
None
Not applicable. The study is considered a retrospective trial and the National Code on Clinical Trials has declared that ethics approval is not necessary for real retrospective studies [41].
Data is available upon request. To request the data, contact the corresponding author of the article.
Patient consent was waived due to due the retrospective study design
We kindly thank Silvia Rossi and Andrea Dottorini of S&R Farmaceutici S.p.A for the editorial assistance.

![]()

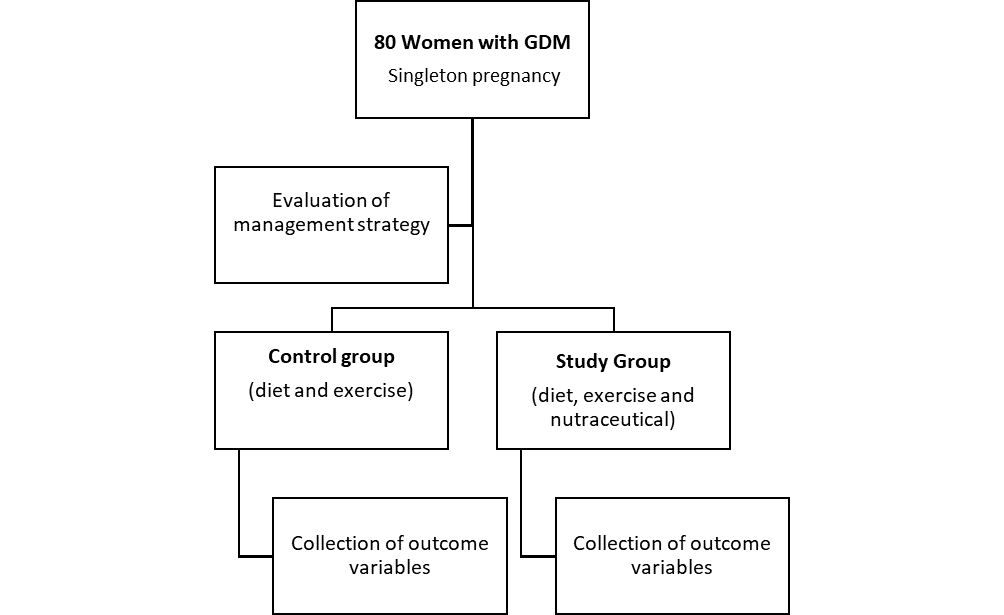 |
| Figure 1: Flow chart of retrospettive study design |
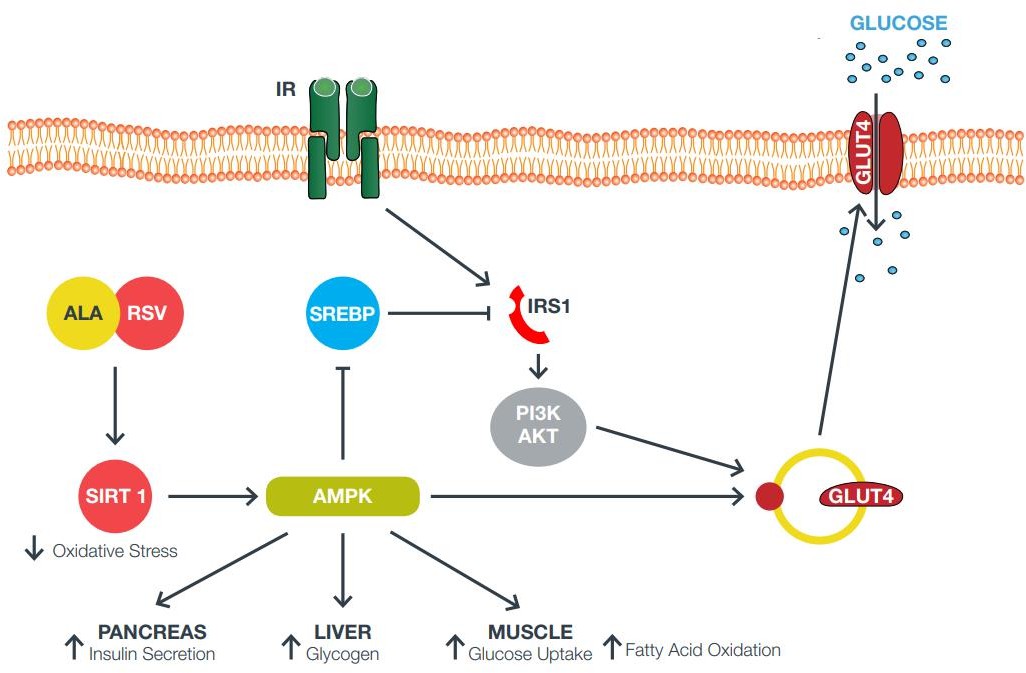 |
| Figure 2: Graphical abstract |
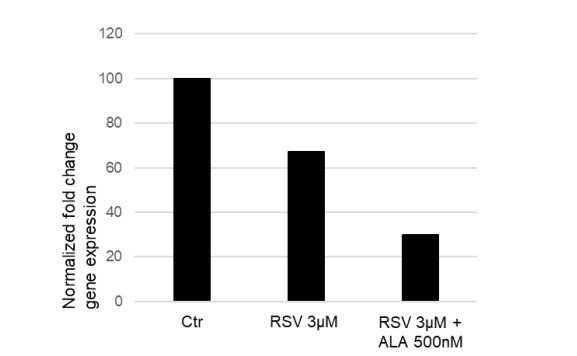 |
| Figure 3: Sterol regulatory element-binding transcription factor 1 (SREBF1) gene expression in HEPG2 cells treated with 3 M of resveratrol and co-treatment with 500nM lipoic acid at 37 degrees celcius for 24h. |
Patient demographic data |
Control |
RSV + ALA |
p |
Age |
32.8 ± 5.1 |
31.9 ± 4.7 |
0.41 |
Pregestational BMI |
26.6 ± 3.4 |
27.5 ± 3.6 |
0.25 |
Rate of nulliparous |
23/40 (57.5%) |
15/40 (37.5%) |
0.08 |
Mode of delivery |
|||
Cesarean section |
11/40 (27.5%) |
9/40 (22.5%) |
0.61 |
Vaginal delivery |
29/40 (72.5%) |
31/40 (77.5%) |
0.61 |
Outcome |
Control |
RSV + ALA |
p |
Insulin require |
15/40 (37.5%) |
6/40 (15.0%) |
0.02 |
Daily insulin requirement (IU) |
14 ± 3 |
11 ± 2 |
<0.0001 |
Fasting glucose level (mg/dL) |
93 ± 5 |
87 ± 4 |
<0.0001 |
Postprandial glucose level (mg/dL) |
142 ± 10 |
139 ± 7 |
0.12 |
Large for gestational age |
5/40 (12.5%) |
4/40 (10.0%) |
0.74 |




































