Open Access
Research Article
Max Screen
ISSN: 2393-9060
Copyright: © 2023 Rahim Rostami. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Objective: physiological changes during pregnancy modulate the endocrine system. This study was carried out with the aim of establishing thyroid specific reference range and prevalence of thyroid dysfunction in pregnant women in their first semester in mild- to moderate iodine deficient area.
Design: Women (n=648; age: 14-45 years old; without any history of thyroid dysfunction) were recruited in their first semesters. Healthy non-pregnant women were enrolled. Random urine- and blood samples were collected for the analysis of UIE,Thyrotropin (TSH), Free Thyroxine (fT4) and thyroid peroxidase antibody (TPO-Ab) respectively.
Results: TSH-specific reference range in 1stsemester was 0.05–2.8mIU/L and in non-pregnant women was0.6–3.95 mIU/L. The reference range for fT4 was 9.1–21.9 pmol/L and 9.1–19.5 pmol/L. TSH reference range was (30% –70%) lower than the Iranian previous reports.Serum TSH in pregnant and non-pregnant women with TPO-Ab positive was significantly higher than TPO-Ab negative individuals. The prevalence of hypothyroidism and isolated hypothyroxinemia were 4.9% and 13%.
Conclusions: TSH-specific reference values in 1st semesters differ from other studies with iodine sufficient status, and applying other reference rangescould lead to thyroid misclassification. Due to a high rate of hypothyroxinemia and iodine deficiency,fetues has predisposed psycho-motor developmental retardation. This preliminarily result suggested that whole body iodine stores areless likely adequate to prevent thyroid dysfunction during early pregnancy in regions with mild-moderate iodine deficiency
Keywords: Pregnancy,Thyroid Stimulating Hormone (TSH), Freethyroxine (Ft4), Thyroid-Specific Reference Range (TSRR), Urinary Iodine Concentration (UIC),Iodine Deficiency (ID), Thyroid Dysfunction, Hypothyroxinemia
Abbreviations: Pregnancy, Thyroid stimulating hormone (TSH), Free Thyroxine (fT4), TSH-specific reference range (TSRR), Urinary iodine concentration (UIC), iodine deficiency (ID), thyroxin-binding globulin (TBG), thyroxine (T4), thyroid hormones (THs).
Thyroid function has profoundly affected by pregnancy. During the first half of pregnancy thyroid is stimulated by HCG and estrogen which lead to decrease in levels of TSH and increase in levels of thyroxin-binding globulin (TBG). During gestation, renal iodide clearance significant increases by approximately 30–50% and, concurrently, thyroid hormone production in pregnancy gradually rise by 50% [1, 2]. At the same time, the placental deiodinase III (DIII), in uteroplacental unit, regulates T4 metabolism, distribution and availability for the mother and for the fetus in the first half of gestationbecause fetus in the first trimester heavily relies on mother for thyroid hormones and iodide [3, 4].
Iodine is an essential trace element for thyroid hormone synthesis and brain development, especially in early fetal psycho-motor development. Low iodine intake can cause thyroid dysfunction in pregnant women, particularly hypothyroidism and hypothyroxinemia [5]. Recent studies have suggested in mild-moderate iodine deficiency, thyroid stimulation by HCG leads to the preferential output of T3 over T4 and increasing TBG concentrations. This event leads to the progressive desaturation of TBG by T4, eventually resulting in a decline in FT4 concentrations. On the contrary, circulating T3 triggers negative feedback on pituitary TSH secretion, and the concentrations of TSH fall within the normal range. As a result, the women are clinically euthyroid even when biochemically hypothyroxinemia [6, 7]. Thus pregnant women are highly recommended to have an adequate iodine intake (10-20 mg iodine stored in the thyroid) and continue to digest more Iodine (150 to 249 µg/day) to be able to meet their requirements during the gestation period [8, 9].
Iodine is vital for thyroid hormone synthesis and fetal brain development. Low iodine intake in pregnant women can cause thyroid dysfunction. Mild-moderate deficiency can lead to decreased FT4 concentrations, but TSH levels remain normal. Pregnant women should consume 150-249 µg/day to prevent hypothyroxinemia.
Iodine as an essential trace element has a key role in thyroid hormones synthesis as well as brain development, especially during early fetuspsycho-motor development.In mild- to moderate iodine deficient area, pregnant women with low iodine intake have undergone thyroid dysfunction, especially hypothyroidism and hypothyroxinemia [5]. The recent studies have been suggested in mild-moderate iodine deficiency,thyroid stimulation by HCG leads to the preferential output of T3 over T4 and increasing TBG concentrations. This event leads to the progressive desaturation of TBG by T4, eventually resulting in a decline in FT4 concentrations. On the contrary, circulating T3 triggers negative feedback on pituitary TSH secretion, the concentrations TSH fall within the normal range. As a result, the women are clinically euthyroid even when biochemically hypothyroxinemic [6, 7]. Thus pregnant womenis highly recommended to have an adequate iodine intake (10-20 mgiodine stored in the thyroid) and continues to digest more iodine (150 to 249 µg/day) to be able to meet their requirements during gestation period [8, 9].
According to the American Thyroid Association (ATA), European Thyroid Association (ETA) and the National Academy of Clinical Biochemistry (NACB), establishing TSH-specific reference ranges using population study is highly recommended in order to establish diagnostic criteria for thyroid disorders and avoid misclassification of pregnant women for thyroid dysfunction [10-13]. Thyroid-specific reference range value are established by several studies in recent decades in iodine sufficient areas, in Iran [14-18]. Azizi, Delshad, Kianpour and Nazarpour defined TSH-specific reference range in 1stsemester in pregnant women, and their reference values was 0.2-3.9,0.2-5.1,0.20–4.60 and 0.14-6.14mIU/L [14-16, 18-20]. Their report differed from ATA and ETA reference range [16]. However, many factors such as iodine intake[1, 2], ethnicity, gestational age[21], laboratory assay methods [22], the study design method, and selection of the reference population[18, 23-25] can affect the reference ranges of thyroid. The effect of marginally iodine sufficient on pregnant women and their offspring did not well understand.
Owing to inadequate data available for the trimester-specific reference intervals in Iranian pregnant women, we carried out this study to establish specific reference ranges for thyroid function tests in healthy pregnant women during their first gestation in marginal iodine sufficient area, Urmia County, North-west of Iran.
This cross-sectional study, performed in Urmia, an area of marginal iodine sufficiency (October, 2009 and December, 2009).
Pregnant women attending prenatal care units in Urmia County were interviewed and demographic information was collected by trained midwives. Sample size calculation (n=394) was based on the prevalence of iodine deficiency in WA Province according to 3rd National Iranian Survey [26]. To enhance the statistic power of the study, sample size was increased to 490 subjects. The studied population was allocated to five districts comprising 12 prenatal care centers. Sample size in each prenatal care was calculated according to annual live birth rate employing Population Proportionate Sampling Approach.
Blood samples (5 mL) were collected by venous puncture from pregnant and non-pregnant women. The blood sample was allowed to stand for 10 min at room temperature and subsequently centrifuged at 1000 ×g for 15 min. Serum aliquot (250 μL) was transferred into Eppendorf tubes and kept −70 °C until TSHand FT4 analysis.
Fasting Urine samples (10 mL) were collected at 1st trimester. The samples were kept at -20oC until UIC testing the modified Sandell–Kolthoff digestion method [27]. Results are given as microgram of iodine per liter of urine (µg/l). Inter-assay and intra-assay coefficient variation (CV) of the UIE measurement method were 6.5% and 8%.
Data handling was carried using SPSS software for windows version 22 (SPSS Inc., Chicago, USA). The normality of UIE, fT4 and TSH in 1st and women of child-bearing age was checked using a histogram and the kolmogrov–Smirnov test. We employed a t-test for comparison of fT4 and UIE, and the non-parametric data were analyzed by the Mann–Whitney test U-test for comparison of TSH between the two groups. Data are expressed as mean±SD and median. Correlations between UIE, TSH and fT4 were examined using Spearman’s rank correlation coefficient. P-values ≤0.05 was considered statistically significant.
Established reference ranges, according to 5 percentiles and 95 percentiles, were used to classify maternal thyroid function as (a) high and low levels of each thyroid function test and as (b) overt (abnormal TSH and fT4) and subclinical (isolated abnormal TSH) hyper- and hypothyroidism as well as hyper- and hypothyroxinemia (isolated abnormal fT4). Thus, the term “abnormal” thyroid function designates thyroid function test results outside the reference ranges in this study
The study was approved by the Ethics Committee of Urmia University of Medical Sciences, Urmia, Iran (Ethics code: IR.umsu.rec.1388.32). Informed written consent was obtained from all participants prior to study entry
The exclusion criteria for pregnant women was pregnancy history (miscarriage, multiparous, preterm delivery and abortions) and medical history (including thyroid medications, history of thyroid disease and thyroid antibodies). Women of child-bearing age (n=181) was recruited as control group with no history of thyroid dysfunction and thyroid medication. The including/excluding process was described in diagram 1. Subjects with TPO-Ab positive antibody was excluded in both groups.
Table 1 displayed the demographic and biochemical characteristic of pregnant women in first trimesters and women of child-bearing age with negative TPO-Ab, residing in Urmia County. The mean±SDof age for 438 pregnant and 156 non-pregnant women was 25.4±5.1 and 24.9±6.7 old years, respectively (P=0.21). More details about the basic and clinical characteristics of participants in both groups are presented in Table 1.
According to 5th and 95th percentiles, the Reference ranges for TSH and FT4 valuesin the first trimester of gestation were 0.05- 2.8 mIU/l and 9.1- 21.9 pmol/l, and in non-pregnant women were0.6 – 3.95mIU/l and 9.1 – 19.1 pmol/L respectively. Iodine deficiency (< 150 µg/L) was found in 87% of pregnant women and in 18% of non-pregnant women. However, no significant difference was observed between pregnant women and non-pregnant with and without iodine deficiency in thyroid function (Table 2).
TPO-Ab was positive in 10.6% of pregnant (52/490) and 13.8% of non-pregnant (25/181) women.Pregnant women with positive TPO-Ab had a higher median, 5th and 95th percentiles of TSHthan pregnant women with negative TPO-Ab. The same results were obtained for non-pregnant women that presentsin Table 3.No significant correlation was observed between TSH and UIC in both TPO-Ab positive and TPO-Ab negative groups, whereas significant inverse correlation was observed between TSH and fT4 in pregnant women with and without TPO-Ab (all P < 0.05).Serum fT4 in pregnant women with positive TPO-Ab was significantly lower than pregnant women without TPO-Ab (13.3±4.3 pmol/L vs.14.7±4.7pmol/L; P=0.03).
According to our reference range the prevalence of hypothyroidism, hyperthyroidism, Hypothyroxinemia and Hyperthyroxinemia was assessed. The prevalence of subclinical and overt hypothyroidism was 4% and 1%, whereas the prevalence of subclinical and overt hyperthyroidism was 4.9% and 1%. The percentage of pregnant women presenting Hypothyroxinemia and Hyperthyroxinemia was 13% and 2.5%.
In 1st semester, significant positive correlation was observed between TSH levels with UIC and TPO-Ab (r= 140; r= 0.190; all P< 0.05), whereas negative significant association was seen between UIC and Tg-Ab (r = ‒ 0.118; P< 0.05). However, in pregnant women there was an inverse association between TSH and fT4 (r = ‒ 0.; P< 0.05). in controls, no significant correlation was detected between different parameters.
The study aimed to establish Thyroid Specific Reference Range for pregnant women in their 1stsemester of pregnancy. In present study, we assessed levels of serum TSH, FT4, TPO-Ab and MUIC in pregnant women in 1st semester in comparison to non-pregnant women
In the present study, pregnant women were at the age of 7-10 weeks of Gestation. The significant difference was observed between pregnant women and non-pregnant women in TSH values (figure 2A). It is well established that in the early weeks of gestation (between 7-12) TSH levels are suppressed because of elevated HCG and Estrogen [1]. However, in both groups, fT4 was similar and did not show any significant difference.Kianpour et al (ref 15). revealed that TSH levels is suppressed in pregnant women relative to non-pregnant women, in line with other studies [28].
Establishing a Thyroid reference range in first semester 7-12 weeks of pregnancy is suitable because serum TSH was beginning to decrease after 7 weeks of gestation. In our study, the thyroid reference range was established using 5 percentiles and 95 percentiles at the 7-10 weeks of pregnancyIn the present study, the TSH reference range in pregnant women withnegative TPO-Ab was 0.05 - 2.8 mIU/L and in non-pregnant women with negative TPO-Ab was 0.6 - 3.95 mIU/L. Karakosta et al [29].reported that TSH reference in pregnant women without TPO-Ab was 0.05 - 2.53 mIU/L, which was similar to our results. Furthermore, in recent studies from Iran, the TSH reference range in pregnant women was0.14 - 6.14 mIU/L and 0.20–4.60 mIU/L [16, 18]. Other studies from iodine sufficient to iodine excess area, such as Chile, Korea and China revealed that TSH reference values were higher than that present study (table 4) [14-16, 18].
In Iran, Azizi and Mehran [14, 15] in cross-sectional studies applied P5 and P95 for the TSH reference range and their figure for 1st semester was similar (0.20 – 3.90 mIU/L and 0.20 – 3.90 mIU/L), whereas the highest values for upper and lower of TSH concentration (2.5th and 97.5th percentiles) was reported by Nazarpour and Kianpour (0.05 - 2.8 mIU/Lvs. 0.14 - 6.14 mIU/L and 0.20–4.60 mIU/L). Ourlower and upper limits for TSH were different from previous Iranian reports and these figures was 30-70% lower than previous studies [16, 18] (Table 4).
Taken together, these regional discrepancies might also originate from iodine intake status, ethnicity and racial differences of maternal HCG, gestational age at sampling, genetic characteristics, study design, assay methods, and inclusion criteria for the determination of reference population and sample size [30-34].
To elucidate, the discrepancy between our findings with previous reports from other reports from Iran, it is suggestedthat iodine deficiency is the main risk factor of pregnant women residing in the north-West of Iran, which should be taken into consideration [35, 36]. In Tehran and Isfahan, iodine status was optimal to more than adequate in pregnant women and schoolchildren [14-16, 18], while in Urmia iodine deficiency was 87% (sever ID: 33.3% and mild to moderate ID: 53.7%) [37, 38]. Moleti et al revealed that long iodine intake before pregnancy would increase TSHlevels in comparison to women with low iodine intake [5]. However, it has been suggested that Increment in TSH levels due to long iodine intake could replenish thyroid iodine storage or could increase the risk of maternal hyperthyrotropinemia in mild- to moderate iodine deficient pregnant women [5, 39]. In iodine deficient nations such European countries and United State (US) thyroid reference range were lower than in societies with high iodine intake [5]. Furthermore, Abel et al [4]. Demonstrated that iodine deficiency affected thyroid function and triggered auto-regulatory mechanisms in the thyroid and other tissues to maintain euthyroid status. They reported there was an inverse association between iodine and thyroid function (fT4), which indicated thyroid synthesis is inhibited to adjust with iodine intake during pregnancy likethe Wolff-Chaikoff effect. Taken together, it has been indicated mild- to moderate ID should carefully be monitored before pregnancy since initiating supplement use in pregnancy to prevent adverse effects on thyroid function.
Our results revealed that the prevalence of TPO-Ab positive in pregnant women was 10% rather than 13% in non-pregnant women. Other studies reported various percentages of TPO-Ab in pregnant women (10% to17%),respectively [40, 41]. In the present study, in pregnant women with TPO-Ab positive, the median of TSH and TSH Reference rangewere higher than negative TPO-Ab individuals (1.6 vs. 0.8 mIU/L and 0.2 – 4.2 mIU/L vs. 0.05 – 2.8 mIU/l); P< 0.05), whereas fT4 was lower in pregnant women with positive TPO-Ab rather than those with negative TPO-Ab. Our finding line with previous studies [18, 42].
Bhattacharyya et al [42]. Reported that in pregnant women with TPO-Ab, TSH concentration was significantly higher than pregnant women without TPO-Ab (2.31 µIU/ml vs. 1.73 µIU/ml). Kianpour et al [18]. Reported TSH value is high in TPO-Ab positive pregnant women than those of TPO-Ab negative pregnant women (0.09 – 8.81 vs. 0.2 – 4.65 mIU/L). As represented in figure 2C, our results revealed that the median of TPO-Ab was significantly lower than non-pregnant women. It was suggested that T regulatory cells (phenotypically CD4+, CD25+) in maintaining peripheral tolerance and preventing autoimmune disease.Taken together, Antibody status influences Thyroid function in the first and early second trimester, and treatment TPO-Ab positive pregnant Women with levothyroxine reduced the negative pregnancy outcomes [43]. This suggests that women with positive TPO-Ab should be excluded from the studies that aim to define the reference ranges for TSH concentration [44, 45].
According to our reference range, the prevalence of subclinical and overt hypothyroidism was 4% and 1%, whereas the prevalence of subclinical and overt hyperthyroidismwas 4.9% and 1%. The percentage prevalence of Hypothyroxinemia and Hyperthyroxinemia was 13% and 2.5%. In the latest study, Delshad and colleagues reported that the prevalence of subclinical hypothyroidism and hypothyroxemia are 10.5% and 0.53%, and only 5.7% of pregnant women is TPO-Ab positive [19]. Other studies from Tehran and Isfahan reported the prevalence of thyroid dysfunction was 10.8% and 5.5%, while none had isolated hypothyroxinemia [18, 20].
While, based on manufacturer’s recommended reference ranges, 7.89 % of women would have been diagnosed with hypo- and hyperthyroidism and 9.75 % with isolated hypothyroxinemia. According to the ATA (up to 2.5) reference range, 8% of our pregnant women had hypo- or hyperthyroidism and 6 % presented isolated hypothyroxinemia.
The difference between the prevalence of thyroid dysfunction in our study and previous studies might be attributed to the local reference range and assessment methods. Nonetheless, the high prevalence of hypothyroxemia in present study revealed that mild-- to-moderate iodine deficiency could upregulate type 1 and 2 iodothyronine deiodinase (DIO1& DIO2), catalyzing the deiodination of T4 to T3.Therefore, in pregnant women with mild to -moderate iodine deficiency, thyroid auto-regulatory response occurs and the synthesis and secretion of thyroid hormones is altered and switched towards a preferential use of the decreasing iodine supply in favour of secretion of T3 over T4, leading to decreased T4 and normal or increased T3 [46].Moleti et al. in the cohort study revealed iodine ingestsfor a long time before gestation (> 2 years) could reduce the percentage of isolated hypothyroxinemia rather than women with limited iodine intake or never has the history of iodine intake before becoming pregnant.Their results revealed that, the overall prevalence of isolated hypothyroxinemia in women with iodine intake was lower than in women with low iodine intake / no iodine intake (8.3% vs. 9.5%, and 20%), respectively [5].In line with Moleti’s findings, our results revealed that 16% of pregnant women with positive TPO-Ab was Hypothyroximic and their MUIC was lower than Euthyroxine individuals (44 µg/L vs. 81 µg/L).
Taken together, low fT4 levels in pregnant women indicating the progressive depletion of intra-thyroidal iodine stores caused by a persistently negative iodine balance [47]. A large Population base study is deemed to clarify the impact of iodine deficiency on thyroid function, thyroid autoantibodies and iodine excretion during gestation.
In preset study, our volunteer largely from both rural and urban population. In spite of different in their socioeconomic status and lifestyles, their main source of iodine was iodinated salt. Another limitation was lack of assessment of thyroid volume by Ultrasound that help to evaluation the effect of pregnancy and iodine deficiency on thyroid volume. Our study relied on a single blood sample drawn in early pregnancy and consecutively collected blood samples from each individual within the early pregnancy weeks would enhance the findings.
Owing to the higher rates of iodine deficiency and physiological changes during gestation, establishing a TSH-specific reference range in pregnant women is essential for Urmia County. TSH values in 1st semesters differ from other studies from iodine sufficient areas, and applying other reference ranges would lead to thyroid misclassification. Iodine deficiency may increase the risk of hypothyroxinemiain the first half of pregnancy, and its negative consequence has affected the fetus’s psychomotor development. This preliminary result suggested that whole body iodine stores are less likely adequate to prevent thyroid dysfunction during early pregnancy in regions with mild to moderate iodine deficiency. Therefore, continuing to monitor iodine intake in pregnant women is essential for preventing iodine deficiency and its negative impact on offspring.

![]()

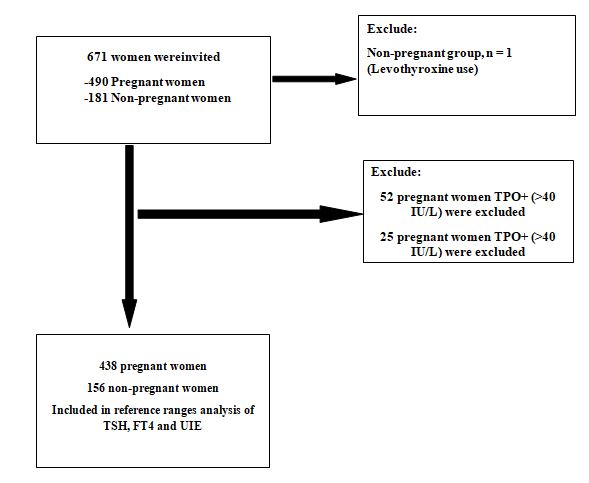 |
| Figure 1: Flow chart of the study design. Exclusion and inclusion criteria for pregnant women and non-pregnant women |
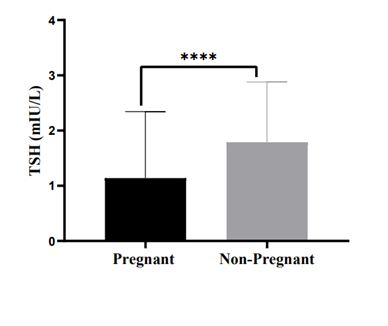 |
| Figure 2a: comparing the levels of TSH, TPO-Ab and MUIC in pregnant and non-pregnant women |
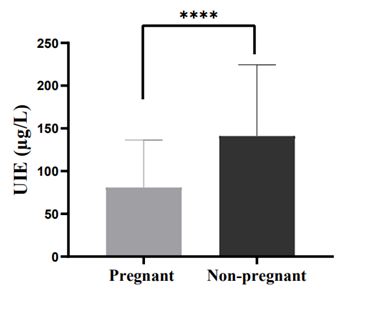 |
| Figure 2b: comparing the levels of TSH, TPO-Ab and MUIC in pregnant and non-pregnant women |
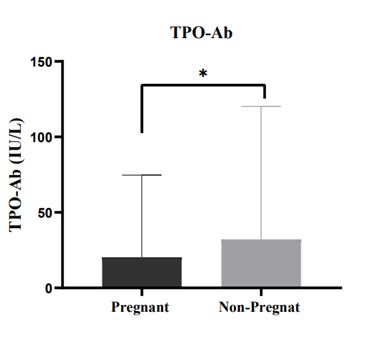 |
| Figure 2c: comparing the levels of TSH, TPO-Ab and MUIC in pregnant and non-pregnant women |
|
Pregnant women (1st) |
Non-pregnant women |
P-Value |
Age |
25.4±5.1 |
24.9±6.7 |
0.458 |
BMI |
24.9±4.1 |
20.9±3.8 |
---- |
Gestational Age |
9.0±2.0 |
---- |
----- |
Iodinated Salt |
20±5 |
20±4 |
NS |
TSH (mIU/L) |
0.80 |
1.7 |
0.001 |
Age<25 years |
0.9 |
1.8 |
----- |
Age 25 – 29.99 years |
1.0 |
1.4 |
---- |
Age 30 – 34.99 years |
0.70 |
1.25 |
--- |
Age >35 years |
0.75 |
1.25 |
---- |
5th percentile of TSH |
0.05 |
0.6 |
---- |
50th percentile of TSH |
0.85 |
1.6 |
|
95th percentile of TSH |
2.8 |
3.95 |
---- |
FT4 (pmol/L) |
14.6 |
13.5 |
0.009 |
5th percentile of FT4 |
9.1 |
9.1 |
---- |
50th percentile of FT4 |
14.2 |
14.5 |
|
95th percentile of FT4 |
21.9 |
19.5 |
----- |
UIE (µg/L) |
74 |
144 |
0.001 |
Urine Cr (mg/dL) |
1.47 |
1.34 |
0.01 |
UIC/Cr ratio (µg/mg) |
47 |
134 |
0.001 |
TPO-Ab (IU/L) |
2.6 |
3.3 |
0.03 |
Variable |
Pregnant women |
Non-Pregnant women |
||
|
Iodine deficient |
Iodine sufficient |
Iodine deficient |
Iodine sufficient |
TSH* |
|
|
|
|
Median |
0.9 |
0.8 |
1.90 |
1.7 |
P5 – P95 |
0.05 – 2.8 |
0.1 – 3.3 |
0.49 – 5.1 |
0.6 – 4.1 |
fT4* |
|
|
|
|
Median |
14.2 |
14.1 |
12.9 |
14.2 |
P5 – P95 |
9.0 – 21.9 |
9.1 – 21.9 |
10.1 – 22.1 |
9.1 – 19.4 |
variable |
Pregnant women |
|
Non-pregnant women |
|
||
|
TPO + |
TPO ‒ |
P-value |
TPO + |
TPO ‒ |
P-value |
TSH* |
|
|
|
|
|
|
Median |
1.6 |
0.8 |
0.001 |
2.1 |
1.7 |
0.05 |
P5 – P95 |
0.2 – 4.2 |
0.05 – 2.8 |
0.03 |
0.75 – 5.5 |
0.6 – 3.95 |
----- |
fT4* |
|
|
|
|
|
|
Median |
11.6 |
14.1 |
0.03 |
14.1 |
12.9 |
0.150 |
P5 – P95 |
7.7 – 25.1 |
9.1 – 21.9 |
----- |
9.1 – 23.1 |
9.1 – 19.3 |
----- |
Study |
Country |
Sample size and |
Centiles’ used |
TSH reference intervals 1st trimester |
Non-pregnant women |
Preset study 2019 |
Iran |
Cohort |
P5 – p95 |
0.05 – 2.8 |
0.6 – 3.95 |
Azizi F 2012 |
Iran |
Cohort |
P5 – p95 |
0.20 – 3.90 |
----- |
Delshad 2021 |
|
|
|
|
|
Mehran L 2013 |
Iran |
Cohort |
P5 – p95 |
0.20 – 3.90 |
----- |
Karakosta 2011 |
Greece |
Cohort |
P2.5 – P97.5 |
0.05 – 2.53 |
------ |
Nazarpour S2018 |
Iran |
Cohort |
P2.5 – P97.5 |
0.14 - 6.14 |
------ |
Kianpour et al. 2019 |
Iran |
cross sectional |
P2.5 – P97.5 |
0.20–4.60 |
0.59–5.60 |
Zhang D et al. 2019 |
China |
Cohort |
P5 – P95 |
0.02 – 3.78 |
----- |
Kim H et al. 2018 |
S. Korea |
Cohort |
P5 – P95 |
0.03 – 4.24 |
------ |
Kostecka-Matyja, M2017 (24) |
Poland |
Cohort |
P5 – P95 |
0.009-3.177 |
------ |
Khalil A et al. 2018 |
UEA |
Cohort |
P5 –P95 |
0.094 – 3.33 |
------ |
Ollero MD |
Spain |
Longitudinal |
P5 – P95 |
0.13 – 4.16 |
------- |
Goel et al 2021 |
India |
Cross-sectional |
P5 – P95 |
0.59 –4.48 |
------ |
Castillo C et al.2018 |
Chile |
Cross-sectional |
P2.5 – P97.5 |
0.13 – 5.37 |
----- |




































