Open Access
Research Article
Max Screen
ISSN: 2393-9060
Copyright: © 2023 Jestin V Thomas. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: Occasional constipation is associated with infrequent bowel movement and difficulty in passing stools without any obvious symptoms. Ginger has been used traditionally to manage various gastric conditions like constipation, dyspepsia, belching, bloating, epigastric discomfort, indigestion, nausea, and vomiting. The current study evaluated the effects of a standardized Ginger extract (GE) on objective and subjective markers of occasional constipation in a randomized, double-blind, parallel, placebo-controlled design.
Methods: Sixty adults with occasional constipation were randomized in 1:1 ratio to receive either 280 mg of GE or placebo, one capsule every night after dinner for 8 weeks. The change in outcomes associated with occasional constipation were measured at various time points from baseline during the course of supplementation. These included Patient Assessment of Constipation Symptoms (PAC-SYM), Patient Assessment of Constipation Quality of Life (PAC-QoL), stool consistency using Bristol Stool Scale, stool frequency using subject diary, gut immunity and inflammatory biomarkers, fecal microbiota composition and short chain fatty acids. Safety was assessed by monitoring adverse events, hematology and clinical chemistry tests.
Results: Fifty-five subjects (29 in GE and 26 in placebo) completed the study. GE group demonstrated significant improvements (p< 0.05) in PAC-SYM and PAC-QoL scores on days 28 and 56 and in stool frequency on days 14, 28 and 56 as compared to placebo. We also observed significant improvement (p< 0.05) in levels of Secretory Immunoglobulin A (SIgA), a marker of gut immunity on day 56. After 8 weeks of supplementation, GE group showed significant increase in relative abundance of bacteria from phyla, Patescibacteria, genera Weisella, Enterococcus, Pseudomonas, Eubacterium coprostanoligenes and significantly reduced relative abundance of genera Megamonas and Catenibacterium, which was not observed in the placebo group. Furthermore, the Firmicutes/Bacteroidetes (F/B) ratio was increased in the GE and placebo groups on day 56; however, the GE group had a lower F/B ratio than the placebo group. No significant change in fecal SCFAs was observed for GE as compared to placebo. GE was well tolerated throughout the study without any related adverse events.
Conclusion: Supplementation with GE for 8 weeks significantly improved occasional constipation symptoms, stool frequency, quality of life, and SIgA levels with few alterations in the fecal microbiome. Further, GE was found to be safe and well tolerated.
Abbreviations: AE = Adverse Event; ALT = Alanine Transaminase; ANOVA = Analysis of Variance; AST = Aspartate Transaminase; ASV = Amplicon Sequence Variants; BMI = Body Mass Index; CBC = Complete blood count; CONSORT = Consolidated Standards of Reporting Trials; CTRI = Clinical Trials Registry of India; DNA = Deoxyribonucleic Acid; F/B ratio = Firmicutes to Bacteroidetes ratio; FDR = False Discovery Rate; GE = Ginger Extract; HBD-2 = Human Beta-Defensin-2; HFD = High-Fat Diet; IBS = Irritable Bowel Syndrome; ICH = International Conference for Harmonization; ICMR =Indian Council of Medical Research; IL-6 = Interleukin-6; MAFFT = Multiple Alignment using Fast Fourier Transform; PAC QoL= Patient Assessment of Constipation Quality of Life; PAC SYM= Patient Assessment of Constipation Symptoms; PCoA = Principal Coordinate Analysis; rRNA = Ribosomal Ribonucleic Acid; SAE = Serious Adverse Event; SCFA - Short Chain Fatty Acids; SD = Standard Deviation; SIgA = Secretory Immunoglobulin A; SSU = Small Sub Unit; TNF = Tumour Necrosis Factor.
Keywords: Ginger; Gastrointestinal Disorder; Constipation; Gut Microbiota; SFCA; PAC
Occasional constipation is defined as an irregular bowel habit that occurs only occasionally or intermittently. This involves a decrease in bowel movement frequency and/or difficulty in passing stools without any obvious symptoms [1]. Constipation creates bowel distension, abdominal pain, headache, dizziness, and poor appetite and affects normal quality of life in affected individuals [2]. Causes of constipation may be genetic, diet, immobility, hormonal disturbance, pharmacological effects, or bodily anatomy. Further, gut microbiota that is a combination of bacteria, archaea and eukarya living in the gastrointestinal tract may also contribute to constipation and its related symptoms [3,4]. Gut microbiota also help in regulation of digestive process in gut to break down the food into absorbable nutrients, prevents the colonization of pathogenic bacteria, and produce metabolites such as short- -chain fatty acids (SCFA), bile acids, and many neuro-modulatory substances [5,6]. Several studies suggest that the dysbiosis of gut microbiota through modulation of metabolic activities causes functional constipation and related to irritable bowel symptoms. Significantly higher levels of bacterial species such as Veillonella species, Firmicutes, including Clostridium species, Enterobacteriaceae and sulfate-reducing bacteria whereas lower levels of Actinobacteria, Bacteroidetes, Bifidobacteria and Lactobacillus was found to be associated with patients suffering from irritable bowel syndrome associated with constipation [3,7]
Ginger is a widely used spice and is known to help to manage gut conditions including constipation, diarrhea, dyspepsia, belching, bloating, gastritis, gastric ulcerations, indigestion, nausea, and vomiting [8,9]. Ginger (Zingiber officinale) belongs to the Zingiberaceae family and contains over 400 phytochemical actives, most prominently oils such as gingerols and shogaols [10]. Ginger has traditionally shown anti-inflammatory, antioxidant, anticancer, and antiulcer properties with gastro-protective effects [8,9,11,12]. Further, ginger treatment modulates relative abundance of certain gut microbiota that is associated with amelioration of dextran sulfate sodium-induced colitis in mice [13].
Use of supplements from traditional sources are preferred by consumers to manage occasional constipation issues [14]. Given the widely established medicinal properties and safety of ginger, it is increasingly being pursued as an important natural product for gut health [15].
Here we report the results of an efficacy study for standardized ginger extract containing 10% gingerols in subjects with occasional constipation through the assessment of clinical end points, gut immune function, and the effect on the gut microbiome.
Study material: The ginger extract (GE) standardized to 10% Gingerols (commercially known as GingeverTM) was obtained from OmniActive Health Technologies (India) as capsules. Each capsule contained ≈ 86 mg of GE to deliver 12 mg of gingerols and 194 mg of microcrystalline cellulose to make a total capsule of 280 mg, whereas the placebo capsule contained 280 mg of microcrystalline cellulose.
Study products were filled in opaque red-colored hard gelatin capsules to maintain double-blindness. Subjects were randomly assigned to the GE and placebo groups and instructed to consume one capsule every night after dinner at the same time every day for 56 days.
This was a randomized, double-blind, parallel, placebo-controlled, clinical interventional study with administration of the investigational product for 56 days. A prior written approval for conducting the study was obtained from BGS Global Institute of Medical Sciences Institutional Ethics Committee, Bengaluru, India.The study was conducted as per the guidelines of Indian Council of Medical Research (ICMR), International Council for Harmonization (ICH) - Good Clinical Practice (E6R2), and the Declaration of Helsinki. The study was registered with the Clinical Trials Registry of India (CTRI/2022/01/039843).
Adult healthy males and/or females aged between 18 and 65 years who reported with < 3 bowel movements per week for at least 2 weeks but not more than 12 weeks in the past 6 months and met all inclusion and no exclusion criteria were enrolled in the study after voluntarily signing a written informed consent.
The study was scheduled with a screening visit of 7 days, a randomization/baseline visit, follow up visits on Days 3, 14 and 28, and an end of study visit on Day 56. The total duration of the study was approximately 63 days, including a screening period of 7 days.
Demographic details such as age, gender, height, body weight, body mass index (BMI), and medical history, including hypertension, diabetes mellitus, chronic liver, gastrointestinal and renal disorders, surgeries, and any other clinically significant medical and medication history, were obtained. Urine pregnancy test for females of child-bearing potential were performed during screening and end of study visit.
The eligible subjects were randomly assigned in 1:1 ratio to either GE or placebo groups at the randomization visit in a double-blinded manner. The randomization schedule was generated by R software version 4.2.1 using a block randomization method using block of 4 by an independent non-study expert. Subjects were instructed to maintain their current diet without making any significant changes to it and monitored using subject diaries
Safety assessments included monitoring of adverse events (AEs), physical examination, vital signs measurement, urine pregnancy tests (for females of child bearing potential), haematology, and clinical chemistry tests.
Abdominal, rectal, and stool-related symptoms were measured by the Patient Assessment of Constipation Symptoms (PAC-SYM) questionnaire, and quality of life (QoL) by the Patient Assessment of Constipation (PAC-QoL) score. Stool frequency was assessed by the number of bowel movements per week and stool consistency by the Bristol Stool Scale. A stool sample was collected for assessment of Secretory Immunoglobulin A (SIgA), Human Beta-Defensin 2 (HBD-2) and faecal microbiota composition. Blood samples were collected for assessment of inflammatory markers (Tumour Necrosis Factor (TNF)-alpha and interleukin (IL)-6) and safety assessment (complete blood count (CBC), liver function tests [alanine transaminase (ALT), aspartate transaminase (AST)], and serum creatinine). Faecal SCFA (acetate, propionate, and butyrate) assessments were conducted in sub-groups of 15 subjects per group at baseline and Day 56.
Subjects who met all the inclusion criteria were included in the study. The criteria were as follows: healthy male or female adults, aged 18 to 65 years (both limits inclusive), had a BMI of 18.5 Kg/m2 to 29.9 Kg/m2 (both limits inclusive), had < 3 bowel movements per week for at least 2 weeks (but for not more than 12 weeks in the past 6 months) prior to screening, agreed to maintain their usual level of activity throughout the trial period, agreed to maintain their usual dietary habits and level of exercise, maintain their usual lifestyle, and agreed to stay weight stable during the study period.
Subjects who met any of the following criteria were excluded from the study: had hypersensitivity or history of allergy to the study product, suffered from a metabolic disorder or from a disease found to be inconsistent with the conduct of the study by the investigator, diagnosed with functional constipation as per Rome III criteria, major gastrointestinal complication (Crohn's disease, ulcers, Irritable bowel syndrome (IBS) - Mixed, IBS-Constipation, IBS-Diarrhea, Celiac disease, Inflammatory bowel disease), suffered from lactose intolerance, prior abdominal surgery (gastric by-pass, gastrectomy, gastric band, visceral surgery) that in the opinion of the investigator, might present a risk for the participant or confound study results, undergoing pharmacological treatment related to constipation (pro-secretory agents, antibiotics, antidepressants, antispasmodics, enterokinetic), dietary treatment of constipation (e.g. probiotics, prebiotics, symbiotic, herbal extracts, fibres), or other constipation treatments (e.g. cognitive behaviour therapy, acupuncture, biofeedback) or within 1 month before screening, used laxative/suppository ≥1 times /month or laxative/suppository used within 48 hours of screening (rescue medications - e.g., laxatives, suppositories and rescue procedures- e.g., enemas, allowed for intolerable symptoms during study), daily consumption of probiotics, prebiotics, symbiotic, fibres, fermented milk, and/or yogurt containing probiotics within 1 month prior to screening, used any drug or dietary supplement during at least 7 consecutive days known to cause constipation (e.g. iron, opioids, sucralfate, misoprostol, 5-hydroxytryptamine (HT) -antagonists, antacids with magnesium, calcium or aluminium, antidiarrheal medication, anticholinergic agents, calcium supplements, calcium channel blockers, tricyclic antidepressants or non-steroidal anti-inflammatory drugs (NSAIDs)) within 1 month before screening, had clinically significant underlying systemic illness that could preclude the participant's ability to complete the trial or that might confound the study outcomes (e.g. bowel cancer, prostate cancer, terminal illness), used systemic steroid within 1 month before screening, had eating disorder (e.g., anorexia, bulimia, etc.), had a lifestyle deemed incompatible with the study according to the investigator e.g., specific diet (vegetarian, vegan, hypo caloric), intense physical activity > 10 hours / week, etc., self-declared history of alcohol abuse (for females: >3 drinks on any single day and >7 drinks per week; for males: >4 drinks on any single day and >14 drinks per week, had other causes of secondary constipation, had been treated with any investigational drug or investigational device within a period of 3 months prior to study entry, were pregnant, nursing or planning a pregnancy within the study participation period, any additional condition(s) that in the investigators opinion would warrant exclusion from the study or prevent the subject from completing the study.
The sample size calculation was based on the difference between the results of the baseline and end of study visits of the subjects that are considered medically relevant. A total of 60 subjects were enrolled in the study by assuming that a minimum of 25 subjects per group, including a 15% dropout rate, were sufficient to detect a mean difference of 1.175 with a common standard deviation (SD) of 2.0 at the end of treatment between the baseline and end of the study with a power of 80% and a 0.05 two-sided level of significance.
The PAC-SYM Questionnaire is used to measure the subject's experience of symptoms and symptom severity in constipation over time. The PAC-SYM questionnaire was administered to assess abdominal, rectal, and stool-related symptoms of constipation at baseline (Day 0) and follow-up visits (Days 3, 14, and 28), and end of study (Day 56).
The PAC-QoL Questionnaire is the most validated and specific tool for measuring the quality of life of subjects with constipation. PAC-QoL is a self-reported questionnaire consisting of 28 items grouped into four subscales assessed at baseline (Day 0), follow-up visits (Days 3, 14, and 28), and the end of study (Day 56).
Stool consistency data was collected using the standard tool, the Bristol Stool Scale, which measures stool consistency from Type 1 (separate hard lumps) to Type 7 (liquid consistency with no solid pieces). The Bristol Stool Scale was administered to assess stool consistency at baseline (Day 0), follow-up visits (Days 3, 14, and 28), and the end of study visit (Day 56).
Immunoglobulin A (SIgA) levels were evaluated using Cusabio ELISA kits (Houston, TX, USA) and Human Beta-Defensin 2 levels were evaluated using ABclonal ELISA kits (Woburn, MA, USA) in the fecal samples. Tumour Necrosis Factor (TNF)-alpha and interleukin (IL)-6 were evaluated in serum samples using ABclonal ELISA kits (Woburn, MA, USA). Faecal SCFA’s - acetate, and propionate were evaluated using HPLC-UV detector and butyrate was evaluated using gas chromatography- flame ionization detection (GC-FID) method as per the lab protocols. For HPLC-UV, Hypersil ODS C18 4.6 x 250 x 5 columns were utilised, and SP2560 columns were used for GC. Injector temperatures were used as: Gradient Programme in HPLC and Split for GC. The sample injection volume was 20 µl.
Bacterial genomic DNA (gDNA) were extracted from faecal samples at baseline and Day 56 using Qiagen’s DNeasy Power Soil Pro kits. Library preparation and paired-end sequencing of 16SrRNA V3V4 amplicon were performed using (2 x 300bp configuration) by Biokart India Private Limited, Bengaluru, India. Sequencing data was de-multiplexed and adapter sequences were trimmed using Trimmomatic v0.39 [16].
The de-multiplexed and trimmed paired-end sequences were imported into QIIME2-2022.8 [17] and quality filtered using q2‐demux-paired. Sequences were then denoised, decluttered, and merged using q2-dada2 [18] to identify amplicon sequence variants (ASVs). Six base pairs were trimmed from 5’ end of forward reads, and eight base pairs were trimmed from 5’ end of reverse reads. Forward reads were truncated at 294 base pairs on the 3’ end, while reverse reads were truncated to 205bp on the 3’ end. 60-90% of all sequences passed filtration, and 40-70% of non-chimeric sequences were merged. Unique features (i.e., ASVs) were aligned with Multiple Alignment using Fast Fourier Transform (MAFFT) [19] using q2‐alignment and used to construct a phylogeny with FastTree2 [20] using q2‐phylogeny. Feature data was rarified to 8500 sequences per sample for alpha and beta diversity metrics [20–22] and Principal Coordinate Analysis (PCoA) estimated using q2‐diversity plugin. Taxonomy was assigned to ASVs using the q2‐feature‐classifier [23] and classify‐sklearn Naïve Bayes taxonomy classifier trained on the Silva 132 Operational Taxonomic Unit (OUT)s full-length reference sequences (Silva 132 Small subunit (SSU) Ref NR 99%). The relative abundance of ASVs classified at the phylum and genera-level was analyzed. Community composition (Bray Curtis, Jaccard, Unweighted and Weighted UniFrac) was assessed using distance matrices and an analysis of variance was individually determined for each β-diversity metric using ADONIS2 and 10,000X permutation analysis in the vegan package within R Studio V.4.2.0 (R Studio Software, Boston, Massachusetts, USA). The r2 and corresponding
P-values for each variable (e.g, Group, treatment) are shown above the graph of each beta-diversity metric. A ROUTs outlier (Q=1 criteria) test was applied to relative abundance data and alpha-diversity metrics and outliers were excluded prior to statistical analysis. Differences in alpha-diversity metrics and relative abundance of genera or next closest taxon were determined using non-parametric Kruskal–Wallis test for non-normally distributed data or Two-way ANOVA followed by Benjamini, Krieger and Yekutieli multiple comparisons post-hoc test with False Discovery Rate (FDR)-adjustment for parametric data, q< 0.05. Exact q values are indicated for notable trends.
The interactions were evaluated by the Paired t-test and Independent t-test using R software for the primary, secondary and tertiary efficacy endpoints. The criterion for significant test-by-treatment was p-value< 0.05. For categorical variables, a chi-square test was conducted. A value of p< 0.05 was considered statistically significant.
The continuous type safety endpoints were summarized by treatment using descriptive statistics (n [number of subjects], mean and percentage on safety population. The categorical type safety endpoints were summarized by treatment using frequency and percentage on safety population. The difference between the treatment groups with the supplements capsule and placebo was evaluated using the Pearson’s Chi-Square test or Fisher’s exact test.
A total of 90 subjects were screened for the study, and 30 failed the screening. Sixty subjects were enrolled in the study, and 55 of them completed the study (GE=29 and Placebo=26). Five subjects who could not complete the study were lost to follow-up (Figure 1)
The mean age of subjects enrolled in the GE group was 36.30±5.36 years, and BMI of 24.67±2.71 Kg/m2. Similarly, mean age of subjects enrolled in the Placebo group was 36.17±6.24 years, and BMI of 24.84±2.37 Kg/m2. Majority (95%) of the study population were males. The demographic characteristics are provided in Table 1.
A significant (p< 0.05) decrease in the PAC-SYM - Total score from baseline was recorded for the GE group on Days 28 and 56 as compared to placebo. Further, no significant differences were seen between the groups on Days 3 and 14 (Figure 2A).
A significant (p< 0.05) decrease in the PAC-QoL - Total score from baseline was recorded for the GE group on Days 28 and 56 as compared to placebo. No significant differences were seen between the groups on Day 14.
The Placebo group, as compared to GE group showed a significant (p< 0.05) difference in the PAC-QoL - Total score at Day 3. However, the decrease in Placebo group at Day 3 was not significant as compared to baseline
A significant (p< 0.05) improvement in the stool frequency was recorded from baseline for the GE group on Days 14, 28, and 56 as compared to placebo group. Further, no significant differences were seen between the groups on Day 3 (Figure 2C).
No significant differences were seen between the groups on Days 3, 14, 28, and 56. However, subjects in the GE group showed significant (p< 0.05) improvement in stool consistency from baseline at Days 14, 28, and 56, whereas subjects in the placebo group showed significant (p< 0.05) improvement from baseline only on Day 14 (Figure 2D).
A significant (p< 0.05) improvement in the SIgA levels in stool samples (mcg/g) was recorded on day 56 as compared to baseline for the GE group when compared against the placebo group (Figure 3A). Further, no significant difference was noted between the GE and placebo groups for HBD-2 levels in stool samples (ng/g) on Day 56 (Figure 3B).
No significant differences were noted between the groups in TNF-alpha (pg/mL) and IL-6 (pg/mL) levels on Day 56 (Figure 3 C&D).
No significant differences were reported between the groups in the SCFA: Acetate (mg/g), Propionate (mg/g) and Butyrate (mg/g) levels on Day 56 (Figure 3E).
Gut microbiome was assessed in faeces at baseline and Day 56 using 16S V3-V4 amplicon sequencing. GE or placebo supplementation did not alter richness or evenness based on Shannon or faith phylogenetic diversity metrics; however, both GE and placebo had increased evenness at endpoint as compared to baseline based on the peilou metric (Figure 4A), which suggested an even distribution in species abundances within gut microbiome by the end of the intervention. Community composition between groups was determined using Bray Curtis, Jaccard, Unweighted and Weighted UniFrac metrics and permutations analysis.
Overall community composition was not different between GE and placebo groups at baseline or after 56 days using any beta-diversity metrics (Figure 4B), which suggested that treatment matrix or time had the greatest impact on community composition. Taxonomic profiling of individual features, or ASVs, at the phyla (Figure 4C-D), and genera level (Figure 5) was assessed Compared to baseline, the post-supplement placebo group had increased relative abundances of Firmicutes which remain unchanged in GE group (Figure 4C). Both placebo and GE groups after 56 days of supplementation decreased relative abundances of Bacteroidetes, and increased Actinobacteria and Cyanobacteria (Figure 4C), and GE supplementation increased abundance of ASVs from the phyla, Patescibacteria (Figure 4C). Both GE and placebo supplementation increased F/B ratio at day 56; however, this increase was lesser in case of GE group as compared to placebo (Figure 4D). Further, both GE and placebo groups after 56 days of supplementation elevated faecal relative abundance of the genera Lactobacillus, Bifidobacterium, Subdoligranulum, Senegalismassilia, Acinetobacter, Blautia, Streptococcus, Slackia, and Ralstonia (Figure 5A).
GE group after 56 days of supplementation increased abundance of genera Weisella, Eubacterium coprostanoligenes, Enterococcus, and Pseudomonas as compared to placebo (Figure 5B). However relative abundance of Alloprevotella, Megasphaera, Dialister, Prevotella 9, Mitsuokella, and Bacteroides which was lowered post supplementation was comparable in both GE and placebo groups (Figure 5C). The pre-supplementation GE group had elevated relative abundance of Megamonas compared to all other groups (Figure 5D) and relative abundance of Catenibacterium was reduced in GE group only which was not seen in the placebo group (Figure 5D). Compared to the pre-supplementation placebo group, relative abundance of Sutterella and Prevotella 2 were lower in all other groups (Figure 5D). Further, Faecalibacterium abundance was higher in the pre-supplementation placebo group compared to post-supplementation GE and placebo groups, (Figure 5D) while Faecalibacterium abundance did not differ pre- or post-supplementation GE groups (Figure 5D). Additional data on relative abundance of microbiome which did not change significantly by GE supplementation is represented in Supplemental Figure 1.
No clinically significant changes were observed in the vitals, physical examination and laboratory assessments between the groups during the study period. During the course of the study, a total of 16 AEs were reported by 10 (16.67%) subjects, including 4 (13.33%) subjects from GE group who experienced 7 AEs and 6 (20%) subjects from placebo group who experienced 9 AEs. Most commonly occurring AEs experienced by >2% of the subjects included headache by 06 (10%), cold by 05 (8.33%) and diarrhea by 02 (3.33%). AEs reported were comparable in the two study groups. All the AEs reported by the subjects were mild in severity and the causality of the AEs was assessed by the Investigator as not related to the study products. The outcomes of all the AEs was noted as resolved before the end of the study. None of the subjects reported any SAE or was withdrawn from the study due to an AE or a SAE.
Overall 10 (16.67%) subjects used at least one concomitant medication during the course of the study for management of adverse events, of which 4 (13.33%) subjects were from GE group and 6 (20%) were from placebo group. Most commonly used medication included Paracetamol, Hifenac-P (Aceclofenac + Paracetamol combination) and Sinarest (Chlorpheniramine Maleate + Paracetamol + Phenylephrine combination). Overall, the safety and tolerability of GE was confirmed by the safety assessments in the study subjects.
Ginger is a widely used spice with a long history of use in traditional medicine for treatment of various gastrointestinal ailments like constipation, diarrhea, dyspepsia, bloating, indigestion, nausea, and vomiting. Scientifically demonstrated activities of ginger are mostly based on in vitro and in vivo studies and human clinical studies are available mainly in case of nausea and vomiting [8,9]. Here we report for the first-time utility of ginger to relieve symptoms of occasional constipation leading to the improved quality of life through a randomized double-blind placebo-controlled clinical study in human subjects with complaints of occasional constipation. We demonstrate that supplementation with GE for 8 weeks significantly improved symptoms of occasional constipation, stool frequency, along with improved QoL. We also observed that GE increased SIgA levels in the gut and modulated some components of the gut microbiome. Further, GE was found to be safe and well tolerated throughout the study period.
Occasional constipation is a widely prevalent functional disorder with infrequent stool and reduced bowel movements that affects QoL of subjects [24,25]. We used PAC-SYM questionnaire to assess abdominal, rectal and stool- related symptoms and severity of constipation over time [26–30]. We observed a significant (p< 0.05) decrease in the PAC-SYM - Total score in the GE group with improvements in symptoms of constipation and PAC-QoL by Days 28 and 56 and a significantly (p< 0.05) increased stool frequency as compared to placebo by as early as 14 days of GE supplementation. Subjects in the GE group alone showed significant improvements in stool consistency from baseline on days 14, 28, and 56, however, these changes were not significant as compared to the placebo group. Although no reported human clinical study data is available in the literature about the activity of ginger on constipation, experimental studies indicate that ginger enhances gastric emptying of charcoal meal in mice and rat models [31], promotes gastric and colonic motilities by enhancing laxative action and alleviating oxidative damage [32]. It is further reported that gingerols and shogaols from ginger have activity on muscarinic acetylcholine receptors and 5-HT serotonergic receptors that is responsible for increased gastric motility. It is also reported that activity of ginger on the 5-HT receptor ion channel complex by binding serotonin binding site is responsible for inhibition of cisplatin-induced delayed gastric emptying. Ginger also stimulates digestive processes and antral contractions in patients with functional dyspepsia [33] suggesting that active component of GE might exert an anti-constipation action possibly by increasing gastric motility [34].
SIgA helps with gut immune function by binding to certain pathogens and supports the intestinal epithelium and gut microbiome composition [35,36]. The significant increase in SIgA after consumption of GE for 56 days suggests an increase in gut immunity [37]. However, HBD-2 analysis did not show any significant improvements for the GE group as compared to placebo. Similarly, no significant difference between placebo and GE was observed for the inflammatory markers TNF-alpha and IL-6 as there was no baseline inflammation in the study subjects.The gut microbiome plays an important role in the maintenance of gut health and intestinal dysbiosis, and is known to be associated with gut-related health conditions such as constipation, irritable bowel disease, etc. [38,39]. Ginger modulates gut microbiota and ameliorates health conditions associated with obesity, cancer, inflammation, and gastric illnesses [9,40–46]. Bio-actives of ginger such as gingerols, shogaols, and paradols, have been shown to modulate gut microbiota metabolic activities, alter microbial composition, inhibit harmful microbiota, and modulate intestinal barrier functions [40,47].
We observed that GE supplementation is associated with selective increase in abundance of members from Patescibacteria which is known to be associated with HFD-induced bone loss in experimental animals [48]. The Firmicutes to Bacteroidetes (F/B) ratio is a marker of obesity in adults and children [49,50]. We observed an elevated F/B ratio post supplementation for both GE and placebo groups as compared to baseline, however this increase was significantly lesser in case of GE supplementation as compared to placebo, indicating that GE may have reduced obesogenic gut microbiome [49]. Compared to baseline, we observed a higher abundance of Firmicutes in placebo as compared to GE group indicating that GE supplementation may have inhibited growth of lipopolysaccharide-producing Firmicutes. However we have not seen any difference in the relative abundance of genera from this phylum (e.g, Bifidobacterium and Lactobacillus), suggesting there may be members from the Firmicutes phylum altered by GE that are rare or unidentified.
Interestingly, Sprague-Dawley rats supplemented with ginger extract for 30 days had decreased plasma lipids and lipopolysaccharide, which was associated with decreased cecal abundance of Bifidobacterium and Lactobacillus, and lower levels of Bacteroides and members from the Firmicutes phyla [51]. We also observed an increase in bacteria from the genera Subdoligranulum, Acinetobacter, Enterococcus, Pseudomonas, Slackia, and Blautia after GE supplementation which are usually detected in kefir, a probiotic drink, and may have a beneficial impact on human gut health [48]. An elevated Blautia is associated with decreased accumulation of visceral fat in adults. The relative abundance of Eubacterium coprostanoligenes group was increased in GE group as compared to placebo group on day 56; which is known to be modulated by gingerols in rats experimentally induced diabetic peripheral neuropathy [52], suggesting GE-induced increase in this genera is translatable and may be associated with metabolic improvements related to ginger. GE supplementation also elevated Weissella, a genera associated with antimicrobial and probiotic effects on inflammation and cancer [53], reduced levels of Megamonas, a genera with species found to be enriched in the gut microbial communities of non-alcoholic fatty lever disease patients [54]. Bacteria from the genera Prevotella and Catenibacterium were reported to have increased faecal levels in case of coronary artery disease in Tibetan highlanders of [55] were to found to be decreased by GE supplementation as compared to placebo. Collectively, a plethora of alterations in faecal microbial composition were observed in GE supplementation group that may promote beneficial phenotypes with anti-inflammatory properties. We also see that some of the dysregulated gut microbe population in subjects supplemented with GE is known to be associated with functional constipation. For example Patescibacteria which is upregulated in GE group is selectively upregulated in constipated mice model studies [56], Prevotella species that is down-regulated by GE is generally found to be up-regulated in functional constipation [57], butyrate-producing genera, such as Coprococcus, Roseburia and Faecalibacterium which are down-regulated in GE is generally found to be up-regulated in constipated patients [58,59] and finally modulated F/B ratio seen in case of constipation [60] is reversed in GE group. However, special care may be required while correlating data from published studies due to parameters such as cultural and demographical differences of the study cohorts diet habits and composition which could have profound impact on gut microbial composition and diversity, and therefore, health [61]. Controlling for variation in diet, computational and DNA extraction methods used between clinical trials are important considerations for gut microbiome analyses [62]. Using 16S does not provide enough resolution of changes in the gut microbiota and these data only really provide evidence to perform shotgun or metagenomic sequencing of the gut microbiome to better characterize which strains of bacteria are changing in response to GE supplementation. Also, additional clinical trials with larger number of study subjects and better sequencing strategies are needed to further characterize how ginger changes the gut microbiome, host-microbe interactions, and bioactive compounds to promote beneficial metabolic phenotypes.
Our study showed significant improvements by GE supplementation in occasional constipation as compared to placebo on symptoms of occasional constipation, stool frequency, quality of life, and SIgA levels. Further, GE supplementation also showed some alterations gut microbiome. No safety concerns were observed.
We thank the participants of the study
MME and JT contributed to the study conception and design. Study conduct, subject recruitment and data collection were performed at study centre by MME. Study was monitored in blinded fashion by LJ. Statistical analysis and study report were prepared by JT. Fecal microbiome samples were processed by VS in the lab and was analyzed and interpreted by KMT. Overall study data interpretation was done by MME and JT.
The first draft of the manuscript was written by MME, JT and KMT. All authors provided their inputs, read and approved the final manuscript.
The study was funded by OmniActive Health Technologies Limited (Mumbai, India)
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Committee approval for this study was obtained from BGS Global Institute of Medical Sciences Institutional Ethics Committee, Bengaluru, India. This study was conducted in compliance with the ethical principles originating in or derived from the Declaration of Helsinki and in compliance with the International Conference on Harmonization (ICH), Good Clinical Practice (GCP) Guidelines, as well as in strict compliance with the “The New Drugs and Clinical Trial Rules- 2019”, the Ministry of Health and the Government of India at all stages of the trial for adherence to protocol and compliance with ethical and regulatory guidelines. Voluntary consent was obtained in written from all the study participants before commencing any study related activities. The EC was duly apprised of the progress and updates of the trial at regular intervals as per prescribed guidelines.
The authors provide their consent for publishing this study results.
The authors declare that they have no competing interests.
http://ctri.nic.in/ Identifier: CTRI/2022/01/039843

![]()

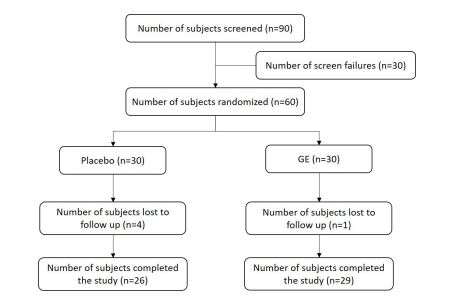 |
| Figure 1: CONSORT diagram of Ginger Extract (GE) clinical trial. |
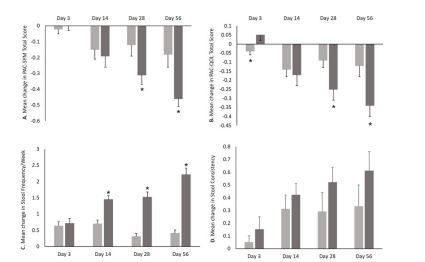 |
| Figure 2: Mean change - (A) Patient Assessment of Constipation Symptoms (PAC-SYM) - Total score; (B) Patient Assessment of Constipa- tion Quality of Life (PAC-QoL) - Total score; (C) Patient Assessment of Stool frequency/Week; (D) Patient Assessment of Bristol Stool Scale Scoring - Stool Consistency. GE - Ginger Extract. |
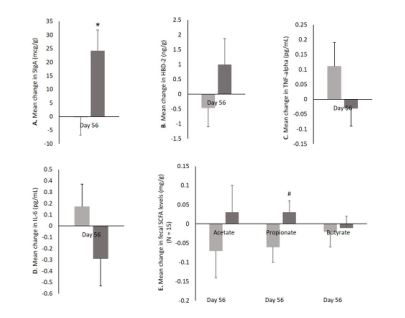 |
| Figure 3: Mean change - (A) Secretory Immunoglobulin A (SIgA) levels (mcg/g) and (B) Human Beta-Defensin 2 (HBD-2) (ng/g) levels in Stool Sample; Inflammatory marker: (C) TNF-alpha (pg/mL) and (D) IL-6 (Interleukin -6 (pg/mL) levels; and (E) SCFAs (Acetate, Propio- nate and Butyrate) (mg/g) levels. GE - Ginger Extract. |
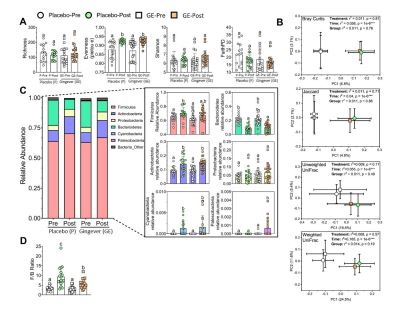 |
| Figure 4: Effect of GE and Placebo on gut microbial composition and diversity. (A) Microbial alpha-diversity of fecal microbial communities in humans fed placebo (n=20 per group; circles) or GE (n=22 per group; squares) for 12 weeks. (B) Beta diversity dissimilarity metrics (Bray Curtis, weighted UniFrac, unweighted UniFrac, and Jaccard) are shown as 2D-principal coordinate analysis (PCoA) plots with the centroid value standard error for each group. The r2 and p values for Supplementation groups (GE/placebo), time (Pre/Post) and overall group ef- fects are displayed on PCoA plots. (C) Relative abundance of ASVs classified by phyla (non-rarified data) after filtering out low abundance (< 0.0005) and low prevalence (< 50%). Different letters (a-c) indicate significant difference as determined by the non-parametric Kruskal-Wallis test for non-normally distributed data or Two-way ANOVA followed by Benjamini, Krieger and Yekutieli multiple compari- sons post-hoc test with FDR-adjustment for parametric data, q< 0.05. (D) F/B ratio: the post-supplementation GE group had a decreased F/B ratio relative to the post- supplementation placebo group. GE - Ginger Extract. |
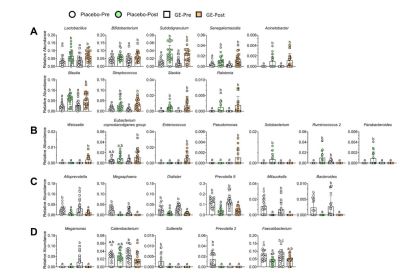 |
| Figure 5: Effect of GE and Placebo on prevalence of specific gut microbes in humans fed placebo (n=20 per group; circles) or GE (n=22 per group; squares) for 12 weeks. (A) Genera elevated in post- supplementation groups; (B) Genera elevated in post- supplementation GE or Placebo; (C) Genera decreased in post- supplementation groups; (D) Genera decreased in either post- supplementation GE or Placebo. Differ- ent letters (a-c) indicate significant difference as determined by the non-parametric Kruskal-Wallis test for non-normally distributed data or Two-way ANOVA followed by Benjamini, Krieger and Yekutieli multiple comparisons post-hoc test with FDR-adjustment for parametric da- ta, q<0.05. GE - Ginger Extract. |
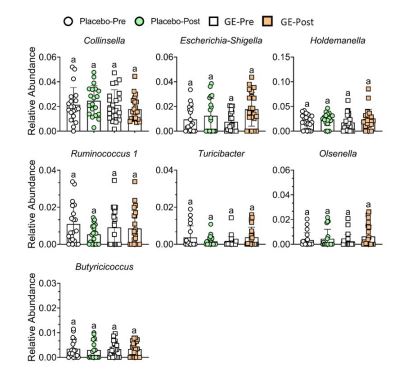 |
| Supplemental Figure 1: Bacterial families and genera unaffected by GE or Placebo in humans fed placebo (n=20 per group; circles) or GE (n=22 per group; squares) for 12 weeks. Relative abundance of ASVs classified by bacterial genera (non-rarified data) after filtration steps. For all panels, data are presented as mean SD. Similar letters indicate no significant difference as determined by the non-parametric Kruskal-Wallis test for non-normally distributed data or Two-way ANOVA followed by Benjamini, Krieger and Yekutieli multiple compari- sons post-hoc test with FDR-adjustment on parametric data, q< 0.05. GE - Ginger Extract |
Parameters |
Placebo (Mean ± SD) |
GE (Mean ± SD) |
N |
30 |
30 |
Age (years) |
36.17 ± 6.24 |
36.30 ± 5.36 |
Male [n (%)] |
29 (48%) |
28 (47%) |
Female [n (%)] |
1 (2%) |
2 (3%) |
2 |
24.84 ± 2.37 |
24.67 ± 2.71 |




































