Open Access
Research Article
Max Screen
ISSN: 2348-9812
Copyright: © 2021 Schloss RS. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Controlling osteoarthritic pain has emerged as a major health care challenge. Available treatments are either cytotoxic or addictive and therefore there is an urgent need to develop alternative treatment options. We previously developed a liposomal-alginate construct to improve local anesthetic delivery as a potential chronic pain management treatment. In order to further improve this construct, we have designed a PLGA-alginate construct which extends drug release for at least 35 days. The current studies describe the characterization of this construct and its effect on chondrocyte viability and function.
Keywords: Sustained Release; PLGA Nanoparticles; Chondrocyte Inflammation; Chondrocyte Hypertrophy
List of abbreviations: PLGA: Poly(Lactic-co-Glycolic Acid); LA: Local Anesthetic
Osteoarthritis (OA) is a disease that affects over 30 million people and it is estimated that 65 million Americans will be afflicted with OA by 2030 [1]. OA is a disease of the entire joint, affecting the cartilage, bone, and surrounding tissue [1]. It is characterized by pain and inflammation, specifically through increases of interleukin 8 (IL-8) and down regulation of proteoglycan deposition [2]. There are no cures for OA, and current treatments include Nonsteroidal anti-inflammatory drugs (NSAIDs) [3], steroids [4], and opioids [5], which all have negative long term side effects [6,7]. Therefore, there is a need for better pain mitigation that can be used in OA without negatively impacting cartilage viability or function.
Our alternative is to use sustained release local anesthetics (LA). LA have a history of safety and efficacy, with minimal side effects [8]. LA can be used to reversibly block sodium gated channels on nerves, thereby blocking pain signal transduction [8,9]. Common LA include bupivacaine, lidocaine, and ropivacaine, which are generally used for management of acute surgical and post-surgical pain [8,9]. However, despite their benefits, multiple studies have shown that LA can have detrimental effects on cell viability and function, including mesenchymal stromal cells [10], chondrocytes [11-14] and macrophages [15], in a dose and time dependent manner. In addition to their cytotoxic effects, LA have a short duration of use [16,17], making them impractical for use with chronic conditions such as OA.
A sustained release system, which delivers drug at predetermined intervals, would allow for LA use for chronic OA pain management. LA sustained release systems include liposomes [18,19], PLGA microspheres [20], injectable pastes [21], and hydrophobic polymers [22]. Thus far, Exparel® (liposomal bupivacaine) is the only FDA approved system for sustained release LA [18]. Exparel® consistently provides 24hr pain relief, but typically falls short of its 72hour target relief goal, and in the absence of repeated injections, is not sufficient for chronic OA pain. Our lab has engineered a hydrogel-liposomal bupivacaine system which consistently releases drug for 4 days [23-25]. However, while this release profile is longer lasting than available alternatives, it is still non-ideal for chronic pain management.
Poly(lactic-co-glycolic acid) spheres (PLGA) have been used for multiple drug delivery formulations. PLGA is biodegradable, biocompatible, and can be modified to fine tune delivery parameters [26,27], which may make them more adaptable than liposomes. In addition, PLGA particles tend to allow for longer release than liposomes [25,27], which would make them better alternatives for long term pain treatment. However, since these particles are nano in scale, additional modifications must be engineered to ensure positional control and site-specific drug delivery. Encapsulating the nanoparticles (NP) in alginate would ensure the drug is released at the site of injury while prolonging release at the same time. However, the effect of an engineered PLGA- alginate- LA system on chondrocytes is unknown, which is critically important before clinical translation of this pain management system for OA treatment can commence. The current studies were designed to develop an improved, longer release PLGA based LA delivery system which can be applied for OA pain management.
Bupivacaine loaded NP were formed using an water-oil-water sonication protocol, as explained in Wang et al. [27] and Nikitczuk et al. [28]. Particles were optimized using different concentrations of all parameters. The final NP formulation is described here. Briefly, 40mg of bupivacaine (Cayman Chemical, Ann Arbor, MI, USA) and 100mg of Resomer R 502H PLGA (50:50 MW 700-17000, acid terminated) (Sigma, St. Louis, MO, USA) was added to 0.4mL dichloromethane (DCM) (Sigma, St. Louis, MO, USA) and vortexed. The solution was added dropwise to 4mL of 1% poly-vinyl alcohol (PVA) (Sigma, St. Louis, MO, USA), and sonicated on a Branson digital sonicator (Model 450) (Branson, Danbury, CT, USA) for 3 cycles of 5sec on and 30sec off. The sample was added dropwise to 16mL of 0.1% PVA and placed on a rotovap for 2 hours, spinning continuously at 45 oC. It was then centrifuged at 15,000xg for 20min, washed with water, and spun down again and suspended in 2mL of 2% (w/v) sucrose. The particles were then lyophilized for 2days. Particles encapsulating Rhodamine B (Sigma, St. Louis, MO, USA) were made substituting 40mg Rhodamine B for 40mg bupivacaine and following the same procedure.
The size and zeta potential of the NP were measured using a Zetasizer Nano ZS (Malvern, Malvern UK). The concentration of drug within the NP was measured using HPLC (Waters Alliance 2695, Milford, MA). The HPLC mobile phase was 0.1% TFA: acetonitrile (21:79), with a sampling frequency of 1hz and a runtime of 10min. A Zorbax Eclipse Plus C18 (4.6x250mm, 5 μn) column was used. A 230nm wavelength was used with a 1.2nm band with Total flow was 1mL/min, with an internal temperature of 30±5 oC and an injection volume of 20uL. A standard curve was determined for free bupivacaine in the mobile phase. Encapsulation efficiency was determined by (starting mass-mass not encapsulated)/starting mass. Mass not encapsulated determined via HPLC of supernatant and washes. To determine drug diffusion out of the particle with and without the hydrogel, NP were placed in PBS. At each timepoint, the particles were spun down at 8000xg for 10 min and 1mL of PBS was removed and fresh PBS was replaced. Drug concentration at each time point was measured by mepivacaine ELISA (94% cross reactivity) (Creative Diagnostics, Shirley, NY).
Alginate encapsulation of NP was performed as previously described in Maguire et al. [25]. Briefly, 2.2wt% ultrapure alginic acid (MW: 100,000-200,000g/mol, G Content: 65%-70%, FMC Biopolymer AS, Sandvika Norway) was prepared using ultrapure water and stirring the solution at 65°C until fully dissolved. The solution was then filtered using a 0.22μm pore syringe filter (FisherBrand). Bupivacaine loaded NP were mixed, in various volumes based on the target drug concentration of 2.5mg/ml or 5mg/ml, with 2.2wt% alginate and deposited in Transwell inserts (Corning). The inserts were then submerged in a bath containing 100mM CaCl2, 145mM NaCl, and 10mM MOPS for 10 min. The hydrogels were then washed with phosphate buffer solution (PBS) for 10 min before being introduced to the cells. All liquid and viscous materials were sterilized via 0.22μm pore filtration (FisherBrand) and all solid materials were UV sterilization before being combined in a sterile environment to create the hydrogels.
The C28/I2 cell line (obtained from Dr. Mary Goldring, Hospital for Special Surgery, NY, NY) was chosen for our initial studies because this cell line is known to duplicate chondrocyte function and responses [2]. Cells were cultured as a monolayer at 50,000 cells/well in a 24 well plate in a humidified 37oC, 5% CO2 incubator. DMEM, supplemented with 10% fetal bovine serum (FBS) (Atlanta Biologicals, Flowery Branch, GA) and 2mM L-glutamine, was added to the cells. The cells were allowed to attach overnight. Fresh media, with or without stimulating cytokines (10ng/mL of TNF-α and IL-1α (R&D Systems, Minneapolis, MN, USA)), replaced the previous media. Transwell inserts (Corning) containing the different treatment conditions (media, bolus bupivacaine, bupivacaine-loaded NP, or alginate-NP construct) were added to the wells containing the chondrocytes and incubated for 24, 48, or 96 hours in the same conditions as described above (37oC, 5% CO2 incubator).
At the end of each time point, the supernatants were removed and saved for cytokine analysis (see Cytokine Measurement below). The cell culture supernatants were replaced with medium containing CellTiter-Blue Cell Viability Assay reagent (Promega) according to the manufacturer’s instructions. Viability can be assessed as the ability of viable cells to convert a dye to a fluorescent end product compared to a standard curve (R2=0.977) [29]. The cells were then returned to the incubator for continued culture. The fluorescence of the wells was read every hour up to 4 hours using a microplate reader (DTX880 Multimode Detector, Beckman Coulter), returning the cells to the incubator between readings.
Cell culture supernatants were thawed and tested for Interleukin 8 (IL-8) using an enzyme linked immunosorbent assay (ELISA, Biolegend, San Diego, CA). The assay was performed according to manufacturer's instructions and absorbance was read using a microplate reader (DTX880 Multimode Detector, Beckman Coulter, Brea, CA).
Following the viability assay, the cells were fixed with 4% paraformaldehyde (PFA) for 20 min and then diluted to 1% PFA using PBS for long term storage at 4 °C. Proteoglycan formation was analyzed using an alcian blue staining kit (ScienCell, Carlsbad, CA). The wells were washed with 0.1N HCl and then covered with alcian blue overnight at room temperature. The wells were then washed with ultrapure water 3 times prior to dye extraction using 6M guanidine HCl overnight at room temperature. The extracted dye was measured using a microplate reader (DTX880 Multimode Detector, Beckman Coulter) at 630nm. A standard curve of alcian blue values from 635 to 9.76μg/ml (R2=0.999) was used for quantification.
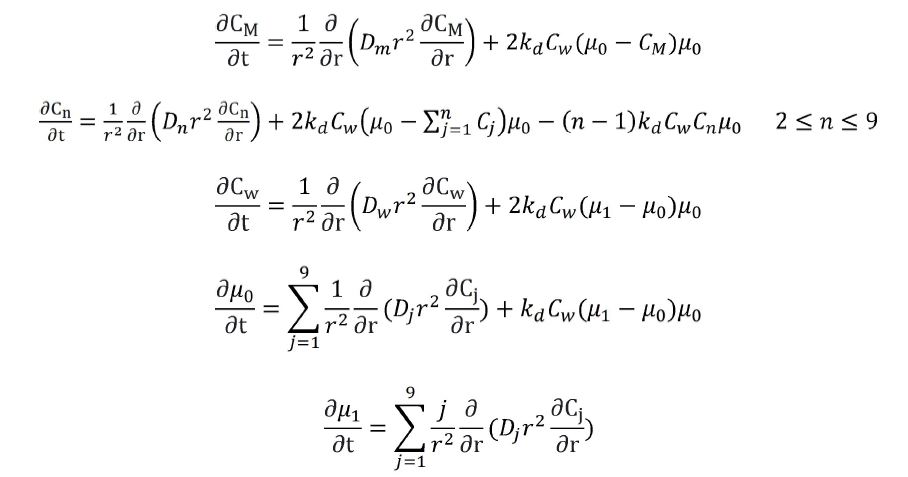
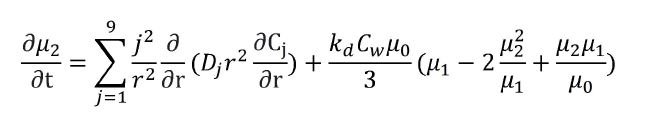
A mathematical model of bupivacaine diffusion from a PLGA NP was created, roughly based on Casalini et al. [30]. MATLAB R2020a was used to model the diffusion of bupivacaine out of the PLGA nanoparticle construct. Simulations were run with the assumption that the surrounding environment is constituted by a PBS solution (pH 7.4) at a temperature of 37 oC. The PLGA particles were modeled as a sphere assuming constant volume with radial variations in concentrations. This geometry was subject to bulk degradation as seen in physiological relevant conditions characterized by the acid-catalyzed hydrolysis mechanism. Polymer degradation of PLGA was modeled using mass conservation equations for varying polymeric chain sizes and water to create a set of partial differential equations which was described in detail elsewhere [30]. To reduce the complexity of expressing longer polymer chains of up to 104-106 monomeric units, the methods of statistical moment were used to represent this as a set of three differential equations. The zeroth order moment expresses the overall chains amount per unit volume. The first order moment represents the overall amount of monomeric units per unit volume. The second order moment describes polydispersity of the particle [30].
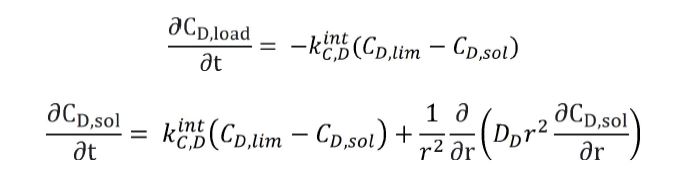
Drug release of bupivacaine from the construct was modeled using two mass balances for the loaded and dissolved drug based off of the Noyes-Whitney equation [30].
These two sets of equations were combined into a single system to describe the synergistic effects of degradation and diffusion. For each run, drug diffusivity of bupivacaine from the construct was determined empirically by fitting experimental data using the lsqnonlin algorithm in MATLAB for solving the nonlinear set of differential equations. A time step of one hour was used. To determine concentrations at any particular time point, the single system of differential equations was solved numerically using the ode15s algorithm implemented in MATLAB. These values were then converted to a percentage provided the amount of drug loaded at time t = 0. Percentage was then plotted as a function of time.
COMSOL Multiphysics 5a (COMSOL Inc. Burlington, MA, USA) was used to model the diffusion of bupivacaine out of the alginate engineered construct. The model was run using a 24 well geometry with a trasnwell insert for the construct. Fixed room temperature with a no-flux condition on all surfaces except the exchange between transwell and well. PBS was assumed to have a similar density to water, 1000kg/m3 and be an incompressible Newtonian fluid. Drug diffusivity within the PBS was assumed to be 1E-10mol/m3 [31]. A convention diffusion model with mesh optimization was performed to create an incompressible Navier-Stokes model. For each simulation, the construct was assumed to be one unit with NP and drug uniformly distributed within the alginate with a starting concentration of 1mM. A time step of one hour was used. Diffusivity of bupivacaine from the construct was determined by objectively fitting the models release profile to the in vitro data. To determine concentration, a point was chosen within the well and using COMSOLS built in 2D cross-section line plot, concentration was plotted as a function of time.
Statistical differences among data sets were determined using two-way analysis of variance (ANOVA) followed by Tukey's honestly significant difference (HSD) post hoc test. Significance level was α=0.05 in Prism 8 (GraphPad Software, San Diego, CA, USA). Data points represent the mean ± the standard error of the mean (SEM) for the indicated number of independent observations (n).
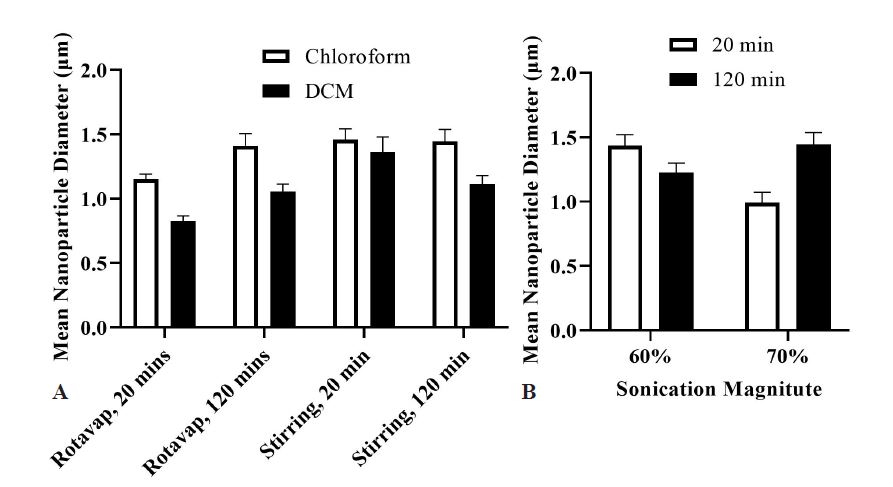
To create polymeric particles with the correct properties for this application, various parameters were analyzed to determine the correct compilation. Organic solvent, percent sonication, PVA concentration, and evaporation technique were all analyzed. DCM, a higher sonication, lower PVA concentrations, rotovap evaporation, and a shorter centrifugation time led to smaller particles (Figure 1). In addition, sonicator tip size also, altered the ultimate size of the particles. The final nanoparticle formulation used DCM as an organic solvent, 70% magnitude for sonication, 1% and 0.1% PVA, rotovap evaporation for 2 hours, and 20min centrifugation at 15,000xg, using the smaller sonicator tip (Branson Ultrasonics), which led to particles between 100-200nm. The size distribution is presented in Figure 1.
Following NP formulation, we characterized the size and drug encapsulation of our NP. We found that our particles were 121.52±14.7nm (Figure 2A), with a zeta potential of -22.4, and an average bupivacaine encapsulation efficiency of around 74.1±1.46% and an average loading capacity of 28.3±2.34%.
Our engineered construct is comprised of bupivacaine NP in an alginate hydrogel. To determine dispersion of the NP within alginate, Rhodamine-B loaded NP were encapsulated in alginate microbeads and imaged. The NP successfully mixed within the alginate hydrogel to ensure uniform dispersion (Figure 2B).
Bupivacaine diffusion out of the PLGA NP and the PLGA-Alginate Construct was analyzed over 35 days. As seen in Figure 3, 40% and 70% of the drug was released from the NP at 7 days and 35 days respectively. For the construct, only 4.5% and 16% were released at those time points. With the NP, there was an initial burst of 12% within the first day (Figure 3). The concentration of released LA at all time points is above the minimum serum levels necessary for effective analgesic effect [32].
Once the construct was characterized and the LA diffusion profile was determined, we wanted to understand the effect of the construct on chondrocyte viability and function. After 24hrs and 96hrs, Cell Titer blue was performed to determine overall cellular viability as a function of metabolic activity. Doses of 5mg/ml (0.5%), 2.5mg/ml (0.25%), and 1.25mg/ml (0.125%) were studied to mimic three common clinical doses of bupivacaine [14]. (These doses are significantly higher than the 1mM liposomal construct we have previously used). As seen in Figure 4 the bolus dose significantly decreases cell viability at 96hrs in both normal and inflammatory conditions. However, the construct improved viability to media levels in both conditions at all concentrations. 10% bolus was also analyzed to look at a control hypothetical LA dose that would be consistent with the cell exposure dose from the construct because previous modeling and diffusion studies of the construct indicate that only 10% of the LA is released at any given time point [24]. These bolus doses are 0.5mg/ml, 0.25mg/ml, and 0.125mg/ml for 5mg/ml, 2.5mg/ml, and 1.25mg/ml respectively. However, even at this lower LA concentration, the construct appears to protect viability whereas any concentration of LA above 0.125mg/ml (10% of 1.25mg/ml) appears to decrease viability in both normal and activated conditions.
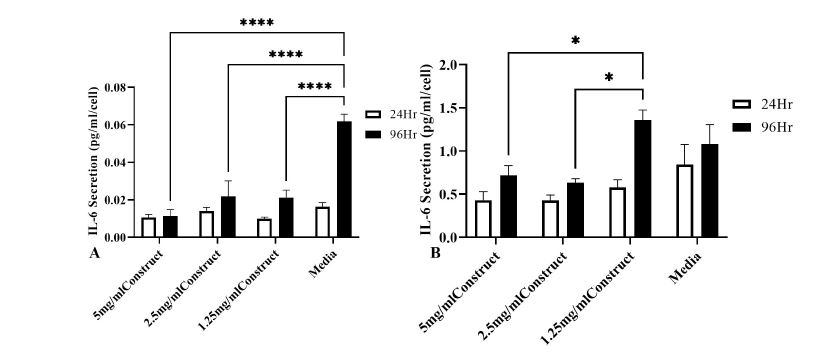
Cell function was analyzed as a measurement of two representative chondrocyte secreted products, IL-6 and IL-8. IL-6 is an inflammatory chemokine which has multiple functions in OA. For example, it has been shown to promote production of cartilage degrading matrix metalloproteases (MMPs) [33]. IL-8 is an inflammatory chemokine secreted by chondrocytes and is associated with promoting immune cell infiltration. Increased IL-8 is associated with later stage OA [2] and is therefore describes not only chondrocyte functional secretion properties but also increased local inflammation. Therefore, decreased IL-6 and IL-8 secretion may be consistent with a less inflammatory environment. As seen in Figure 5, in the presence of the construct, IL-6 secretions per cell remains below media controls except for 1.25mg/ml at 96hrs in activated conditions. The same trends are seen with IL-8. Only the 1.25mg/ml construct at 96hours has higher IL-8 secretions compared to media controls.
Collagenase was measured to determine chondrocyte degeneration in the presence of the construct. As seen in Figure 6A, the construct did not change collagenase activity. Proteoglycan deposition was also measured to determine chondrocyte regenerative potential in the presence of the construct. Alcian blue assay was used to stain the GAG produced in the various conditions in the presence of different LA modalities. As seen in Figure 6B, the construct does not impair proteoglycan deposition. The construct increases the concentration of GAG production at lower LA doses compared to media controls in both non-stimulated and stimulated conditions.
In addition to ensuring that the construct did not reduce viability, modify inflammatory secretions, or negatively impact degeneration or regeneration, it is important to know whether the construct promotes a hypertrophic cellular environment. Alkaline phosphatase (ALP) activity is a strong indicator of chondrocyte hypertrophy [34,35]. As seen in Figure 7, ALP activity per cell is not increased compared to media controls. In fact, ALP activity is decreased in most cases, especially at lower LA doses.
These formulated nanoparticles enabled cellular function and viability to be retained. Based on the diffusion data, the NP and construct allow for use for a minimum 35 days if the starting conditions remained unchanged. However, being able to design our NP and construct with different starting conditions would be valuable for condition specific treatment design. While our diffusion data reflects clinically effective levels of LA at all time points in vitro, a higher or lower starting dose may be necessary for in vivo applications. In order to understand how changing parameters would affect diffusion, the nanoparticle and construct diffusion was modeled with MATLAB and COMSOL Multiphysics, respectively. Using the in vitro diffusion release data (Figure 3), the diffusivity from the nanoparticle and the construct could be determined. For the nanoparticle, MATLAB determined the diffusivity to be 2.23E-16 cm2/s. For the construct, COMSOL Multiphysics determined the diffusivity to be 4.7E-13 cm2/s. Diffusivities were determined by minimizing sum of squares between the modeled and in vitro data. The discrepancy between the diffusivities is due to the material properties and the size of the carrier. The NP is much smaller than the construct and therefore, its diffusivity is smaller than the constructs diffusivity. Geometry of the system plays an integral role in diffusivity calculations. As seen in Figure 8, the diffusion profiles for the NP and construct showed 40% release in 7 days and 16% release in 35 days respectively.
By changing the starting parameters, such as the starting concentration or the geometry of the construct, the diffusivity and diffusion profile changes. For instance, changing the geometry of the well changes the diffusion parameters of the model. Therefore, mathematical modelling will allow for more robust NP and construct design as needed.
Chronic inflammatory conditions, such as OA, are difficult to treat effectively without adverse side effects. Our approach of using LA to combat the pain associated with OA would allow for pain mitigation without cytotoxicity or unwarranted responses.However due to the short half-life of LA, a sustained release system is necessary for use in chronic conditions. Sustained release biomaterials loaded with bupivacaine are able to release clinically relevant levels of LA, however they are designed for post-surgical applications and are unsuitable for chronic conditions [36]. Other formulations are limited in injection volume [25] or duration of use [37]. Our engineered construct not only prolongs release further than anything currently on the market, but also allows for positional control at the site of injury so that the drug is constrained to the localized area.
PLGA LA particles allowed for release for 7 days, with only 40% of the drug released. The initial burst of drug from the NP solution may be drug conjugated to the particles or may be free drug not adequately separated from the NP. However, a burst response in the beginning may be beneficial in minimizing pain quickly and after 24 hours, when the pain has been successfully managed, the slow release would help continue the pain mitigation with lower continuous LA. The engineered construct also allows for the drug initial burst; however, it slows down the overall drug release. By five weeks, only 16% of the drug has been released (Figure 8). The PLGA system is an improvement over the liposome system previously engineered because it allows for longer sustained release while maintaining uniform NP dispersion within the alginate and positional control at the site of injection. Diffusion models of the NP and construct recapitulated these findings while allowing for changes to be modeled as well (Figure 8). The models are specific to the original assumptions, geometries, and starting parameters, but with modifications, different scenarios are possible and can be simulated before any in vitro work is completed. Additional components, such as cell uptake, can be incorporated to allow for a more complex and realistic model.
The concentrations of drug used are consistent with typical clinical values. Our engineered construct allows for tailoring the drug concentration easily. When chondrocytes were dosed with the sustained release drug, viability remained as high as media controls. Using the engineered construct improved viability over bolus or 10% bolus conditions (Figure 4). The construct helped decrease ALP activity while maintaining proteoglycan deposition (Figure 7). ALP activity is a good indicator for hypertrophy. Therefore, decreasing inflammation and ALP activity indicates a less hypertrophic environment. In our case, all constructs reduced ALP activity compared to media controls. This is likely due to the decreased inflammation, however, LA have also been shown to reduce ALP activity in other cell types, such as bone [38,39]. The construct also kept IL-6 and IL-8 comparable to media controls (Figure 5), which could be beneficial in OA. These findings are consistent with research that shows that LA can downregulate inflammatory cytokine and chemokine secretion, including IL-8, while upregulating the release of IL1-RA which has been shown to reduce inflammation [40-43]. We recognize that some of the conditions did increase the levels of these cytokines, specifically at the lower doses. However, this construct on its own was not designed to decrease inflammation to levels sufficient to mitigate the effects of OA. We aimed to optimize LA doses without causing extraneous side-effects, and this was achieved at most doses tested. The novelty of our system is that, an anti-inflammatory (non-steroidal or steroidal) sustained release medication [44], or even perhaps mesenchymal stem cells [23,24,45], could also be encapsulated and included into this LA construct.
Our studies indicate that a sustained release LA system can be used in conjunction with chondrocytes without negatively impacting their cellular viability or function. Moreover, this engineered construct allows for clinically relevant drug release for a minimum of 5 weeks, significantly longer than anything on the market. Overall, the bupivacaine PLGA NP alginate construct can help neutralize one of the main symptoms of OA, pain, while allowing for inflammation reduction and regeneration of cartilage.
We would like to thank Dr. Mary Goldring (Hospital for Special Surgery, NY, NY) for providing the C28/I2 cells. We would also like to thank Elisheva Strauss for her work with the PLGA nanoparticle formulation. We would like to thank Dr. Tommaso Casalini for his help in recreation of the MATLAB model for drug diffusion study. Research reported in this manuscript was supported by the National Institute of General Medical Sciences of the National Institute of Health under award number T32.

![]()

 |
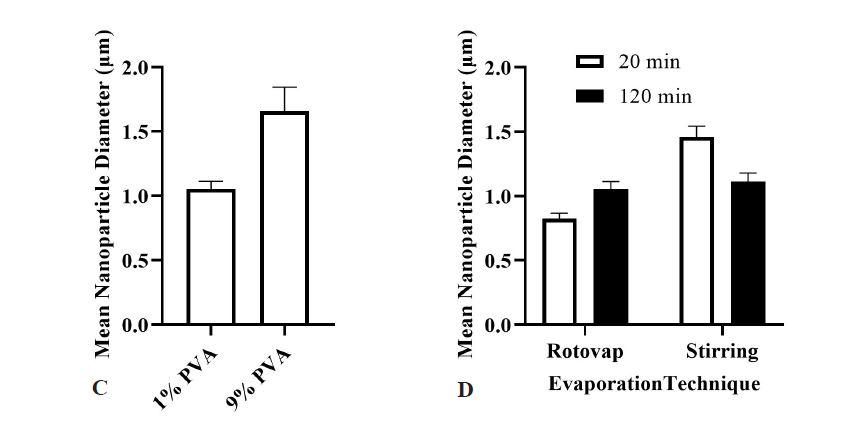 |
| Figure 1: Formulation Parameters for Nanoparticles. Various parameters were analyzed to determine optimal nanoparticle size (A) Organic Solvent. Chloroform or dichloromethane; (B) % Magnitude for Sonication. 60% vs 70%; (C) PVA concentration. 9% vs 1% and 0.1%; (D) Evaporation method and centrifugation time. 2hr Rotovap vs 5hr Stirring. 20min centrifugation 15000xg vs 120min centrifugation 15000xg. All other parameters held constant for comparisons. The data is the mean ± SEM of n=15-50 independent observations |
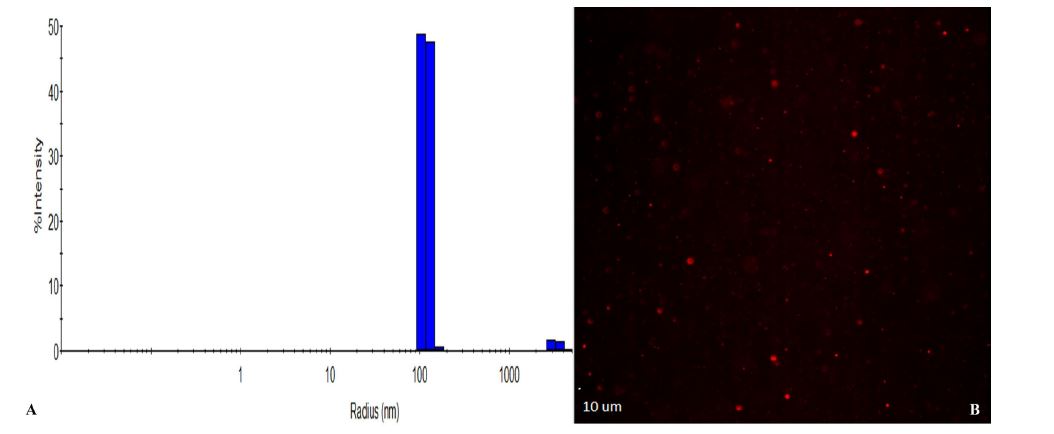 |
| Figure 2: Nanoparticle size and dispersion (A) DLS histogram of nanoparticle size distribution of 10 nanoparticle batches; (B) Rhodamin B PLGA nanoparticles are homogeneously dispersed within the alginate hydrogel |
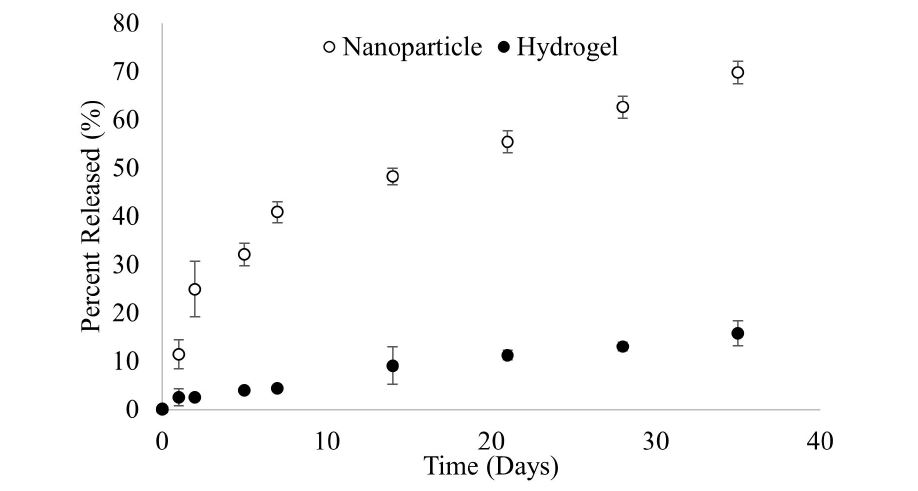 |
| Figure 3: LA diffusion from PLGA NP and Construct. Cumulative release of drug from the PLGA NP and Construct as measured by ELISA. Mean ± SEM of n=6 |
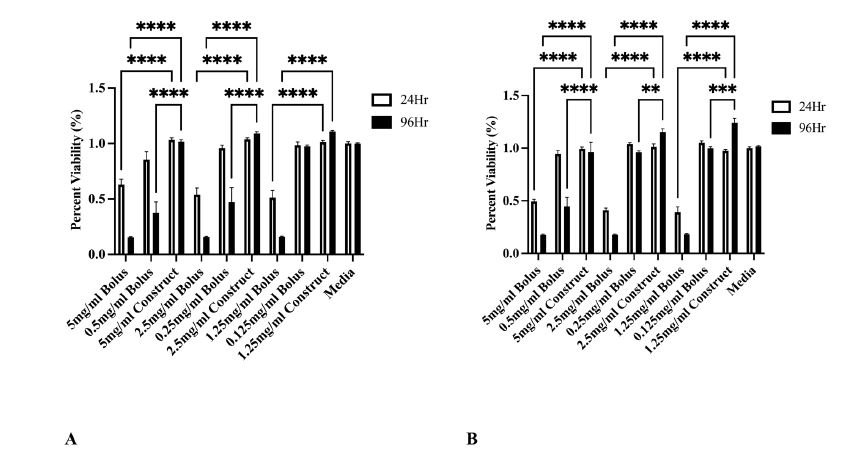 |
| Figure 4: C28I2 viability in the presence of LA. The bar heights represent the fluorescence intensities (FI) of reduced CellTiter-Blue reagent (A) Non-stimulated media and; (B) inflammatory media stimulated with 10ng/mL of TNF-α and IL-1α. The data is the mean ± SEM of n=9-12 independent observations. *p≤0.05, ** p≤0.01, *** p≤0.001, **** p≤0.0001 |
 |
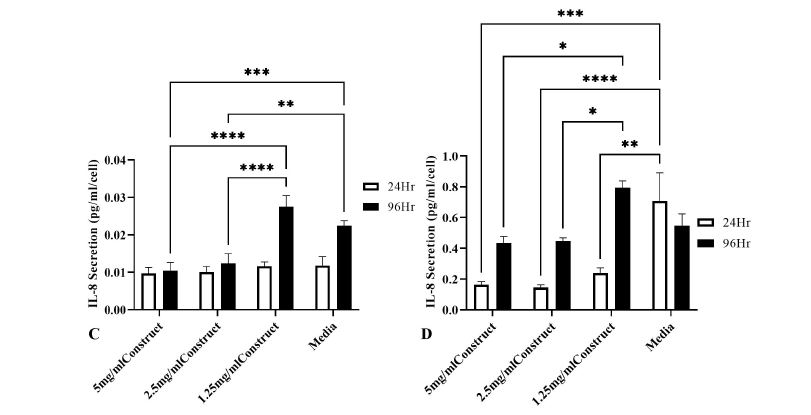 |
| Figure 5: C28/I2 IL-6 and IL-8 Secretion in the presence of the Construct. The bar heights represent Il-6 and IL-8 secretion concentrations per cell quantified from cell supernatants treated with 5mg/ml, 2.5mg/ml, 1.25mg/ml, or 0mg/ml media controls (A) and (C) non-stimulated media and; (B) and (D) stimulated media containing 10ng/ml of TNF-α and IL-1α. The data is the mean ± SEM of n=9-12 independent observations. *p≤0.05, ** p≤0.01, *** p≤0.001, **** p≤0.0001 |
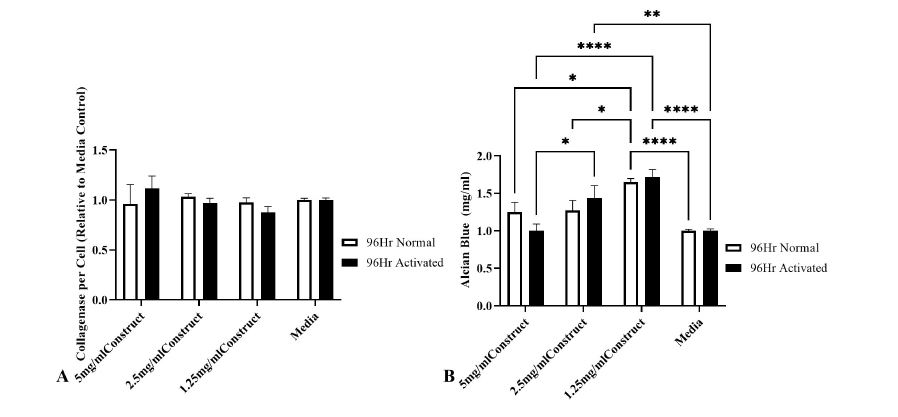 |
| Figure 6: C28/I2 collagenase and proteoglycan deposition are not negatively impacted by Construct. Bar heights represent (A) collagenase activity relative to media controls and; (B) alcian blue quantified from ECM deposits. Cells treated with 5mg/ml, 2.5mg/ml, 1.25mg/ml, or 0mg/ml media controls. Non-stimulated or stimulated media containing 10ng/ml of TNF-α and IL-1α. The data is the mean ± SEM of n=9-12 independent observations. *p≤0.05, ** p≤0.01, *** p≤0.001, **** p≤0.0001 |
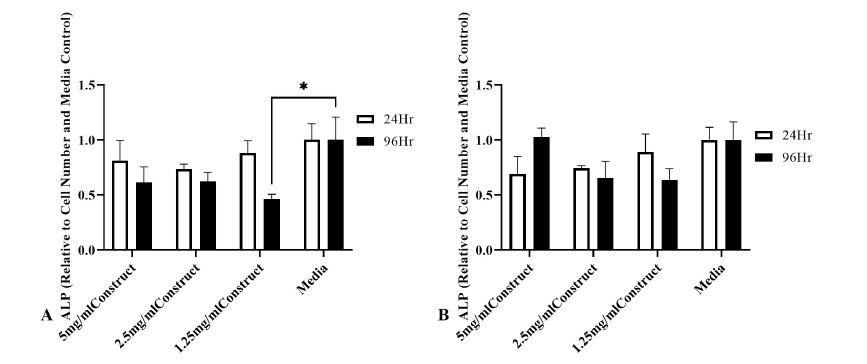 |
| Figure 7: ALP activity is not increased in the presence of the construct. Bar heights represent ALP activity for C28/I2 treated with constructs containing 5mg/ml, 2.5mg/ml, 1.25mg/ml, or 0mg/ml media controls (A) non-stimulated media and; (B) stimulated media containing 10ng/ml of TNF-α and IL-1α. The data is the mean ± SEM of n=4-6 independent observations. *p≤0.05, ** p≤0.01, *** p≤0.001, **** p≤0.0001 |
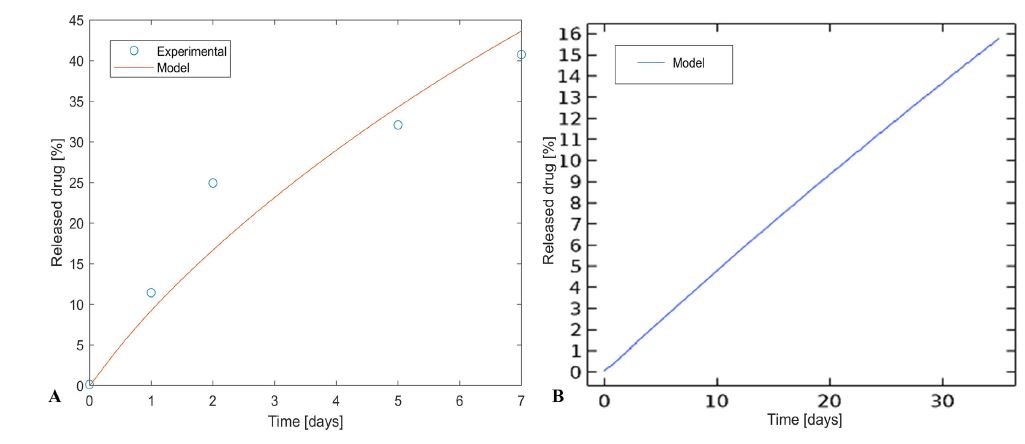 |
| Figure 8: Diffusion Models (A) MATLAB model if bupivacaine release from PLGA NP. Using experimental diffusion data for 7 days, the drug release was modeled for 7 days. 40% is released in 7 days; (B) COMSOL model of bupivacaine release from construct. Using experimental data for 35 days, the drug release was modeled for 35 days. 16% is released in 35 days |
r |
radius of particle |
Cm |
concentration of monomer |
Cn |
concentration of oligomer of chain length n |
Cw |
concentration of water |
μ0 |
zeroth order statistical moment |
μ1 |
first order statistical moment |
μ2 |
second order statistical moment |
CD,load |
molar concentration of loaded drug |
CD,sol |
molar concentration of solubilized drug |
CD,lim |
drug solubilization limit |
Dn |
diffusion coefficient for oligomer of chain length n |
Dm |
diffusion coefficient for monomer |
Dw |
diffusion coefficient of water |
kd |
degradation kinetic constant |
Dd |
diffusion coefficient of active ingredient in devicet |
kC,D |
mass transfer coefficient |




































