Open Access
Research Article
Max Screen
Copyright: © 2019 Amrit Thapa. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Distraction Osteogenesis (DO) is an established method for correction of developmental anomaly of the facial skeleton. The early beginning of urgent surgical corrections are allowed in smaller age as even small children suffering from bilateral severe mandibular deficiency who are often associated with breathing and swallowing disorder caused by glossoptosis. Till date conventional radiographs and computed tomography were the preferred diagnostic modalities to monitor the distraction osteogenesis regenerate. But these techniques do not detect the ongoing osteogenic process; moreover they obligate the patient to serial radiation exposures which have a cumulative hazardous effect. In addition, virtual findings were obscure due to anatomic overlap and metal artifacts. Comparatively, ultrasound is a noninvasive, efficient and an inexpensive way to evaluate bone healing. This case report was presented to test the efficacy of USG (Ultrasonography) in evaluating bone healing at mandibular distraction sites for estimation of bone formation, using a radiological and ultrasonographic bone fill scoring method and successful management of OSA (Obstructive sleep apnoea) patients with planned DO.
Keywords: Distraction Osteogenesis; Obstructive Sleep Apnoea; Ultrasonography; Polysomnography
Severe mandibular hypoplasia sometime associated with significant morbidity and mortality in infants and children due to compromised upper airway space airway. They may exhibit frequent episodes of oxygen desaturation, hypoxemia, hypercarbia, acidosis, persistent inspiratory stridor, severe sternal retraction, and poor feeding (secondary to airway compromise). Children with long-term airway obstruction exhibit failure to thrive, daytime sleepiness, hemodynamic derangements, developmental disabilities, malnutrition, increased pulmonary morbidity, and death [1].
There are various treatment modalities for the management of severe mandibular retrognathic case is associated with OSA i.e, Distraction Osteogenesis, BSSRO and Le Forte I osteotomy. For this particular case, DO was chosen due to severity of malocclusion and overjet was more than 7mm. DO is a process of new bone formation between the surfaces of bone segments gradually separated by incremental traction [2]. Distraction protocol principles and guidelines are mainly based on the studies and clinical trials of Dr. Ilizarov [3]. Presently no fixed protocol exists for the assessment of the distraction regenerate, which could aid in modifying the distraction protocol according to the needs of each patient. USG promises to give an accurate assessment of not only the mandibular regenerate, but also the surrounding soft tissues.
Correct assessment of the wound during the distraction phase and neutral fixation phase is important to document the progress of bone lengthening, assure stability of the device, and determine the degree of bone formation in the distraction gap and the optimal timing for device removal which is still a debatable issue amongst clinicians [4]. To assess the mandibular distraction wound healing various procedure followed that include clinical examination, plain radiography, computed tomography (CT) and Dual Energy X-ray Absorptiometry (DEXA). Serial radiographs and CT examination increase unnecessary radiation exposure to the patients.
In addition, standard radiographic imaging poorly defines the regenerate as compared to the high accuracy of USG. It has been observed that the presence of bone union on radiographs is difficult to evaluate and not reliable during the first 4 weeks of fixation [5]. Numerous superimpositions in the postero-anterior (PA) view and panoramic radiographs of the skull have a limited application in patients with a distraction device in situ [6].
Comparatively, USG is an inexpensive and effective method which provides in depth assessment of bone formation across a defect during early period [6-10]. Normal mature bone assessment via USG is limited by the inability of the ultrasound beam to penetrate the outer cortex, however newly formed bone, which is not completely remodeled and calcified, can be well evaluated with highresolution linear ultrasound [11]. This phenomenon allows the surgeon or radiologist to evaluate the quantity and distribution of the regenerate. Thus USG has minimal expense, lack of metal artifact, lack of the need for sedation for uncooperative young patient and lack of radiation exposure makes this a powerful tool for the assessment of bone healing. The purpose of this case report was to demonstrate the efficacy of Ultrasonography as an assessment tool in comparison with radiographic and clinical examination in the evaluation of the mandibular distraction osteogenesis regenerate secondary to obstructive sleep apnoea.
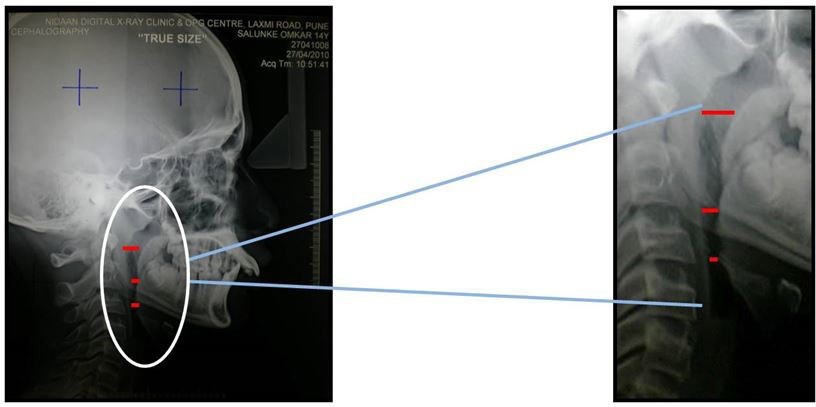
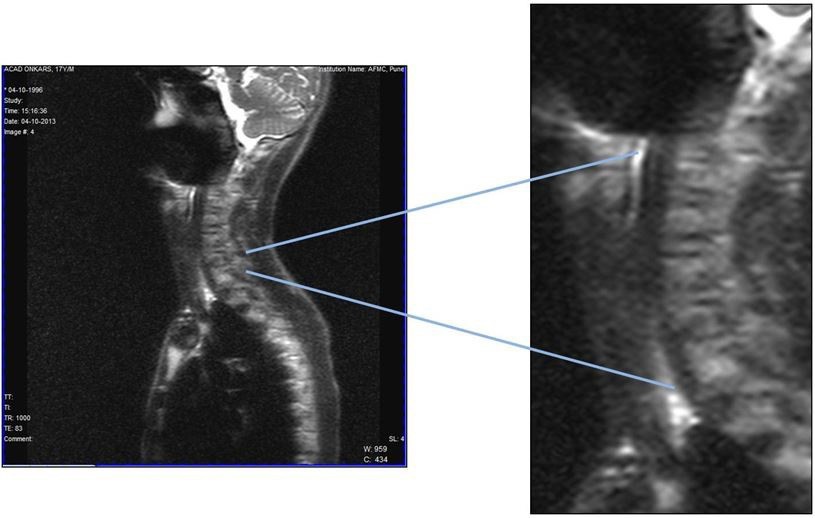
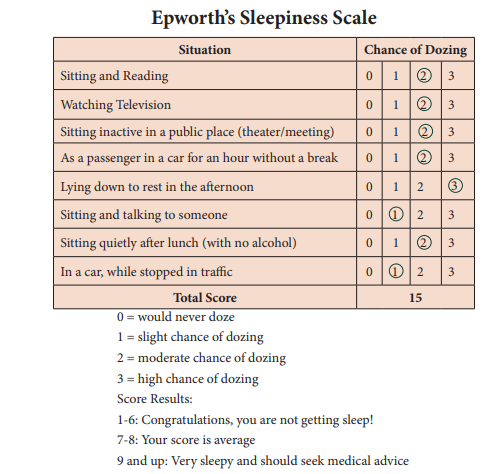
17 year-old adolescent male reported with the chief complaint of backwardly placed lower front teeth. Medical history was not significant. Temporomandibular joint examination revealed no significant anomaly. On evaluation of facial photographs, it was elicited that he had convex facial profile, normal nasolabial angle with potentially noncompetent lips, nonconsonant smile, deep mentolabial sulcus, and reduced lower anterior facial height. The intraoral photographs and dental casts revealed ovoid arches, coinciding dental and facial midline, overjet of 11 mm, molar and canine relation class II bilaterally, spaces in upper and lower anteriors and an impinging bite (Figure 1). The cephalometric analysis revealed a class II jaw-base relationship; an ANB angle of 60, orthognathic maxilla (Co-A, 84 mm), retrognathic mandible (Co-Gn, 98mm [105–108 mm]), and mandibular plane angle of 210, panoramic radiograph depicted no obvious bony pathology (Figure 2). All third molars were in different stages of development. Thorough case history and clinical examination of patient were performed. MRI, Lateral cephalogram and subjective scale i,e. Epworth sleepiness scale of 15 was associated with patient which indicate association with OSA (Figure 3 and 4) (Table 1). Polysomnography (PSG) were also done to ascertain whether patient having Apnoea Hypopnoea episode, which indicate patient having mild OSA (Table 2). The primary problem was mandibular retrognathism with overjet of more than 7mm so he was taken up for surgical mandibular advancement using DO.
Both arches were well-aligned and there was negligible transverse discrepancy therefore orthosurgical approach was planned to achieve desired objectives. The treatment objectives were improvement of profile, improvement of smile, correction of molar and canine relationship, correction of skeleton relationship, and finishing and retention [1-5].
To achieve desired objectives 2 treatment alternatives were proposed to the patient:
1. Conventional BSSRO orthognathic approach: This approach had a disadvantage for this case as patient having overjet of more than 7mm which can cause relapse afterwards.
2. Distraction Osteogenesis: This approach was considered because overjet of 11 mm was present which destabilizes the overall result if BSSRO was done.
The main goals of the orthodontic-surgical treatment were to promote mandibular advancement for correction of the dental and skeletal base correction. Before surgical correction, presurgical orthodontic preparation was done to correct the dental disharmonies. Leveling and alignment of the arch with simultaneous dental expansion for transverse correction was planned with simultaneous closure of anterior upper and lower spaces. After dental corrections, distractions osteogenesis was planned by advancement of the mandible by 11mm.
Bonded 0.018” Roth pre adjusted edgewise appliance was placed along with banding upper and lower 1st and 2nd molar. To prevent the lingual roll-in of lower molars, upper expanded transpalatal arch for transverse correction and lower 0.036” mandibular lingual arch was given (Figure 5). Archwire sequence followed for the treatment were:- Upper, 0.016 nickel-titanium (NiTi), 0.016 ss, 0.018 x 0.018 NiTi, 0.017 x 0.025 ss, 0.016 ss (postsurgical); lower, 0.014 NiTi, 0.016 NiTi, 0.018 x 0.018 NiTi, 0.017 x 0.025 ss, 0.016 ss (postsurgical). Anterior upper and lower spacing was relieved with use of Elastic traction. Presurgical preparation was completed in upper and lower arch followed by placement of 0.017 x 0.025 ss archwires that remained in place for 3 months before surgery. The teeth of the lower arch were positioned more favorably (labiolingually, buccolingually) to their apical base. During presurgical phase, proper model analysis and vector planning was done (Figure 6). On completion of presurgical orthodontics, lateral cephalogram and orthopantogram was taken that showed almost root parallism and no abnormal root resorption. Distraction osteogenesis was planned keeping in view that the skeletal Class II was due to a combination of orthognathic maxilla and small mandible with overjet of 11mm. After presurgical phase, the surgical procedure included complete osteotomy of mandible was carried out followed by placement of distractor parallel to maxillary occlusal plane (Figure 7). After five days of latency period, activation of distractor was done till achieved edge to edge bite. Distractor was open every day bilaterally with 1mm opening. Callus molding was done afterwards before completion of consolidation phase in order to close the posterior open bite based on the “floating bone concept”. During postsurgical phase, periodically USG (Ultrasonography) was taken at the interval of 1st month, 2nd month, 3rd month and 16 weeks stage at which analysis was done by seeing USG which showed semiquantative score of 3 after twelve weeks (Figure 8) [12]. 12 weeks after surgery, distractor was removed based on UGS analysis. Afterwards, Upper 0.016 x 0.022 ss and lower 0.016 ss were used for finishing and detailing. Intermaxillary elastics were used to settle the occlusion. After the active treatment phase, intraoral photographs shows class I molar and canine relation bilaterally with optimum over jet and overbite (Figure 9).
OSA generally associated with patients having retrognathic maxilla or mandible compromising upper airway space. There are several surgical treatment modalities for the treatment of severe class II div I malocclusion secondarily associated with OSA. Laser assisted uvulopalatoplasty (LAUP), uvulopalatopharyngoplasty (UPPP), hyoid suspension, tongue base reduction, genioglossus advancement and maxillomandibular advancement are the most preferred procedures that aim to enlarge airway dimensions and decrease airway collapsibility [13].
In recent years, DO have become popular and reliable methods for the correction of craniomaxillomandibular deformities compromising the airway space. Advancements of 25 mm or more without a bone graft and the associated donor site morbidity, scarring, and potential for infection can be achieved with the help of DO. Soft tissue seems to grow linearly along lines of tension, and skin, muscles, nerves, and vascular tissue are generated with less soft tissue resistance by a process of distraction histogenesis. The primary purpose of distraction osteogenesis compared to conventional orthognathic approach is to achieve stable occlusion having overjet more than 6mm and with minimal relapse. This procedure permits skeletal correction and help in establishing good intercuspation postsurgery. This procedure is time consuming but has significant effect on patient esthetics, stability and ultimately patient psychology [14]. In this case report, patient with facial asymmetry due to mandibular deficiencies, requiring at an average greater than 6 mm of movement of the mandible, were treated by DO. Patient was found to be associated with OSA with severe mandibular hypoplasia with increase overjet and overbite which was associated with compromising upper airway space as noticed during orthodontic review chair side. Complete history was taken including Polysomnography which shows patient fall under mild OSA group with AHI (Apnoeic hypopnoeic index) of 14. The high success rate of MMA has been established and oral and maxillofacial surgeons are now involved more frequently and at an earlier stage in the treatment of OSA [15-18]. After corroborating clinical and radiological findings, case was planned for distraction osteogenesis for more predictable and stable result which can be seen in post surgical photographs and after comparing between pre and post cephalometric values after debonding (Table 3) [19].
In recent years, DO have become popular and reliable methods for the correction of craniomaxillomandibular deformities compromising the airway space. Advancements of 25 mm or more without a bone graft and the associated donor site morbidity, scarring, and potential for infection can be achieved with the help of DO. Soft tissue seems to grow linearly along lines of tension, and skin, muscles, nerves, and vascular tissue are generated with less soft tissue resistance by a process of distraction histogenesis. The primary purpose of distraction osteogenesis compared to conventional orthognathic approach is to achieve stable occlusion having overjet more than 6mm and with minimal relapse. This procedure permits skeletal correction and help in establishing good intercuspation postsurgery. This procedure is time consuming but has significant effect on patient esthetics, stability and ultimately patient psychology [14]. In this case report, patient with facial asymmetry due to mandibular deficiencies, requiring at an average greater than 6 mm of movement of the mandible, were treated by DO. Patient was found to be associated with OSA with severe mandibular hypoplasia with increase overjet and overbite which was associated with compromising upper airway space as noticed during orthodontic review chair side. Complete history was taken including Polysomnography which shows patient fall under mild OSA group with AHI (Apnoeic hypopnoeic index) of 14. The high success rate of MMA has been established and oral and maxillofacial surgeons are now involved more frequently and at an earlier stage in the treatment of OSA [15-18]. After corroborating clinical and radiological findings, case was planned for distraction osteogenesis for more predictable and stable result which can be seen in post surgical photographs and after comparing between pre and post cephalometric values after debonding (Table 3) [19].
In this case report, the pattern of the regenerate also being observed after latency period of 4–7 days, at the site in which the distraction was performed at the interval of 1 month, 2 month and 12 weeks. No difficulty was observed in the initiation of the distraction process, and satisfactory bone formation was observed in this case, as seen in USG prior to distractor removal. Based on the principles of Ilizarov, a daily distraction rate of 1.0 mm in two increments daily was followed in the present case report till we have achieved edge to edge bite [20]. In post surgical phase, PSG was done which shows AHI (apnoeic hypopnoeic index) reduced to normal i, e. 4 with no episode of snoring during night (Table 4). ESS (Epworth sleepiness scale) score also reduced to 6 from 12 which shows improve subjective score.
Arriving at the endpoint of distraction is an important part of DO. Evaluation of quantity and quality of regenerate is one of the cornerstones of this treatment modality. Common methods of assessment of the regenerate consist of serial physical examinations, lateral radiographs, DEXA, and CT [5,7-9]. Evidence of bone union on radio-graphs is difficult to evaluate and not reliable during the first 4 weeks of fixation [21]. Deficiencies in standard radio-graphic techniques for the assessment of the distraction zone have led to an interest in the use of USG for this purpose. Due to an inadequate imaging of non-calcified structures on radiographs, such investigations are rational only after mineralization has commenced. It is not possible to estimate the stability of the callus using radiological methods at the time when distractors are usually removed. Another major disadvantage is the repeated exposure to ionizing radiation during the follow up period. CT imaging is more accurate in the context of the definition of the regenerate. However, the high doses of radiation in CT have a deleterious effect on the patient as well as the regenerate. In addition, metal artefacts and scatter caused by the distraction device frequently hamper evaluation of the region of interest in conventional radiography and CT imaging [22]. In the present study, CT imaging was not used as a protocol, as it was felt that the radiation dose of serial CT images would be very high.
Hirai et al. utilized 30 MHz and 15 MHz frequency B-mode ultrasound probes, applied to five patients with nasal bone fractures, orbital rim fractures, maxillary fractures, and mandibular fractures, and observed that high-resolution USG can be used to diagnose even 0.1 mm wide disruptions of the bony surface as the callus is not mineralized in the initial few weeks [23]. On similar principles, its application in the evaluation of the DO regenerate in the maxillofacial region is the basis of the present study. The present study evaluated USG as a diagnostic aid to assess the quantitative as well as the qualitative aspects of the regenerate. A study by Thurmuller et al. used ultrasound to assess healing of a mandibular distraction wound utilizing ex vivo radiographs and USG. The USG beam penetration depth was measured in millimetres and was used to estimate bone fill using a semiquantitative score. They concluded that USG provides an accurate measurement of the corticotomy gap, early detection of new bone formation, and accurate assessment of bone maturity [24]. In our study, radiographs were valuable in the immediate postoperative period in ascertaining the position of the distraction device as well as the alignment of bony segments, which is not possible with ultrasound. However, mineralization of the regenerate was detected earlier by USG as compared to radiographs (Table 2). The results of the present study also indicate that USG evaluation can be treated as a major diagnostic modality in monitoring the progress of DO and the status of the regenerate. Using a 4-point semiquantitative score and clinical evaluation, radiography, and USG, Troulis et al. indicated that USG is an accurate non-invasive technique that may prove to be useful in assessing the mandibular DO regenerate in patients [22]. The results obtained in this study are similar to those obtained in a study by Hughes et al. in which they used USG at the end of the distraction phase to identify a bony union at the distraction site [25]. USG indicated the timing of distractor removal. They confirmed that ultrasound offers a reliable, safe, and dynamic method of monitoring callus formation and lead to a significant reduction in radiation exposure for the patient [26]. The results of the present study suggest its use as a standard diagnostic modality [27-30].
DO to treat the facial skeleton is another effective method to standard orthognathic surgery for selected patients with different grade of OSA. Furthermore, USG evaluation of the DO zone gives another clinical edge over conventional methods and hence we proposed its use for the evaluation of mandibular regenerate as a standard protocol, with advantage of good patient compatibility, nil exposure to radiation and post effective alternative to CT and conventional radiography.

![]()

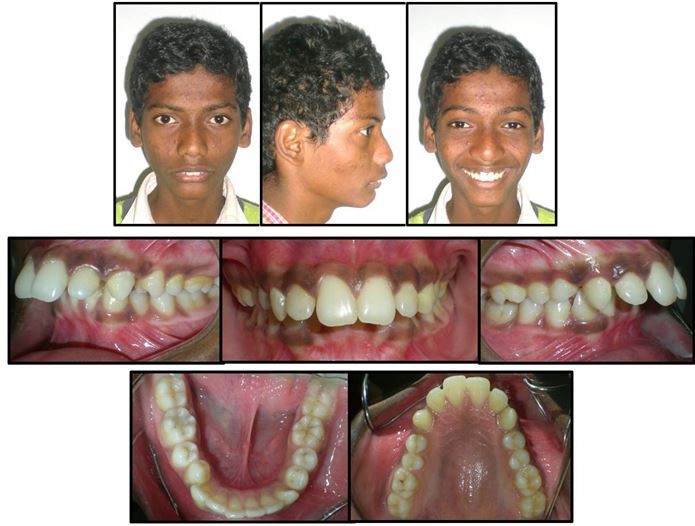 |
| Figure 1: Pretreatment Facial and Intraoral Photographs |
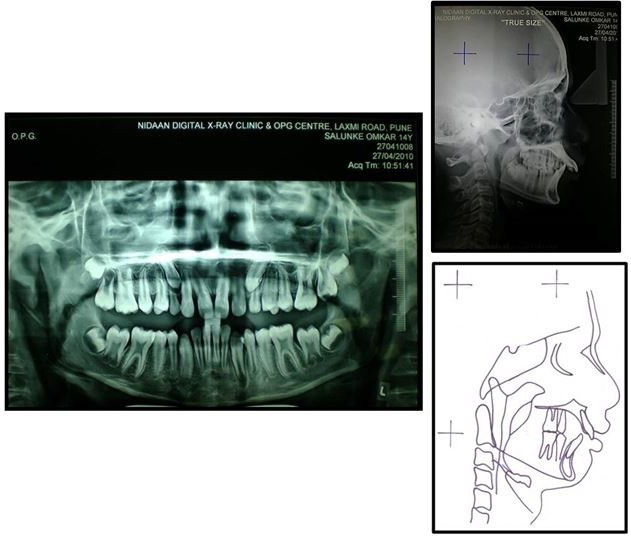 |
| Figure 2: Orthopantomogram, Lateral Cephalometric Radiograph and Tracing |
 |
| Figure 3: Lateral Cephalogram Indicating Upper Airway Space |
 |
| Figure 4: MRI Showing Compromise Airway |
 |
| Figure 5: Initial bonging of Upper and Lower Arch |
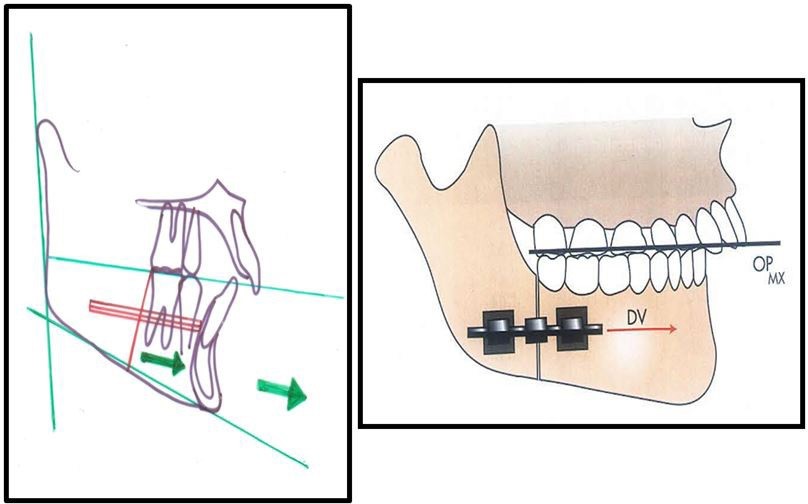 |
| Figure 6: Vector Planning |
 |
| Figure 7: Surgical phase showing Intraoral Distractor in situ |
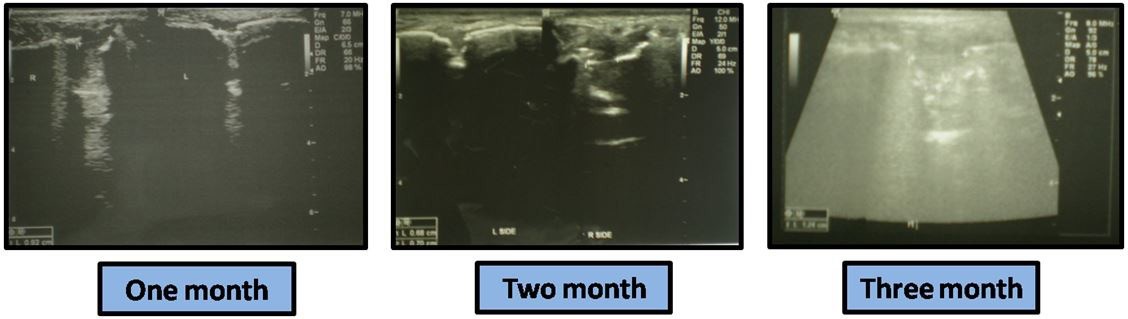 |
| Figure 8: USG Callus Maturation at Different Stages |
 |
| Figure 9: Posttreatment Facial and Intraoral Photographs |
 |
|
Apneas |
Hypopneas |
A + H |
Central |
Obstructive |
Mixed |
#Events |
34 |
53 |
87 |
1 |
86 |
0 |
Index |
5.5 |
8.6 |
14.2 |
0.2 |
14.0 |
0.0 |
Index with Arousal |
2.0 |
1.5 |
3.4 |
0.0 |
3.4 |
0.0 |
Mean duration(s) |
31 |
15.8 |
21.8 |
12.4 |
21.9 |
- |
Longest duration(s) |
87.4 |
49.4 |
87.4 |
12.4 |
87.4 |
- |
Parameters |
Pre-Rx |
Pre-Surg |
Post-Surg |
SNA |
84 O |
84 O |
92 O |
SNB |
93 O |
93 O |
91 O |
ANB |
-9 C |
-9 O |
0 O |
UI-NA |
37 O (10) |
39 O (12) |
36 O (10) |
LI-NB |
19 O (5) |
26 O (6) |
87.4 |
GoGn-SN |
28 O |
28 O |
22 O |
SMA |
22 O |
23 O |
22 O |
IMPA |
98 O |
102 O |
102 O |
LAFH |
69mm |
69mm |
71mm |
Co-A |
84mm |
84mm |
90mm |
Co-Gn |
117mm (107-110) |
117mm |
111mm |
ANS-PNS:GoPoG |
1:1.1.8 |
1:1.1.8 |
1:1.6 |
|
Apneas |
Hypopneas |
A + H |
Central |
Obstructive |
Mixed |
#Events |
26 |
23 |
26 |
1 |
34 |
0 |
Index |
0.5 |
8.6 |
4.5 |
0.2 |
6.0 |
0.0 |
Index with Arousal |
1.0 |
1.5 |
3.4 |
0.0 |
3.4 |
0.0 |
Mean duration(s) |
11 |
15.8 |
21.8 |
12.4 |
11.9 |
- |
Longest duration(s) |
23.4 |
18.4 |
17.4 |
12.4 |
14.4 |
- |




































