Open Access
Research Article
Max Screen
ISSN: 2394-6512
Copyright: © 2023 Akadiri Yessoufou. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background:Despite their good efficacy, antiretroviral drugs often induce adverse effects, in particular hypersensitivity reactions (HSR) which cause significant discomfort leading to the abandonment of treatment and then to therapeutic failure in some HIV-positive patients. Therefore, in this study, we aimed to assess the association between immune responses and hypersensitivity reactions (HSR) induced by antiretroviral treatment in people who living with HIV-1 (PLHIV-1), through the distribution of immune cells and cytokine profiles.
Methods:PLHIV-1 were enrolled at two reference centers in Benin. Clinical data, therapeutic line and adverse reactions were recorded. Serum cytokine levels were determined by ELISA and immune cell frequencies by immunophenotyping us ing flow cytometry.
Results:98 PLHIV-1 individuals aged between 30-50 years old were enrolled, including 71% female, 30% who developed HSR and all were under TDF+3TC+EFV therapeutic line at inclusion date. We observed an increase in IFN-γ levels and conversely a significant decrease in IL-4 in PLHIV-1 who developed HSR. In addition, pro- and anti-inflammatory cytokines (TNF-α, IL-5, IL-6 and IL-13) increased in all PLHIV-1, concomitant with a shift of Th1/Th2 ratio to Th1 phenotype, especially in those who developed HSR. Besides, CD4+ T cell frequencies decreased while those of CD8+ T cells increased in all PLHIV-1, and especially in those who developed HSR. NK and NKT cells frequencies significantly decreased in all PLHIV-1.
Conclusion: Our study showed that immune status of PLHIV-1 having developed ART-associated HSR was linked to an increase in CD8+ T lymphocytes correlated with a proinflammatory Th1 phenotype despite a decrease in CD4+ T lymphocytes and low level of circulating IL-4. These results suggested a decrease in humoral response and in favor of cellular response characteristic of type IV hypersensitivity reactions. Such immune parameters might also show a prognostic power of HSR in PLHIV-1 and the results would better guide clinicians to improve the management of PLHIV-1.
Keywords: PLHIV-1; Antiretroviral Therapy; Hypersensitivity Reactions; Immune Cells; Cytokines
List of AbbreviationsART: Antiretroviral therapy; HIV: Human immunodeficiency virus; PLHIV: People living with HIV; NRTI: Nucleoside reverse transcriptase inhibitors; NNRTI: Non-nucleoside reverse transcriptase inhibitor; IP: Protease inhibitor; IIN: Integrase inhibitor; TDF: Tenofovir; AZT: Zidovudine; 3TC: Lamuvidine; FTC: Emtricitabine; DTG: Dolutegravir; EFV: Efavirenz; ABC: Abacavir; ATV: Atazanavir; LPV: Lopinavir; HSR: Hypersensitivity reactions; IL: Interleukin; TNF-α: Tumor Necrosis Factor Alpha; IFN-γ: Interferon gamma; Th: T-helper.
For over past two decades, antiretroviral drugs have been proven to significantly reduce mortality and morbidity related to HIV infection [1]. However, despite this efficacy, antiretroviral treatment (ART) induced side effects which are one of the major causes of treatment failures in the curative fight against HIV [2]. To date, the most effective pharmacotherapy for the treatment of HIV is a combination of antiretroviral drugs [1]. Indeed, WHO recommends in the standard first-line treatment the combination of two nucleoside reverse transcriptase inhibitors (NRTI) associated with one non-nucleoside reverse transcriptase inhibitor (NNRTI) or one protease inhibitor (PI) or one integrase inhibitor (IIN) [3,4]. Thus, in Benin most of people living with HIV-1 (PLHIV-1) are under the combination of Tenofovir (NRTI) + Lamivudine (NRTI) + Efavirenz (NNRTI). However, the high rate of primary resistance observed in PLHIV-1 and side effects caused by antiretroviral drugs such as Efavirenz (EFV) have led WHO to recommed new high genetics barrier drugs as INI [5,6]. Therefore, Dolutegravir (DTG) as integrase inhibitor has been recommended by WHO to replace EFV. Indeed, since 2019, DTG has been introduced in antiretroviral tritherapy in Benin [7]. Currently, the replacement of EFV by DTG is not yet effective in all PLHIV- 1 in Benin due to the delay in the supply of DTG. For this reason, most of PLHIV-1 remained on combined therapy containing EFV.
Moreover, it has been reported that emergence of drug resistance was not the only cause of treatment failure. Indeed, side effects induced by antiretroviral drugs also appeared as other major causes of therapeutic non-compliance and then therapeutic failure [2]. Most of antiretroviral drugs induced adverse effects including allergy and hypersentivity reactions in some patients [2]. The frequency of drug hypersensitivity was estimated roughly 3-20%. Besides, hypersensitivity reactions related to ART are one hundred times more frequent in HIV- infected patients than in the general population [8]. Indeed, since the introduction of ART in the late 1990s, an increase in hypersensitivity reactions to antiretroviral drugs has been reported [9]. Moreover, the number of HIV-infected patients who experienced adverse drug reactions during their treatment is estimated to be up to 80% [10]. These side effects have been attributed to dysregulation of the immune system, the use of polypharmacy, recurrent infections, increased vulnerability to oxidative stress and genetic factors [11]. Indeed, adverse drug reactions appear more often during the first year of treatment and are the most common reasons for stopping ART in HIV- infected patients [12]. Moreover, the frequency of drug hypersensitivity has been estimated between 11%-35.9% [13]. Adverse drug reactions can be classified into 2 types: type A reactions based on the pharmacological action of the drug called predictable and dose-dependent and type B reactions related to host genetics and hypersensitivity immunological which are said to be unpredictable and dose-independent [14,15]. NNRTI (Efavirenz, Nevirapine), NRTI (abacavir), and IP (amprenavir) are drugs that may cause adverse reactions [16-18]. The main adverse effects caused by Efavirenz are rash, skin eruption, urticaria, erythema and neuropsychiatric disorders [19,20]. Few studies have investigated the real causes of side effects in PLHIV-1 under ART. Particularly in Benin, no study has documented on neither the prevalence of side effects nor the occurence of hypersensitivity reactions upon the use of ART.
Due to potential risk of therapeutic failure in PLHIV-1 which could be induced by these adverse effects, it becomes important to explore the causes of these effects in order to improve the heathcare of PLHIV-1. Some studies have evoked genetic predisposition showing strong association between Human leukocyte antigen (HLA)- B*5701 allele and hypersensitivity to abacavir in PLHIV-1 under ARV treatment [21,22]. Few studies have investigated immunological causes which could explain the observed ARV-induced hypersensitivity reactions in PLHIV-1. In France, some investigators have shown correlation between increased interleukin (IL)-4 production by CD4+ and CD8+ T cells and hypersensitivity reactions to abacavir [23]. Indeed, HIV infection has been characterized by a shift from a T-helper (Th)-1 to a Th-2 cytokine pattern [24]. T-helper 1 cells are known to secrete tumor necrosis factor alpha (TNF-α) and interferon gamma (IFN-γ) which favor cell-mediated responses and have clinical manifestations such as a contact dermatitis. Th-2 cells are characterized by IL-4, IL-5 and IL-13 secretion which favor humoral immune responses and can cause immediate hypersensitivity [25,26]. Besides, studies have reported that variations in pro-inflammatory cytokines could serve as markers of the activation of TCD4 lymphocytes which are the main targets of HIV [27,28]. However, most of these studies did not link the immune parameters and the occurrence of ART-related hypersensitivity reactions in PLHIV-1, despite the critical roles of immune system in hypersensitivity reactions [18,19]. Knowing the immunological causes of these reactions may lead to consider the association of ART along with the treatment of hypersensitivity reactions in PLHIV-1. Therefore, the present study aimed to assess the association between immune responses and hypersensitivity reactions induced by antiretroviral treatment in PLHIV-1, through the distribution of immune cells and cytokine profiles. Such results may allow clinicians to consider additional treatments in order to limit side effects caused by ART and thus reduce non-compliance and therapeutic failures in PLHIV-1.
This cross-sectional study was carried out among routine PLHIV-1 over 18 years old, on antiretroviral treatment for at least 6 months, in two health facilities care in Benin, CHUZ-Sô-Ava/Calavi and Menontin Hospital. Patients started ARV treatment just after the HIV infection diagnostic. Patients were examined for hypersensibility reactions by Clinicians. Specific questionnaire was set up to record anthropometric and clinical data from each participant. Data collected included treatment line and ARV-related adverse effects. Subjects infected with HIV-2 or co-infected with HIV-1 and 2 or having a history of diabetes mellitus, suffering from opportunistic infections, diarrhoea, malaria, and parasitosis or in a state of pregnancy or under anti-inflammatory medication were not included from the study.
A total of one hundred and eighteen (118) participants were recruited in this study. Among them, 20 HIV-negative particpants, apparently healthy and without anti-inflammatory drug treatment, were considered as control group. Fourty-three (43) PLHIV-1 who showed undetectable viral load (< 40 copies/ml) after six month treatment were classified as therapeutic success group (PLHIV-1s), and 55 PLHIV-1 showing viral load ≥1000 copies/ml were classified as HIV treatment failure group (PLHIV-1f). Each PL-HIV group has been divided into two subgroups: a subgroup of PLHIV-1 showing hypersensitivity reactions HSR(+) and the other who did not exhibit hypersentivity reactions HSR(-), resulting in four subgroups: PLHIV-1s_HSR(+) (N=10); PLHIV-1s_HSR(-) (N=33); PLHIV- 1f_HSR(+) (N=19) and PLHIV-1f_HSR(-) (N=36). All PLHIV-1 were under the first line of treatment (TDF+3TC+EFV or TDF+3TC+DTG).
The study was conducted in accordance with the Declaration of Helsinki 1964 (as revised in Edinburgh 2000) and was approved by the National Ethics Committee for Health Research of the Ministry of Health of Benin under the number N°131/MS/DC/SGM/CNERS/SA-2021. Prior to enrollment, all participants were informed of the purpose of the study, gave their free consent and expressed their willingness to participate in the study. We have taken care to fully respect the rights of participants, confidentiality and security of information collected with limited access to only investigators.
Venous whole blood samples were collected from each participant into sterile vacuum blood collection tubes (Becton Dickinson, CA, USA) containing or not EDTA. Blood samples were collected during the onset of HSR in patients who showed HSR. Blood collected in EDTA tube was used for immune cell phenotyping within 2 h after sampling. Plasma was obtained from whole blood after centrifugation (3500 rpm, 20°C, and 10 min) and used for plasma viral load. Serum was isolated from blood collected in tubes without anticoagulant and distributed in aliquots and stored at - 80°C for future cytokine determinations. Repeated freeze-thaw cycles were avoided.
HIV-1 viral load in plasma was determined using automated Abbott m2000 System. The quantification of viral load was carried out by RT-PCR done in 3 steps according to the manufacturer’s instructions. Briefly, RNA was extracted from plasma samples and reverse-transcribed into cDNA. cDNA was amplified using HIV-1 specific and internal control primers with quencher and reporter labeled probes. The intensity of the fluorescence is proportional to the quantity of RNA present thus determining the viral loads.
IFN-γ and IL-4 (respectively Th1 and Th2 cytokines), TNF-α and IL-6 (as pro-inflammatory cytokines); IL-5 and IL-13 (as anti-inflammatory cytokines) were determined in serum by ELISA method using Human Peprotech Elisa Kits (Rocky Hill, NJ 08553 USA), according to manifacturer’ instructions. Briefly, the protocol for determination of serum cytokine levels is composed of four big steps: (i) Preparation of buffers, (ii) Coating the plates, (iii) Technical protocol and (iv) Results and data interpretation. Details of the protocol are presented in the supplementary annex file as Supplementary methods: serum cytokine assay protocol.
Immne cell frequencies were determined as previously described [29]. Briefly, monoclonal antibodies purchased from BD Pharmingen (France) were used to label immune cells in whole blood. A combination (3 µl per each monoclonal antibody) of anti-CD3-PerCP, anti-CD4-FITC, anti-CD8-PE and anti-CD56-APC was made for respectively labelling CD4+ and CD8+ T lymphocytes, NK and NKT cells; and a second combination (3 µl per each monoclonal antibody) of anti-CD3-PerCP, anti-CD14-FITC, anti-CD16-APC/Cy7 and anti-CD19-PE was used to label monocytes, B lymphocytes and polynuclear neutrophils (PNN) and eosinophils (PNE). In practice, 300µl of whole blood was used for cell staining. Indeed, blood was incubated with optimized volume of antibodies (3 µl per each) for 30 minutes at 4°C in the dark. Then red blood cells were lysed using Facs-Lysing buffer-1X (2mL of Facs Lysing is added to each tube) and the mixture was incubated for 10 min at room temperature in the dark and washed twice with PBS-1X (3 mL of 1X PBS was added and centrifuged for 8 min at 1000 rpm at 4°C). Stained cells were suspended in 300 µl of PBS 1X and 100,000 cells from each tube were acquired with the BDFACSCanto II flow cytometer. Results were analyzed using FlowJo 7.6 software version 10.8.1, BD Pharmingen, France). Gating strategies for immune cell identification are shown as supplementary data (supplementary Figure 1 and Figure 2).
Cytometry results were analyzed with FlowJo 7.6 software version 10.8.1 and the graphs were drawn with GraphPad Prism software (version 8.3.0). The results were presented as median values (IQR). The statiscal differences for cytokine levels and immune cell frequencies between control subjects and PLHIV-1 were analyzed using the non-parametric method of Kruskal-Wallis, following by Dunn’s multiple comparisons. Differences were considered statistically significant when p values < 0.05.
Table 1 presents age, sex, viral load and CD4+ T cell counts of PLHIV-1. The median age of participants was 42 [36.25-49] years, and female subjects represented 71.4%. The average CD4+ T cell count in PLHIV-1 was 273 [162-403] cells/µl. The average viral load in PLHIV-1 with treatment failure was 4.6 [3.9-5.2] Log
Table 1 presents the prevalence of HSR in PLHIV-1 according to antiretroviral treatment. PLHIV-1 were under two therapeutic lines, TDF+3TC+EFV or TDF+3TC+DTG; however, most of them were under TDF+3TC+EFV, i.e. 73.5%. At the inclusion date, a total of 29/98 PLHIV-1 (i.e. 29.6%) have developed HSR and were all under TDF+3TC+EFV, and no patient under TDF+3TC+DTG have shown HSR. The most observed hypersensitivity reactions in our stuy population were mouth ulceration, skin rash, allergy, dermatosis, pruritus and respiratory disorders. The details of hypersensitivity reactions are shown in supplementary data (supplementary Table 1).
Independently of HSR status, PLHIV-1 groups exhibited lower concentrations of IFN-γ than control group. The decrease was significant in PLHIV-1s_HSR(-) and PLHIV-1s_HSR(+) (p < 0.0001 and p = 0.002 respectively). However, the IFN-γ levels were significantly higher in PLHIV-1s_HSR(-) compared to PLHIV-1f_HSR(-)(p=0.01) and PLHIV-1s_HSR (+) (p=0.007). Moreover, PLHIV-1 with HSR exhibited higher levels of IFN-γ than those who did not show HSR (Figure 1a).
Regardless to HSR or therapeutic status, IL-4 levels increased in PLHIV-1 compared to control subjects. However, patients with therapeutic success and who did not show HSR had higher level of IL4 than the other groups.
Moreover, PLHIV-1 who showed HSR exhibited low levels of IL-4 concentrations as compared to those who did not show HSR (Figure 1b).
Independently of HSR status, PLHIV-1 groups exhibited high levels of proinflammatory cytokines compared to control subjects. Indeed, TNF-α and IL-6 were significantly higher in PLHIV-1f_HSR(+) (p=0.0003 and p< 0.0001, respectively) than controls. Only, IL-6 level was significantly increased in PLHIV-1f_HSR(-) (p< 0.0001) compared to controls (Figure 1c; Figure 1d).
Besides, TNF-α and IL-6 were significantly higher in PLHIV-1f_HSR(+) (p=0.04 and p< 0.004, respectively) compared to PLHIV-1s_HSR(-). Only, IL-6 level was significantly increased in PLHIV-1f_HSR(-) (p=0.003) compared to PLHIV-1s_HSR(-). However, the levels of these cytokines were higher in PLHIV-1 who showed HSR compared to those who did not show HSR (Figure 1c; Figure 1d).
All the PLHIV-1 groups exhibited higher levels of IL-5 and IL-13 cytokines than control subjects. The increases were more pronounced and significant for IL-5 in PLHIV-1f_HSR(-) and PLHIV-1f_HSR(+) (p< 0,0001 and p=0,001 respectively) compared to controls subjects. Moreover, IL-13 levels were significantly higher in PLHIV- 1f_HSR(+) compared to PLHIV-1s_HSR(-) (p=0.01) and to control suvbjects (p=0,008) (Figure 1e; Figure 1f).
Independently to the presence or not of HSR, the frequencies of CD4+ T cells significantly deacreased while those of CD8+ T cells increased in PLHIV-1 as compared to control subjects (p< 0.05). The decrease of CD4+ T cells and the increase of CD8+ T cells were more pronounced in PLHIV-1f than in PLHIV-1s (Figure 2a; Figure 2b).
The frequency of NK cells was decreased in all PLHIV-1 groups compared to control subjects but the decrease was significant in PLHIV-1f (p< 0.05). NKT cells exhibited same profiles of decrease as CD4+ T cells in PLHIV-as compared to control subjects (p< 0.05) (Figure 2c; Figure 2d). A trend to decrease but not significant was observed in B cells frequencies in PLHIV-1 groups regardless of HSR and therapeutic status as compared to control subjects (Figure 2e).
As shown in Figure 3a, no significant difference was observed in the frequencies of monocytes CD14+ between PLHIV-1 groups. However, PLHIV-1f_HSR(-) presented low frequencies of classical and non classical monocytes compared to control subjects (p< 0.05) (Figure 3b; Figure 3d). A high frequency of intermediate monocytes was observed in PLHIV-1f_HSR(+) compared to healthy controls (p=0.02) (Figure 3c).
The frequency of granulocytes was lower in HIV infected group compared to control subjects. The low frequency is statistically significant in PLHIV-1f without and with HSR (p=0.001 and p=0,006 respectly) (Figure 3e) .
Although the p-values were not significant, we observed a trend of increasing eosinophils and decreasing neutrophils in the PLHIV-1 groups, except for the PLHIV-1s_HSR(-) groups. However, the trend of increasing eosinophils and decreasing neutrophils was more pronounced in the groups that exhibited HSR compared to those that did not (Figure 3f; Figure 3g).
The heatmap figures on correlation between CD4 and CD8 T cells and differents cytokines is shown in Figure 4. There was no significant correlation between CD4, CD8 T cells frequency and IFN-γ concentration in the differents groups (Figure 4). There was no significant correlation between CD4 and TNF-α in differents groups but a negative correlation between CD8 and TNF-α in PLHIVs_HSR(-) (p< 0,05) and a positive correlation between CD8 and TNF-α in PLHIVs-HSR(+) (p< 0,05). No significant correlation between CD4, CD8 T cells and IL-4, IL-6, IL-13 in the differents groups was observed (Figure 4).There was a positive and negative correlation between CD4 T cells and IL-5 respectively in PLHIVf_HSR(-) and PLHIVf_HSR(+) (p< 0,05) ; and a positive correlation between CD8 T cells and IL-5 in PLHIVf_HSR(+) (p< 0,05) (Figure 4).
Despite their effectiveness in fighting HIV infection, ARV drugs have often caused adverse effects which have been one of the main indirect causes of treatment failures among PLHIV-1. In order to explore the role of immune system in the occurrence of ART-induced adverse reactions, we investigated immune cell frequencies along with cytokine profiles in PLHIV-1 who presented hypersensitivity reactions after ART.
Fisrt, it is interesting to remark that, in our study, PLHIV-1s showed indetectable viral load as compared to PLHIV-1f who exhibited high viral load. We observed that 71% of our study population were women, in line with several other studies [30,31]. In the pre sent study, 30% of PLHIV-1 had developed hypersensitivity reactions and they were all under TDF+3TC+EFV therapeutic line. The most observed hypersensitivity reactions in our study population were mouth ulceration, skin rash, mycosis, allergy, dermatosis, pruritus and respiratory disorders. Indeed, it has been reported that cutaneous hypersensitivity reactions are the most frequent side effects observed in PLHIV-1 under ART [32,33].
As expected, concomitant decrease of CD4+ T cells and increase of CD8+ T cells were observed in PLHIV-1 regardless of the presence of ART-induced adverse reactions as compared to control subjects. In this condition, the decrease of CD4+T cells and increase of CD8+ T cells were more pronounced in PLHIV-1f than in PLHIV-1s, suggesting that the ART has contributed to progressive restoration of immune system in PLHIV-1s. Our findings were similar to results obtained by others researchers [34,35] that showed a negative correlation between CD4+ T cells and viral load in HIV infection. Our results also suggested that destruction of CD4+ T cells by HIV infection seemed to be compensated by the increase CD8+ T cells in PLHIV-1 [36]. Similarily, others previous studies have also reported a decrease of CD4+T cells and an increase of CD8+ T cells in HIV infection [37-39].
As far as T-cell derived cytokines are concerned, we observed in this study that serum IFN-γ significantly decreased in PLHIV-1, while circulating IL-4 increased, compared to control subjects. Nevertheless, the IFN-γ levels appeared higher in PLHIV-1f than those of PLHIV-1s, suggesting that therapeutic failure in HIV infection might be associated with high IFN-γ concentrations. In fact, serum IFN-γ is expected to be low during HIV infection [40] as CD4+Th1 cells, one of the major cells that secrete IFN-γ, have been depleted during chronic HIV infection [41]. But, the positive correlation between IFN-γ /CD8+ T cells and the negative correlation between IFN-γ/CD4+ T cells in PLHIV-1 observed in this study suggested that IFN-γ was predominantly secreted by CD8+ T cells. Indeed, similar results have been observed by other studies which reported consistently high rates of circulating IFN-γ levels in HIV-1 infected people despite ART [42,43]. Conversely to our results, some studies have shown that IFN-γ levels have decreased in HIV-infected people on ART [44,45]. On the other hand, we found that PLHIV-1 who showed HSR exhibited higher IFN-γ levels than those who did not showed HSR. Indeed, some researchers have also reported a significantly higher IFN-γ levels in the symptomatic HIV-1 infected individuals compared to asymptomatic groups [46]. The positive correlation between IFN-γ levels and CD8+ T cells which increased in PLHIV-1 who showed HSR suggested that HSR might be due to combined effect of high CD8+ T cells and increased IFN-γ in PLHIV-1_HSR(+) [47,48].
In this study, the profiles of IL-4 and of IFN-γ were different even if the levels of IL-4 were relatively higher in PLHIV-1 than in control subjects. This difference observed suggested that IL-4 synthesis might not be linked solely to HIV infection alone. Regardless of successful of treatment or not, PLHIV-1 with HSR showed low levels of circulating IL-4 than patients with no HSR, suggesting that occurrence of HSR might be associated with low Th2 phenotype in PLHIV-1 with HSR. Similary to our results, Musa et al. have reported elevated IL-4 levels in HIV patients with a high viral load [28]. Conversely, Soufian et al. have reported low levels of serum IL- 4 in HIV infected individuals compared to HIV negative subjects [49]. In addition, [23] showed that IL-4+ T cells in the abacavir HSR group were higher than in subjects without HSR. This discrepancy could be explained by the fact that these authors measured the intracellular IL-4 specifically produced by the T lymphocytes, whereas in our study, we measured the circulating IL-4 which is not specific to CD4+ T cells. Moreover, the HSR appeared to be linked to abacavir, a nucleoside reverse transcriptase inhibitor, whereas in our study, the HSR were linked to efavirenz, a non-nucleoside reverse transcriptase inhibitor. In fact, the concomitant decrease of IL- 4/CD4+ T cells and increase of IFN-γ/CD8+ T cells in PLHIV-1 with HSR compared to PLHIV-1 without HSR, suggested that HSR would be much more linked to IFN-γ-producing CD8+ T cells than to IL-4-producing CD4+ T cells which decreased in PLHIV-1 with HSR. Moreover, due to cytotoxic ability of CD8+ T cells, their increase in PLHIV-1 with HSR could suggest that they may be involved in the occurrence of allergic hypersensitivity reactions. Indeed, some studies have reported that a cytotoxic skin reaction mediated by CD8+ T cells seems to be more dangerous than CD4+ T cell-mediated cytotoxicity [50,51]. Keratinocytes are potential targets for CD8+ T cells because they all express MHC-I, while responses mediated by CD4+ T cells are directed to a few cells expressing MHC-II [50,51]. Additionally, the massive presence of CD8+ T cells is characterized by the most severe reactions such as Stevens Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) [50,51].
To better understand the relationship between HSR and Th-cell phenotype relative to cytokines IFN-γ (Th1) and IL-4 (Th2), we calculated the Th1/Th2 ratios in order to appreciate the phenotype of PLHIV-1. We found that Th1/Th2 ratio was in quasi-equilibrium in PLHIV-1s_HSR(-) (0.91), whereas it was strongly polarized towards Th1 phenotype in control subjects (32.60) (Figure 1G). These ratios remained at high Th1 phenotype in the following proportions 6.70-fold in PLHIV-1s_HSR(+), 7.31-fold in PLHIV-1f_HSR(-) and 40.66-fold in PLHIV-1f_HSR(-). Our results showed that highly polarized Th1 phenotype in control subjects decreased sharply in PLHIV-1, suggesting that HIV infection strongly downregulated Th1 phenotype. However, in PLHIV-1f with HSR, the ratio remained strongly biased to Th1 phenotype (40.66 times), suggesting that high viral load combined with HSR may have created a potential pro-inflammatory state in these patients. These observations migth explain the behavior of high IFN-γ and low IL-4 in PLHIV-1 with HSR compared to those without HSR [42,43].
In attempt to link the Th-cell phenotype in the occurrence of HSR to the inflammatory status in PLHIV-1, we assessed serum levels of TNF-α and IL-6 as proinflammatory cytokines. Our study revealed, independently to the treatment outcome, that all PLHIV-1 showed an increase in both proinflammatory cytokines TNF-α and IL-6, suggesting that all these patients were in a pro-inflammatory state. Additionally, therapeutic success was associated with low levels of these cytokines, indicating that HIV infection induced an inflammatory status which was corrected by ART. Similar to our findings, some studies reported that TNF-α and IL-6 were high in HIV-1 infected individuals and decreased with consistent use of ART [52,53]. Contrary to our results, some studies have reported no changes in serum IL-6 levels among HIV patients on ART [54,55]. This divergent of data in cytokine studies can be attributed to the various mechanisms of immune activation that are differentially affected by antiretroviral therapy, slow immune reconstitution despite ART and poor therapeutic adherence. Moreover, the increases of both cytokines were more remarkable in PLHIV-1 who developped HSR compared to those whithout HSR which led us to assume that these cytokines play an important role in the appearance of HSR. Thus, there was a positive correlation between CD8+ T cells and TNF-α in PLHIV-HSR(+) suggesting that HSR leads to an increase in cellular response. In fact, Th1 immune reactions have been reported to act as co-stimulators for pro-inflammatory responses such as elevation of TNF and CD8+ T lymphocytes responses consistent with hypersensitivity reactions [51,56].
IL-5 and IL-13 are anti-inflammatory cytokines produced by Th2 cells which promote B cell production of IgE and IgG4, macrophage deactivation, mast-cell and eosinophil responses [25,57]. In the present study, both cytokines (IL-5 and IL-13) significantly increased especially in PLHIV-1f_HSR(+). The concomitant increase of IL-5 and eosoniphils in PLHIV-1f_HSR(+) was consistent with the increase of TNF-α and IL-6, describing the above chronic inflammatory state in PLHIV-1f_HSR(+). Moreover, there was a positive correlation between T cells (CD4 and CD8) and IL-5 in PLHIVf_HSR(+). Indeed, it has been reported that elevated IL-5 production leads to eosinophilic inflammation characteristic of many drug hypersensitivity reactions [56,57].
It is commonly known that NK cells play important role in controlling acute HIV infection by producing cytokines, including IFN-γ, and mediating lysis of virus-infected cells before the onset of adaptive immunity [58].
NKT cells are a bridge across innate and adaptive immune responses and have an important role in chronic viral infections [59]. In our study, the frequencies of NK and NKT cells were low in PLHIV-1 groups compared to control subjects, and their decreases were more pronounced in patients who showed HSR. The fact that IFN-γ increased while NK and NKT decreased in PLHIV-1 with HSR suggested that IFN-γ is not produced by these cells. The decrease in the proportion of these cells in PLHIV-1 with HSR suggested that these cells seem to play no role in the onset of hypersensitivity reactions. Our findings were similar to those obtained by other investigators [59,60]. Our results showed that both HIV infection and HSR induced no significant change in B lymphocytes frequencies, suggesting that B cells might not be involved in the appearance of HSR in PLHIV-1. Monocytes play critical roles in HIV transmission, early viral spread during infection, and as a reservoir of virus throughout infection [61]. In our study, we found that, except for intermediate monocytes which increased, there was a trend of decreasing classical and no classical monocytes in all patient groups compared to control subjects, suggesting that HIV infection may be associated with low monocyte counts. In line with our results, others studies foundhigher proportions of intermediate monocytes than classical populations in HIV-infected patients [62,63].
To sumup, our study revealed that PLHIV-1_HSR(+) were under TDF+3TC+EFV treatment. The appearance of HSR due to TDF+3TC+EFV in PLHIV-1 was associated with Th1 phenotype response consistent with increase of CD8+ T cells, IFN-γ, TNF-α and IL-6. According to Coombs and Gell, hypersensitivity reactions can be classified into type I or immediate-type hypersensitivity reactions which are mediated by drug-specific IgE antibodies, type II reactions are based on immunoglobulin-mediated cytotoxic mechanisms, type III reactions mediated by immune-complex responses, and type IV reactions known as delayed hypersensitivity reactions mediated by drug-specific T lymphocytes [64]. Based on this classification, our results suggested that HSR in PLHIV-1 seemed to be type IV hypersensitivity reactions. Indeed, Th1 cells have been reported to activate CD8+ T cells, corresponding to Th1 immune reactions characteristic of type IV reactions [51,56].
In conclusion, our study provided new insights into the involvement of immune system in the onset and the type of hypersensitivity reactions induced by ART in PLHIV-1. This would better guide clinicians in the management of these patients, advising them to combine anti-HSR treatments with ARVs, in order to minimize the appearance of these reactions and thus optimize the chances of therapeutic success in PLHIV-1. Moreover, the immune parameters studied may also serve as prognostic or predictive values of HSR in PLHIV-1. Indeed, the increase in CD8+ T cells, IFN-γ, TNFα, IL-6 and PNE in PLHIV-1 (treatment failure and success) who showed HSR reactions could serve as prognostic parameters and useful in the diagnosis of HSR.
Although the number of patients who developed hypersensitivity reactions was small in this study, the association demonstrated between hypersensitivity reactions and the concerned immune cells and cytokines was strong. Moreover, some limitations of this study rely on the fact that patients were included based on self-reported information regarding certain ART-induced effects. Nevertheless, cutaneous hypersensitivity reactions were clearly visible and examined by the Clinicians. Further large-scale studies are thus needed to better understand the mechanisms of immune system in the occurrence of hypersensitivity reactions in order to define suitable generalized prevention and treatment strategies.
This work was carried out in the Laboratory of Cell Biology, Physiology and Immunology, Department of Biochemistry and Cellular Biology, Faculty of Sciences and Technology (FAST) and Institute of Applied Biomedical Sciences (ISBA), University of Abomey-Calavi (UAC), under the Ministry of Higher Education and Research of the Republic of Benin. The authors thank the engineers, technicians, students for their valuable technical advices and contributions. We are also very grateful to the participants from the two hospitals where the study took place. We sincerely thank Dr. Geneviève Tchigossou (Laboratory of Agro-EcoHealth Platform, International Institute of Tropical Agriculture, Cotonou, Benin) for having carried out extensive proof reading of the manuscript and improved the English style.
Not applicable. This work has not received any funding from any organization. The work was financed from the authors’own funds. Products and reagents were purchased by the contribution of the authors themselves.
APA was in charge of major parts of technical aspects of work and wrote the manuscript. PYA, ET and OPN participated in the technical work and contributed in the interpretation of data. KM, NF and CD contributed to the development of protocol. AY designed the study, supervised the work, participated in the manuscript writing and established the collaborative aspects. All authors read and approved the final manuscript.
The study was conducted in accordance with the Declaration of Helsinki 1964 (as revised in Edinburgh 2000) and was approved by the National Ethics Committee for Health Research of the Ministry of Health of Benin under the number N°131/MS/DC/SGM/CNERS/SA-2021. Written informed consent to participate in this study was provided by the participants

![]()

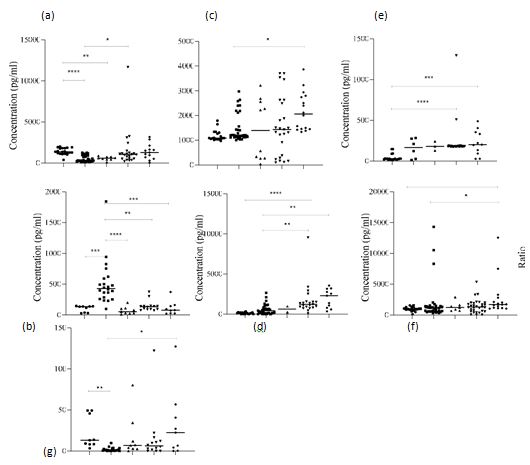 |
| Figure 1: Serum cytokines levels in the study groups. Data are presented as median (IQR, interquartile range). The levels of serum cytokines of IFN-? (a), IL-4 (b), TNF-a (c), IL-6 (d), IL-5 (e), IL-13 (f) and IFN-?/IL-4 (g) are shown . The data are presented for five studied groups: Healthy subjects (N=20), PLHIV in therapeutic success who did not showed HSR (PLHIVs-HSR(-), N=33), PLHIV in therapeutic success who showed HSR (PLHIVs- HSR(+), N=10), PLHIV in therapeutic failure who did not showed HSR (PLHIVf-HSR(-), N=36); and PLHIV in therapeutic failure who showed HSR (PLHIVf-HSR(+), N=19). Statistical analyses were performed using the nonparametric Kruskal-Wallis test. Significant differences were indicated as *p < 0.05; **p < 0.01; ***p < 0.005 or ****p < 0.001. |
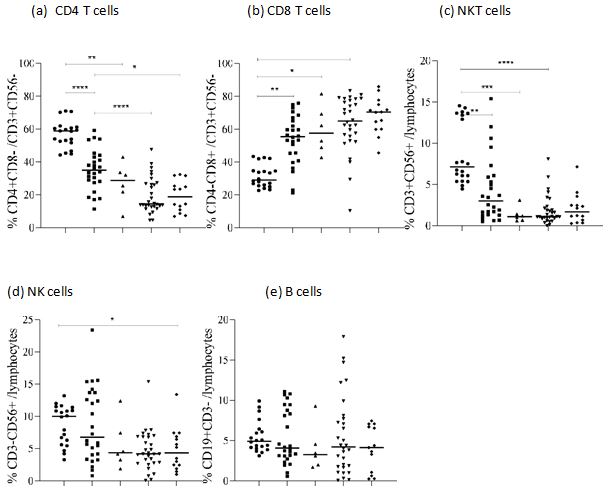 |
| Figure 2: Frequencies of T and B lymphocytes in the study groups. Data shown as box plots representing medians with 25th and 75th percentiles. The frequencies of lymphocytes CD4+ (a), CD8+ (b), NKT cells (c), NK cells (d) and B cells (e) are shown. The data are presented for five studied groups: Healthy subjects (n=20), PLHIV in therapeutic success who did not showed HSR (PLHIVs-HSR(-), n=33), PLHIV in therapeutic success who showed HSR (PLHIVs-HSR(+), n=10), PLHIV in therapeutic failure who did not showed HSR (PLHIVf-HSR(-), n=36); and PLHIV in therapeutic failure who showed HSR (PLHIVf-HSR(+), n=19). Statistical analyses were performed using the nonparametric Kruskal-Wallis test. Significant differences were indicated as *p < 0.05; **p < 0.01; ***p < 0.005 or ****p < 0.001. |
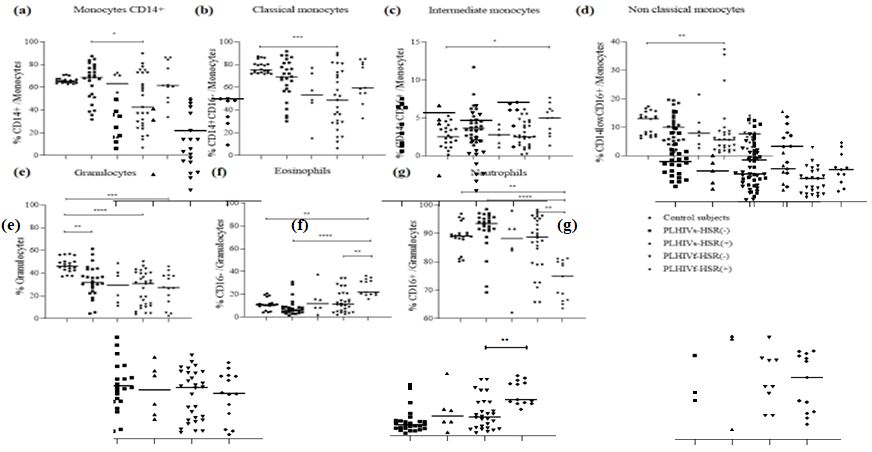 |
| Figure 3: Frequencies of monocytes subpopulations and polynuclear cells in the study groups. Data shown as box plots representing medians with 25th and 75th percentiles. The frequencies of CD14+ monocytes (a), classical (b), intermediate (c), no classical (d) monocytes, granulocytes (e), eosinophils CD16- (f) and neutrophils CD16+ (g) are shown. The data are presented for five studied groups: Healthy subjects (n=20), PLHIV in therapeutic success who did not showed HSR (PLHIVs-HSR(-), n=33), PLHIV in therapeutic success who showed HSR (PLHIVs- HSR(+), n=10), PLHIV in therapeutic failure who did not showed HSR (PLHIVf-HSR(-), n=36); and PLHIV in therapeutic failure who showed HSR (PLHIVf-HSR(+), n=19). Statistical analyses were performed using the nonparametric Kruskal-Wallis test. Significant differences were indicated as *p < 0.05 ; **p < 0.01 ; ***p < 0.005 or ****p < 0.001. |
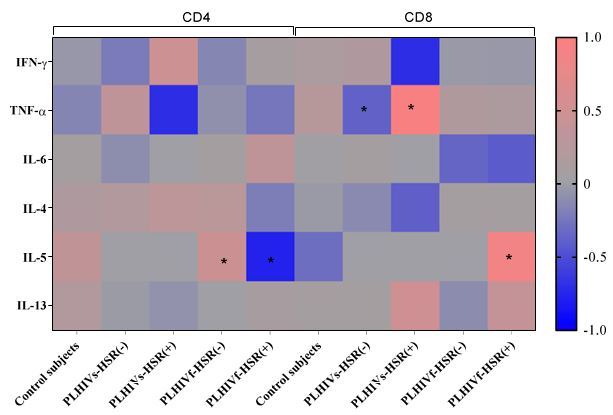 |
| Figure 4: Correlation of serum cytokines levels with frequencies of T cell subsets. Figure shows correlation between CD4+, CD8+ T cells and cytokines. The heat map is made using correlation coeficient 'r' value. *p< 0.05 indicates significant difference. |
Data |
Healthy control subjects N=20 |
PLHIV-1s_HSR(-) N=33 |
PLHIV-1s_HSR(+) N=10 |
PLHIV-1f_HSR(-) N=36 |
PLHIV-1f_HSR(+) N=19 |
Total number or average for all PLHIV-1 N=98 |
Sex, N (%) |
|
|
|
|
|
|
Female |
11 (55) |
21 (63.6) |
9 (90) |
27 (75) |
13 (68,4) |
70 (71.4) |
Male |
9 (45) |
12 (36.4) |
1 (10) |
9 (25) |
6 (31.6) |
28 (28.6) |
Age (years) |
35 |
45 |
36,5 |
40 |
40 |
42 |
Median, [IQR] |
[30.25 - 40.75] |
[41-51] |
[30.5-47.75] |
[37.75-49] |
[34-36] |
[36.25-49] |
Viral load (Log10) |
|
|
|
|
|
|
<1.6 |
Not determined |
Undetectable |
Undetectable |
- |
- |
- |
≥ 3 |
- |
- |
- |
4.66 [3.97-5.06] |
4.5 [3.76-5.19] |
4.6 [3.9-5.2] |
CD4+ T cell number (cells/µl) Median, [IQR] |
Not determined |
369,5 |
216,5 |
269 |
181 |
273 |
|
[257.25-518.25] |
[156.75-273] |
[160-352] |
[72.5-385.5] |
[162-403] |
|
Therapeutic lines N (%) |
|
|
|
|
|
|
TDF+3TC+EFV |
- |
14(14.3) |
10 (10.2) |
29(29.6) |
19 (19.4) |
72 (73.5) |
TDF+3TC+DTG |
- |
19(19.4) |
0(0) |
7 (7.1) |
0(0) |
26 (26.5) |




































