Open Access
Research Article
Max Screen
ISSN: 2455-7641
Copyright: © 2022 Rateesh Sareen. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
The current case report illustrates role of vigilant laboratory services that helped in unmasking asymptomatic HbE variant in a middle aged known diabetic woman who came as an outdoor patient and on subsequent HbA1c testing was found to have lower value -2.9 %. It triggered extensive workup after looking for common causes and an electrophoresis of Hemoglobin revealed HbE variant.
The case also summarizes common causes of spurious low and high HbA1c values which are encountered on regular basis by laboratories. Such abnormal values that do not correlate with blood glucose values mandates workup and shouldn’t be left without work up.
Keywords: Spurious glycated hemoglobin; Latent hemoglobinopathy
Abbreviations: Glycated hemoglobin - HbA1c; Hemoglobin E - HbE Hemoglobinopathies are known to arti factually alter hemoglobin A1c (HbA1c) concentration. [1] The American diabetes association recommends testing for glycated hemoglobin (Hb A1C) for diagnosis and monitoring of diabetes. [2] Here we report a case of diabetes with normal hemoglobin level but reduced HbA1c. The case holds clinical relevance as A1c is frequently ordered test and therefore close attention at the part of pathologists & laboratory personnel could enable us to unfold asymptomatic Hemoglobinopathies.
A middle aged 55yearold known diabetic woman came to OPD for routine investigations. The investigations showed Hb- 12.0 g/ dl WBC Count- 10.5 x 13/ uL, MCV-75.2 fl, MCH- 24.6 pg, MCHC-32.8 g/dl, Platelet count – 353 x 103 /uL and WBC differential showing – Neutrophils- 63%, Lymphocytes- 32%, Monocytes- 02% & Eosinophils- 03%. The biochemical investigations showed serum creatinine- 0.6 mg/dL, SGPT- 57 IU, Total cholesterol- 195 mg/dl, HDL- 41 mg/dl, LDL- 117 mg/dl, VLDL- 37 mg/dl & Triglyceride- 185 mg/dl. (Table -1) The patient serum blood glucose was 236 mg/dl but surprisingly the HbA1c was far lower than expected value at 2.9 % (Fully automated HPLC Variant II Turbo, Bio rad Laboratories, Munich, Germany) (Figure1) The abnormal A1c value prompted laboratory to repeat test to eliminate any potential source of preanalytical error. The repeat testing showed A1c -2.9% and fasting blood glucose – 230 mg/dl. The exceptionally low level of A1c prompted further work up to evaluate the cause and a hemoglobin electrophoresis revealed patient presence of Hemoglobin E. (Figure 2).
HbA1c was available for testing in 1978 and was put in to clinical use in 1980’s. [3] Glycated hemoglobin (HbA1c) is formed by non enzymatic glycation of the beta chain of hemoglobin A by plasma glucose. [4 ] The initial reaction is reversible which results in the formation of an aldehyde Shiff ’s base and later an irreversible reaction takes place that forms a stable ketomine by Amadori rearrangement. The level of A1c is directly proportional to the blood glucose level and life span of RBC. [5,6] The Schiff ’s base formed is unstable known as Labile hemoglobin A1c or Pre Hb A1c or LA1c or pre glycohemoglobin which cannot be separated from stable ketoamine fraction by the currently available methods.[7] The latter stable ketomine undergoes irreversible glycation and occurs continuously throughout the life span of red blood cells i.e 120 days [8,9] This property serves as principle for using A1c as long term glycemic control as diabetes is rampant worldwide.
The American Diabetic association (ADA) in 2010 recommended the use of HbA1c as diagnostic test for screening for Diabetes mellitus type II. [10,11] ADA standards of medical care in diabetes, consensus statement by American association of clinical endocrinologists (AACE) and guidance statement update from American college of physicians (ACP) , published guidelines for HbA1c target for glycemic control for non pregnant adults with type II diabetes mellitus in 2018. [12, 13] As per ADA guideline the diagnosis of diabetes mellitus is made when A1c value is more than or equal to 6.5%. (154.1 mg/dl). Prediabetes is defined as A1c value between 5.7% to 6.4%. The diagnosis of type I DM in individuals with overt symptoms of hyperglycemia in pediatric age group to be made using plasma glucose concentration rather than HbA1c levels [14] whereas for the diagnosis of type 2 DM in younger as well as older patients – A1c, fasting plasma glucose and 2 hour Post prandial values after oral glucose tolerance test may be used. [15] The guideline also recommends the testing for HbA1c levels twice a year for patients who have achieved stable glycemic control and for those who have not achieved glycemic control, a quarterly testing of A1c is recommended. [16]
A1c testing is advantageous than other glucose estimation methods as it does not involve any special preparation like overnight fasting requirement and therefore can be done at any point of time during the day. There is also less variability in levels of A1c as compared to fasting blood sugar [17,18]
The commonly methods used for measuring A1c [19,20]
1. Liquid chromatography
2. Immunoassay
3. Boronate affinity
4. Ion exchange high performance liquid chromatography
5. Capillary electrophoresis
A1c measurement is advantageous as it eliminates preanalytical issues of testing because it does not require fasting state of patient and is less affected by physiological changes. It results from post translational addition of glucose to N-terminal valine of beta chain of hemoglobin.
However, A1c is not full proof and it is affected by many factors like race & age, African- American having higher A1c values in comparing with non Hispanic whites. [14,21] One of the most important condition that results in erroneous A1c estimation is hemoglobinopathy. Hemoglobinopathies affect the reliability of A1c testing by threefold mechanism- altering normal glycation of HbA to HbA1c, abnormal chromatography peak and shorter red cell survival. Table -1 depicts various situations that may result in spurious HbA1c values.
The situations where A1c does not yield accurate results one has to adopt alternative methods to assess long term glycemic control like fructosamine level, glycated albumin or 1,5 anhydroglucitol [23]. Fructosamine test is useful in patients having renal disease however they have limitation in states associated with hypoproteinemia. [24,25] Similarly, glycated albumin may be used for assessment of glycemic control over 2to3 week period. [24,25] 1,5 anhydroglucitol may also be used as higher glucose concentration competitively inhibit its renal absorption resulting in inverse relationship with blood glucose concentration. Mendlovic et al [26] in their review found fructosamine estimation as a good alternative method for cases where long term glycemic control using A1c cannot be performed in presence of hemoglobinopathy.
HbA1c has been used for long term glycemic control and therefore low HbA1c values below reference range are not given clinical relevance rather neglected and should be worked up as the literature studies which have shown that low HbA1c values of (< 5%) are associated with increased risk of mortality showing a J shaped or Ushaped association between HbA1c & all cause mortality. [27-30] The low HbA1c values are general marker of ill health, liver disease and early stage of cancer. [27, 30, 31] Our case highlights the importance of evaluating very low HbA1c levels that unfold in asymptomatic hemoglobinopathy HbE and therefore mandates work up for all extremely low HbA1c levels for better health surveillance.
Conflict of interest- Nil
Sources of funding – Nil

![]()

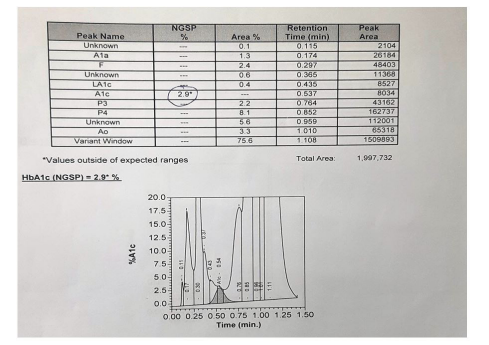 |
| Figure 1: HbA1c Bio rad variant II |
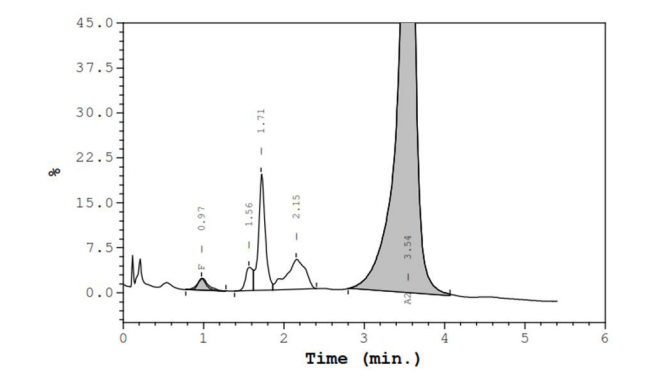 |
| Figure 2: Hemoglobin electrophoresis showing abnormal high HbA2 due to presence of Hb E (Bio rad Laboratories, Munich, Germany) which was confirmed by second electrophoresis |
Parameter |
Value |
Unit |
Hb |
12 |
g/dL |
WBC count |
10.5 |
/cumm |
MCV |
75.2 |
fl |
MCH |
24.6 |
pg |
MCHC |
32.8 |
g/dl |
Platelet count |
353000 |
Ul |
Serum Creatinine |
0.6 |
mg/dl |
SGPT |
57 |
mg/dl |
Total Cholesterol |
195 |
mg/dl |
HDL |
41 |
mg/dl |
LDL |
117 |
mg/dl |
VLDL |
37 |
mg/dl |
Triglyceride |
185 |
mg/dl |
Blood glucose |
236 |
mg/dl |
HbA1C |
2.9 |
% |
Falsely decreased HbA1c |
Falsely increased HbA1c |
Physiological |
|
Pregnancy in II trimester |
Pregnancy III trimester, Hypertriglyceridemia, Hyperbilirubinemia |
Hemoglobinopathy |
|
Hemoglobin variants ( Thal trait, HbE etc) |
|
OtherPathology |
|
Splenomegaly |
Asplenia, Chronic liver disease, Renal insufficiency, uremia |
RBC disorder |
|
RBC transfusion |
Anemia – Defective erythropoiesis (Vit B12, Folate, Iron deficiency) |
Drug intake |
|
Vitamin C ingestion |
Chronic alcohol consumption, Chronic salicylate ingestion, Chronic opiod ingestion, Lead poisoining, Dapsone, Ribavarin |




































