Open Access
Research Article
Max Screen
ISSN: 2455-7641
Copyright: © 2022 Mei Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Bloodstream infections(BSI) are one of severe infectious complications faced by hematopoietic stem cell transplantation(HSCT) patients. BSI increases significantly the morbidity and mortality of HSCT patients. Gram-positive bacteria occurred more frequency than gram-negative bacteria over past decades, but rates of gram-negative bloodstream infections have recently increased again. Antibacterial prophylaxis could be justified in HSCT, but infections caused by resistant pathogens increased mortality. New antibiotics such as omadacycline, meropenem/vaborbactam, eravacycline, ceftobiprole, tedizolid, dalbavancin, cefiderocol hold promise for the treatment of highly resistant pathogens.
Keywords: bloodstream infections; hematopoietic stem cell transplantation; bacteremia; drug resistant; novel antibiotics
Abbreviations: BSI : bloodstream infections; HSCT:hematopoietic stem cell transplantation; CVC : central venous catheter; AD : alternative donor; FQ: fluoroquinolones; TMP-SMZ:trimethoprim-sulfamethoxazole; MDR:multiple-drug resistant; MDROs: multi-drug resistant organisms; MRD: matched related donor; MSSA: methicillin-susceptible staphylococcus aureus; MRSA: methicillin-resistant staphylococcus aureus; ESBL:extended-spectrum β-lactamase-producing; VRE :vancomycin-resistant enterococcus; FDA :Food and Drug Administration; ABSSSI :acute bacterial skin and skin structure infections; CABP: community-acquired bacterial pneumonia; UTI:urinary tract infections; ECR: early clinical response; IACR: investigator-assessed clinical response ; PTE: post-treatment evaluation; EOT : end of treatment; CRE: carbapenem-resistant enterobacteriaceae; TOC: test of cure; AE: adverse events; cUTI :complicated urinary tract infection ; ITT: intent-to-treat; APN:acute pyelonephritis; ESBL :extended-spectrum β-lactamase; cIAIs: complicated intra-abdominal infections; LRTIs:lower respiratory tract infections; HAP :hospital-acquired pneumonia; CAP:community-acquired pneumonia; IE :infective endocarditis; SoC: standard-of-care ; cSSSI :complicated skin and skin-structure infection
Hematopoietic stem cell transplantation (HSCT) is only the treatment to cure or improve many hematological malignancies but recipients are at high risk of bacterial, fungal, viral, and parasitic infections. Bloodstream infections (BSI) is a serious complication of HSCT, especially in pre-engraftment phase. The incidence and mortality rates of BSI rang from 12% to 46.2% and from 4.0% to 41.5%, respectively [1,2]. The most common clinical symptoms of BSI are fever (>38 °C), chills, hypotension and increasing in white blood cell count and inflammation markers [3].
Many risk factors have been associated with the development of BSI in HSCT recipients. Patient-related risk factors are advanced age, comorbidities, lower functional capacity and high-risk hematological diseases. The post-HSCT period includes the pre-engraftment, the early and late post-engraftment phase. During the pre-engraftment period, the incidence of bacteremia is similar in both auto-and allo-HSCT recipients. Neutropenia and mucositis probably represent the main risk factors. The greatest incidence of bacteremia is observed in pre-engraftment period, when mucositis is more severe [4]. Contamination of hematopoietic stem cell grafts is also a risk factor for the development of bacteremia [5,6]. The contamination rate of hematopoietic stem cell grafts is approximately 1%. The risk factors of infection in the early post-engraftment phase are central venous catheter (CVC), graft-versus-host disease (GVHD)-related organ damage and its treatment, and lack of immune reconstitution[7]. The proportion of patients who develop bacteremia depends on the type of HSCT, the presence and severity of acute or chronic GVHD. Generally, there are higher infection for patients receiving HSCT from alternative donor (AD) than matched related donor (MRD) [8]. During the late post-engraftment phase, incompetent humoral and cellular immunity resulting from GVHD predisposes to encapsulated pathogen-associated infections.
The epidemiology of BSI has changed substantially. During the 1960s and 1970s, gram-negative pathogens predominantly caused BSI. Starting in the 1980s, this tendency shifted towards Gram-positive bacteria because of more frequent usage of CVC and antimicrobial prophylaxis. Nevertheless, during the last two decades, several centers in Europe and the United States reported higher proportions of Gram-negative BSI, which have replaced Gram-positive bacteria as leading pathogens. The study of ONKO-KISS showed the allo-and auto-HSCT patients developed BSI were 61.6%, 38.4%, respectively. BSI caused by Escherichia coli in allo-HSCT patients increased from 1.1% in 2002 to 3.8% in 2014, and Enterococci increased from 1.8% to 3.3%. Coagulase-negative staphylococci decreased in allo-HSCT patients from 8.2% to 5.1% and in auto-HSCT patients from 7.7% to 2.0%. No significant difference was observed in methicillin-resistant staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE) or extended-spectrum β-lactamase-producing (ESBL) enterobacteriaceae [9]. The most common Gram-negative and Gram-positive bacteria of BSI were Escherichia coli (20.5%), Klebsiella pneumoniae (17.07%), Coagulase-negative staphylococcus (CoNS, 17.07%), Viridans streptococci (14.63%), Staphylococcus aureus (20.7%), Escherichiacoli (20.5%), Pseudomonas aeruginosa(PA) (5.3%), and Enterococcus faecalis (5.2%). Other major species were Staphylococcus aureus (9.75%), Pseudomonas aeruginosa (7.31%), Acinetobacter baumannii(4.87%), Enterobacter cloacae (4.87%), and Proteus mirabilis (4.87%)[10-11].
It is well-known that HSCT recipients undergo frequently bacterial infections because of prolonging neutropenia. If the duration of neutropenia (absolute neutrophil count < 100/μl) in HSCT recipients is more than 7 days, prophylactic antibiotics can be considered. Fluoroquinolones (FQ)prophylaxis is recommended routinely by most expert guidelines [12]. However, prophylactic efficacy is reduced when the fluoroquinolone resistance rate of Gram-negative bacteria exceeds 20% [13]. Trimethoprim-sulfamethoxazole (TMP-SMZ) and cephalosporin are attractive alternative to FQs for antibacterial prophylaxis. Compared with FQs, patients who received TMP-SMZ have no significant differences in all-cause or infection-related mortality, febrile episodes or bacteremia [14]. Allo-HSCT recipients who received cefpodoxime had a similar incidence of neutropenic fever, multidrug-resistant and Pseudomonas aeruginosa infections in comparison to those who received levofloxacin [15].
The usage of broad-spectrum empirical antibiotics has decreased the mortality of febrile neutropenic in HSCT recipients, but the incidence of infections with multi-drug resistant organisms (MDROs) is increasing globally [16]. Multi-resistant bacteria are commonly MRSA, VRE, ESBL, carbapenemase-producing enterobacteriaceae (CRE), metallo-ß-lactamase-producing bacteria (MBL) .Main risk factors for resistant bacterial infections are advanced age (≥65 years), exposure to antibiotics, severe mucositis, open skin lesions, enteral feeding, skin GVHD, colonisation with VRE on hospital admission, Clostridium difficile-associated diarrhea, presence of neutropenia more than 7 days and prolonged hospital stay (≥21 days) [17]. It is reported that 40.5% HSCT recipients are colonized with MDROs and 20% develop BSI with resistant bacteremia which is associated with increased mortality [18]. The treatment of these resistant organisms in HSCT recipients is very important. Several new antibiotics may be efficacy in recipients with resistant Gram-negative and Gram-positive infections.
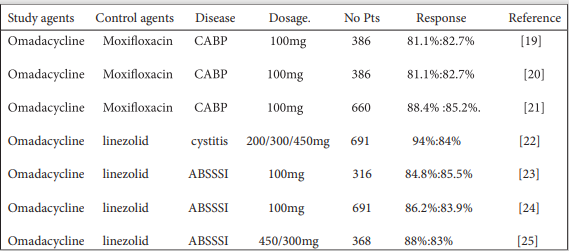
Omadacycline is a novel aminomethylcycline antibiotic developed by Paratek Pharmaceuticals. It is demonstrated that omadacycline possesses broad-spectrum antibacterial activity against Gram-positive, Gram-negative and drug-resistant bacteria such as Streptococcus pneumoniae, Enterobacterales, β-hemolytistreptococci, methicillin-susceptible staphylococcus aureus (MSSA), MRSA, VRE and Legionella pneumophila. In 2018, omadacycline was approved by the US Food and Drug Administration (FDA) for the treatment of patients with acute bacterial skin and skin structure infections (ABSSSI), community-acquired bacterial pneumonia (CABP) and urinary tract infections (UTI). The efficacy and safety of omadacycline and moxifloxacin were compared in CABP patients. In a double-blind trial, a total of 386 CABP patients were administrated with omadacycline at 100 mg intravenously every 12 hours(q12h), then 100mg every 24 hours(qd) and 388 patients received the treatment of mosifloxacin at 400mg intravenously qd. The early clinical response (ECR) was 81.1% in omadacycline group and 82.7% in moxifloxacin group. The rates of investigator-assessed clinical response were 87.6% and 85.1%, respectively. Adverse events (AE) were reported in 41.1% and 48.5% of the patients in two groups; the most frequent events were gastrointestinal, diarrhea. 8 patients in the omadacycline group and 4 patients in the moxifloxacin group were deaths [19]. Ramirez JA, et al had same results as Stets R, et al in ECR and similar numbers of patients achieved clinical stability [20]. Omadacycline was evaluated in investigator-assessed clinical response (IACR) at post-treatment evaluation (PTE, 5-10 days after last dose). Numbers of 660 patients were randomized as PORT risk class III and IV. The clinical success rates were 88.4%, 85.2% and 92.5%, 90.5%, respectively. PTE and clinical success rates of two groups were similar against identified pathogens and across key subgroups [21]. The efficacy of omadacycline in 31 women with cystitis was conducted. Patients received three doses of omadacycline for 5 days. Investigator-determined clinical success was observed in 94% and 84% of patients at end of treatment (EOT) and PTE, respectively, with similar results across groups. The mean range urine of omadacycline was 17.94 to 48.12 μg/ml at day 5. The most common adverse events were generally mild and transient gastrointestinal sides [22]. Furthermore, omadacycline was noninferior to linezolid in the treatment of ABSSSI [23-25]. Omadacycline was administrated orally at 300, 450, and 600 mg doses were well tolerated, but the 600 mg dose had more gastrointestinal adverse events [26]. Omadacycline at 100 mg and 300 mg doses had no effect on the QTc, PR and QRS intervals of electrocardiogram, but increased heart rate [27].
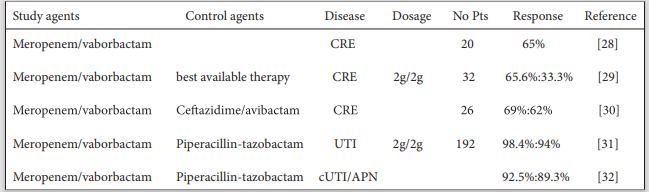
Meropenem/vaborbactam is an inhibitor of the combination carbapenem and beta-lactamase. CRE infections result in high clinical failure and mortality rates. The options for the treatment of CRE infections are limited. Meropenem/vaborbactam has a potential treatment for severe drug-resistant Gram-negative infections. Twenty patients with CRE received the treatment of mono-drug of meropenem/ vaborbactam. 30-day clinical success and survival rates were 65% and 90%, respectively. 35% patients had microbiologic failures within 90 days. One patient developed a recurrent infection due to meropenem/vaborbactam nonsusceptible[28]. TANGO II showed that the efficacy/safety of meropenem/vaborbactam were better than best available therapy (BAT, mono/combination therapy with polymyxins, carbapenems, aminoglycosides, tigecycline; or ceftazidime-avibactam alone) for CRE. The cure rates were 65.6% and 33.3% at EOTand 59.4% and 26.7% at test of cure (TOC). All-cause mortality of 28 days was 15.6% and 33.3% between groups. Treatment-related AE and renal-related AE were 24.0%,4.0% in meropenem/vaborbactam group and 44.0%, 24.0% in BAT group [29]. Meropenem/vaborbactam was compared with ceftazidime/avibactam in patients with CRE infections. The clinical success of patients in meropenem/vaborbactam group (62%) is similar with those in ceftazidime/avibactam group (69%). The mortality of 30- and 90-day and rates of AE were not different between groups. But there were more patients in the ceftazidime/avibactam group received combination therapy than patients in the meropenem/vaborbactam group (61%,15%) [30]. Furthermore, meropenem/vaborbactam was also evaluated in complicated urinary tract infection (cUTI). 550 patients (≥18 years) were enrolled and were randomized 1:1 to receive meropenem/vaborbactam or piperacillin/tazobactam every 8 hours. overall success occurred in 98.4% with meropenem/vaborbactam and 94.0% with piperacillin-tazobactam. Microbial eradication in the microbiologic modified intent-to-treat (ITT) population and in the microbiologic evaluable population were 66.7%, 57.7% and 66.3%, 60.4%in two groups and AE was similar [31]. In another trial, the clinical cure rates were microbiological eradication at EOT and TOC in meropenem/vaborbactam group were non-inferior to piperacillin/tazobactam group. The similar result was observed in the subgroup of patients with cUTI/ acute pyelonephritis (APN) [32].
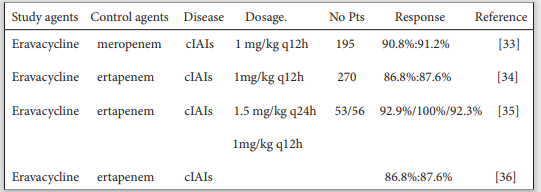
Eravacycline is a novel, fully synthetic fluorocycline with broad spectrum of activity against resistant Gram-negative, Gram-positive aerobic, facultative bacteria and multidrug resistance bacteria including ESBL. Eravacycline was proved for the treatment of complicated intra-abdominal infections (cIAIs). Compared with meropenem in a prospective, randomized, double-blind trial, eravacycline was noninferior to meropenem in cIAI patients and infections caused by resistant pathogens. The clinical cure rates in the primary end point were 90.8% in eravacycline group and 91.2% in meropenem group; The clinical cure rates in secondary endpoints were 92.4%,91.6% and the clinically evaluable population were 96.9% and 96.1% in both groups. In patients with ESBL, clinical cure rates were 87.5% and 84.6%, respectively. Patient with the treatment of eravacycline had relatively lower AE than those patients with meropenem [33]. The efficacy and the safety of eravacycline were also compared with ertapenem. When cIAI patients were randomized to receive eravacycline 1.0 mg/kg q12 h, or ertapenem 1.0 g qd, for a minimum of four 24-hour dosing cycles. The rates of clinical cure were 86.8% in the eravacycline group and 87.6% in the ertapenem group [34]. In another phase 2 study, 53 patients received eravacycline at 1.5 mg/kg q24h, 56 received eravacycline at 1.0 mg/kg q12h, and 30 received ertapenem at 1 g qd for a minimum of 4 days and a maximum of 14 days. The clinical success rate at the TOC visit was 92.9% in the group receiving eravacycline at 1.5 mg/ kg q24h, 100% in the group receiving eravacycline at 1.0 mg/kg q12h, and 92.3% in the ertapenem group. The incidences of treatment-emergent adverse events were 35.8%, 28.6%, and 26.7%, respectively. Incidence rates of nausea and vomiting were low in both eravacycline groups [35]. For the treatment of ESBL and CRE-expressing organisms. The clinical cure rates were 86.8% and 87.6% in eravacycline and ertapenem groups [36].
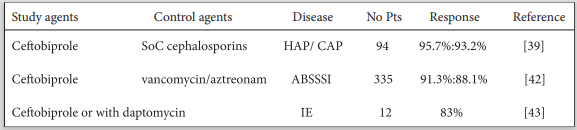
Ceftobiprole is a novel broad-spectrum antibiotics. Gram-positive pathogens such as Streptococcus pneumoniae, Coagulase-negative staphylococci, Enterococcus faecalis , Staphylococcus aureus , Gram-negative pathogens including Escherichia coli, Pseudomonas aeruginosa, Klebsiella pneumoniae but not ESBL, haemophilus influenzae , moraxella catarrhalis were susceptible to ceftobiprole[37]. In vitro, MSSA, MRSA and Gram-negative bacteria of community-onset or hospital-onset lower respiratory tract infections (LRTIs) were also inhibited by ceftobiprole [38]. Ceftobiprole is an effective and well-tolerated treatment for hospital-acquired pneumonia (HAP) excluding ventilator-associated pneumonia, community-acquired pneumonia (CAP), ABSSSI and infective endocarditis (IE). A multicenter phase 3 study demonstrated ceftobiprole has a similar efficacy to standard-of-care (SoC) cephalosporins in pediatric patients with HAP or CAP. 94 and 44 patients received ceftobiprole and SoC cephalosporin treatments, respectively. ECR rates at day 4 were 95.7%,93.2% and clinical cure rates were 90.4% and 97.7% in the ceftobiprole and SoC cephalosporins groups. Adverse and treatment-related AE were 20.2%, 8.5% and 18.2%,0% in two groups[39]. Previous studies show that ceftobiprole is an efficacious therapy for patients with pneumonia who are at high risk of poor outcomes. Two studies compared the efficacy of high-risk 398 CAP and 307 HAP patients with ceftobiprole or ceftriaxone ± linezolid treatment. The rate of early response was numerically higher in ceftobiprole-treated patients than ceftriaxone ± linezolid -treated patients. Ceftobiprole may have advantages over other antibiotics in terms of achieving early improvement in high-risk patients with HAP and CAP [40]. The efficacy and safety of ceftobiprole were also evaluated in 633 patients aged ≥65 years with ABSSSI, CAP and HAP. Findings were consistent with those for the overall study populations, although a trend toward improved outcomes was reported in some subgroups, patients aged ≥75 years with CAP were more likely to achieve ECR with ceftobiprole than comparator. The safety profile was similar between treatment groups in all studies [41]. A randomized, double-blind, active-controlled, parallel-group, multicenter, phase 3 study demonstrates ceftobiprole is noninferior to vancomycin/aztreonam in the treatment of ABSSSIs. 679 patients were randomized to ceftobiprole (n = 335) or vancomycin/aztreonam (n = 344). ECR rates were 91.3% and 88.1% in the ceftobiprole and vancomycin/aztreonam groups, respectively. Investigator-assessed clinical success at the TOC visit was similar between the two groups, and noninferiority was demonstrated for both the ITT (90.1% vs 89.0%) and clinically evaluable (97.9% vs 95.2%) populations. Both of groups had similar microbiological success and safety profiles [42]. Ceftobiprole in combination could be a promising alternative treatment.12 patients with IE treated with ceftobiprole (1 patient) or ceftobiprole and daptomycin (11 patients). All of patients were isolated with Gram-positive bacteria and 3 cases were polymicrobial. Cure rate was 83%. 9 /12 patients were switched to ceftobiprole because of the failure of previous antimicrobial regimen. 3/12 patients with persistently positive blood culture, bacteraemia was rapidly cleared after ceftobiprole administering [43].
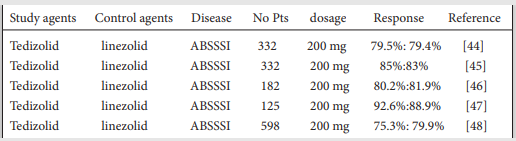
Tedizolid is a novel oxazolidinone antibacterial drug developed for the treatment of ABSSSI which are caused with Gram-positive pathogens. ABSSSI are composed of cellulitis or erysipelas, major cutaneous abscesses, and wound infections. ESTABLISH-1 was conducted to compare the efficacy and safety of tedizolid and linezolid for the treatment of ABSSSI in North America, Latin America, and Europe. 332 patients treated with a 200 mg once daily dose of oral tedizolid for 6 days and 335 patient received 600 mg of oral linezolid every 12 hours for 10 days. The early clinical treatment response rates were 79.5% in the tedizolid group and 79.4% in the linezolid group. The sustained clinical treatment response rates were 69.3%, 71.9%, respectively. Results of investigator-assessed clinical treatment success rates at a posttherapy evaluation visit were 85.5%, 86.0% in two groups [44]. ESTABLISH-2 was further to evaluate the efficacy of tedizolid administrated by intravenous with same doses of ESTABLISH-1. 85% patients in the tedizolid group achieved early clinical response which better than oral tedizolid. Gastrointestinal AE were less frequent with tedizolid (16%) than linezolid (20%).1 patient in the tedizolid group and 4 patients in the linezolid group were discontinued because of treatmentemergent AE [45]. The Latino patients treated with the same protocols of ESTABLISH-1 and -2 were to evaluate the efficacy and safety of tedizolid. The efficacy to tedizolid and linezolid at 48-72h in the ITT population were 80.2%, 81.9%. Sustained clinical success rates were 86.8% 88.9%, respectively. Tedizolid treatment was well tolerated in Latino patients and lower incidence of gastrointestinal AE without warranting dose adjustment [46]. Tedizolid was also investigated in Japanese, China, Taiwan, the Philippines, and the United States patients[47-48]. Tedizolid phosphate was noninferior to linezolid in clinical response and may be a reasonable alternative to linezolid for treating ABSSSI. Interestingly, a recipient of allo-HSCT infected with Nocardia novacomplex successfully treated with liposomal nebulized amikacin and tedizolid. The general condition of this patient has greatly improved and don’t relapse over 3-year follow-up [49].
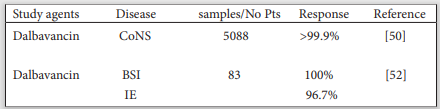
Dalbavancin is a lipoglycopeptide against Gram-positive bacteria in vitro activity. In Europe, it is approved for skin and soft tissue infections in adults. Dalbavancin is administrated with a single infusion of 1,500 mg or 1,000 mg followed one week later by 500 mg, repeated high doses are also effective and well tolerated. To evaluate the in vitro activity of dalbavancin compared with vancomycin, daptomycin and other agents in CoNS. A total of 5088 CoNS causing clinically significant infection were consecutively collected from 122 medical centers in the USA and Europe. Most isolates were from BSI (53.5%) or skin/skin structure infections (28.5%). Staphylococcus epidermidis was the most common species overall (54.6%) and for BSI (61.3%). The second most common species were Staphylococcus lugdunensis overall (12.3%) and Staphylococcus hominis for BSI (14.7%). Dalbavancin (DBV)inhibited >99.9% of CoNS isolates at ≤0.25 mg/L. All species were inhibited at ≤0.25 mg/L dalbavancin, except some Staphylococcus epidermidis (>99.9%) and Staphylococcus warneri (98.9%) isolates. Staphylococcus capitis and Staphylococcus simulans exhibited the lowest dalbavancin MIC50/90 values (0.015/0.03 mg/L) and Staphylococcus haemolyticus and staphylococcus saprophyticus the highest (MIC50/90, 0.06/0.12 mg/L) [50]. Dell’Orso et al. reported that an allo-HSCT recipient got Staphylococcus aureus liver abscess during pre-engraftment neutropenia and used dalbavancin to prevent the reactivation. A 1,500mg single dose of dalbavancin was administered and second dose administered after 15 days. Abdominal ultrasound after 50 days from HSCT did not show any significant hepatic lesion [51]. Finally, a multicentre, observational and retrospective study was conducted of 83 hospitalised patients with BSI and/or IE produced by Gram-positive cocci who received at least one dose of dalbavancin 59.04% had BSI and 49.04% IE. The most frequently isolated microorganism was Staphylococcus aureus in BSI (49%) and CoNS in IE (44.1%). All patients with IE were clinically cured in hospital; at 12 months, there was 2.9% loss to follow-up, 8.8% mortality unrelated to IE, and 2.9% therapeutic failure rate. The percentage effectiveness of dalbavancin to treat IE was 96.7%. The clinical cure rate for BSI was 100% during hospital stay and at 3 months; there were no recurrences or deaths during the follow-up. No patient discontinued treatment for AE [52].
Cefiderocol (S-649266), a new siderophore cephalosporin, has broad activity against enterobacteriaceae and non-fermenting bacteria, such as Pseudomonas aeruginosa and Acinetobacter baumannii, including CRE. A randomised, open-label, multicentre, parallelgroup, pathogen-focused, descriptive, phase 3 study in 95 hospitals in 16 countries in North America, South America, Europe, and Asia. Participants were randomly assigned 2:1to receive either a 3h intravenous infusion of cefiderocol 2 g every 8 h or best available therapy (a maximum of three drugs) for 7-14 days. For patients with nosocomial pneumonia, BSI or sepsis, clinical cure was achieved by 50%, 43% in the cefiderocol group and 53%, 43% in the best available therapy group; For patients with cUTIs, microbiological eradication was 53%,20%, respectively. In the safety population, treatment-emergent AE were noted for 91%of the cefiderocol group and 96% of the best available therapy group. 34 (34%) of 101 patients receiving cefiderocol and nine (18%) of 49 patients receiving best available therapy died [53]. The efficacy and safety of cefiderocol versus imipenem-cilastatin for the treatment of cUTIs were evaluated in patients at risk of multidrug-resistant Gram-negative infections. The primary efficacy endpoint was achieved by 183 (73%) of 252 patients in the cefiderocol group and 65 (55%) of 119 patients in the imipenem-cilastatin group, with an adjusted treatment difference of 18·58%, establishing the non-inferiority of cefiderocol. AE occurred in 41% patients in the cefiderocol group and 51% patients in the imipenem-cilastatin group, with gastrointestinal disorders the most common AE for both treatment groups 12%patients in the cefiderocol group and 18% patients in the imipenem-cilastatin group [54]. The efficacy and safety of cefiderocol versus high-dose, extended-infusion meropenem for adults with nosocomial pneumonia were conducted. Of 292 patients in the modified ITT population, 251 (86%) had a qualifying baseline Gram-negative pathogen, including Klebsiella pneumoniae (92 [32%]), Pseudomonas aeruginosa (48 [16%]), Acinetobacter baumannii (47 [16%]), and Escherichia coli (41 [14%]). All-cause mortality at day 14 was 12.4% with cefiderocol and 11.6% with meropenem. Treatment-emergent AE were reported in 88% participants in the cefiderocol group and 86% in the meropenem group. The most common treatment-emergent AE was urinary tract infection in the cefiderocol group and hypokalaemia in the meropenem group. Two participants (1%) of 148 in the cefiderocol group and two (1%) of 150 in the meropenem group discontinued the study because of drug-related AE [55].
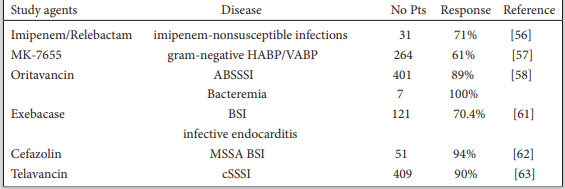
Imipenem combined with the β-lactamase inhibitor relebactam has broad antibacterial activity, including against carbapenemresistant Gram-negative pathogens. We evaluated imipenem/relebactam for treating imipenem-nonsusceptible infections. In randomized, controlled, double-blind, phase 3 trial, hospitalized patients with hospital-acquired/ventilator-associated pneumonia(HABP/VABP), complicated intraabdominal infection, or cUTI caused by imipenem-nonsusceptible (but colistin- and imipenem/relebactam-susceptible) pathogens were randomized 2:1 to 5-21 days imipenem/relebactam or colistin+imipenem. 31 patients received imipenem/relebactam and 16 colistin+imipenem. Pseudomonas aeruginosa (77%), Klebsiella spp (16%), other Enterobacteriaceae (6%). Favorable overall response was observed in 71% imipenem/relebactam and 70% colistin+imipenem patients, day 28 favorable clinical response in 71% and 40%, and 28-day mortality in 10% and 30%, respectively. Serious AE occurred in 10% of imipenem/relebactam and 31% of colistin+ imipenem patients, drug-related AE in 16% and 31% (no drug-related deaths), and treatment-emergent nephrotoxicity in 10% and 56%, respectively [56]. A randomized, controlled, double-blind phase 3 trial evaluated efficacy and safety of imipenem/cilastatin/relebactam (MK-7655) in treating HABP/VABP. Adults with HABP/VABP were randomized 1:1 to imipenem/cilastatin/relebactam 500 mg/500 mg/250 mg or piperacillin/tazobactam 4 g/500 mg, intravenously every 6 hours for 7-14 days. Of 537 randomized patients (from 113 hospitals in 27 countries). The most common baseline pathogens were Klebsiella pneumoniae (25.6%) and Pseudomonas aeruginosa (18.9%). Imipenem/cilastatin/relebactam was noninferior (P < .001) to piperacillin/tazobactam for both endpoints: day 28 all-cause mortality was 15.9% with imipenem/cilastatin/relebactam and 21.3% with piperacillin/tazobactam, and favorable clinical response at early follow-up was 61.0% and 55.8%, respectively. Serious AE occurred in 26.7% of imipenem/cilastatin/relebactam and 32.0% of piperacillin/tazobactam patients; AE leading to treatment discontinuation in 5.6% and 8.2%, respectively; and drug-related AE (none fatal) in 11.7% and 9.7%, respectively [57].
Oritavancin(ORI) is a long-acting lipoglycopeptide antibiotic with bactericidal activity against Gram-positive pathogens, including MRSA. The largest multicenter, retrospective, observational study in patients who received ORI for the treatment of ABSSSI and other Gram-positive pathogens infections. Clinical success in evaluable patients receiving at least 1 dose of ORI was 88.1%. In a subgroup of patients who received ORI for skin and soft tissue infections (n = 401) and bacteremia (n = 7), clinical success was achieved in 89.0% and 100%, respectively. A cohort of 32 patients received 2-10 ORI doses separated by no more than 14 days for complicated GP infections. Clinical success was observed in 30 of 32 patients (93.8%), including 10 of 11 (90.9%) patients with bone and joint infections and 7 of 8 (87.5%) patients with osteomyelitis. In the safety evaluable population, the overall rate of AE was 6.6% [58]. SOLO I and SOLO II were conducted that a single 1,200-mg dose of ORI was well tolerated and had a safety profile similar to that of twice-daily vancomycin in ABSSSI patients. The incidences of adverse events, serious AE, and discontinuations due to AE were similar for ORI (55.3, 5.8, and 3.7%, respectively) and vancomycin (56.9, 5.9, and 4.2%, respectively). The median time to onset and the duration of AE were also similar between the two groups. The most frequently reported events were nausea, headache, and vomiting. Greater than 90% of all events were mild or moderate in severity. There were slightly more infections and infestations, abscesses or cellulitis, and hepatic and cardiac adverse events in the ORI group; however, more than 80% of these events were mild or moderate and did not identify clinically meaningful differences [59]. The phase 3 studies of SOLO I and SOLO II demonstrated both ORI and vancomycin achieved similarly high rates of clinical response by pathogen, including MSSA and MRSA provides a singledose alternative to 7-10 days of twice-daily vancomycin to treat ABSSSI [60].
Exebacase, a first-in-class antistaphylococcal lysin, is a direct lytic agent that is rapidly bacteriolytic, eradicates biofilms, and synergizes with antibiotics. In a superiority-design study, 121 patients with S. aureus BSI/endocarditis receive a single dose of exebacase or placebo. All patients received standard-of-care antibiotics. Clinical responder rates on day 14 were 70.4% and 60.0% in the exebacase + antibiotics and antibiotics-alone groups, respectively, and were 42.8 percentage points higher in the prespecified exploratory MRSA subgroup. Rates of AE were similar in both groups. No AE of hypersensitivity to exebacase were reported. 30-day all-cause mortality rates were 9.7% and 12.8% in the exebacase + antibiotics and antibiotics-alone groups, respectively, with a notable difference in MRSA patients (3.7% vs. 25.0%) [61].
This study compared safety and effectiveness of nafcillin (NAF) versus cefazolin (CFZ) for MSSA BSI. A total of 130 patients receiving NAF (n = 79) or CFZ (n = 51) were included for safety analysis. Clinical success was achieved in 82% NAF and 94% CFZ treated patients (p = 0.1). NAF was associated with a higher incidence of nephrotoxicity compared to CFZ (25% vs. 2%), allergic reactions and a trend for hepatotoxicity. CFZ was associated with less nephrotoxicity and no difference in clinical success compared to NAF for MSSA BSI [62].
The clinical cure and microbiological eradication rates were 90% (368/409) and 89% (366/409) for telavancin-treated patients, and were similar for patients with methicillin-susceptible and -resistant Staphylococcus aureus isolates and Staphylococcus aureus isolates with elevated vancomycin MICs (≥1μg/mL)[63].
Many HSCT patients have high risk of poor outcomes because of BSI. Although antibacterial prophylaxis decreased obviously the number of infections of HSCT patients in the past, the trend of Gram-negative bacteria infection is increasing. Novel antibiotics could be a promising alternative treatment for BSI, HAP, CAP, ABSSSI, CABP, UTI, CRE and cIAIs. Omadacycline, meropenem/ vaborbactam, eravacycline, ceftobiprole are well tolerated and demonstrate similar efficacy to comparator.

![]()