Open Access
Research Article
Max Screen
ISSN: 2455-7641
Copyright: © 2021 Daltro PB. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Analyze the clinical profile of the spine with osteonecrosis in sickle cell disease. 610 patients were followed-up in this study between 2000 and 2017. 98 osteonecrosis were identified, 48 in the lumbar spine, 40 in the thoracic spine and 10 in both spine segments. We analyzed sex, age, genotype, and pain. Magnetic resonances and radiographs of the spine were performed. The patients were classified by the Verbal / numeric pain scale and functional pain scale according to Denis scale, 1983. We found that during the acute phase of bone infarction, the pain is severe and there is a progressive reduction in pain with drug treatment during the 1st week, progressing to moderate or mild pain in the 2nd week. All patients had severe pain in the acute phase lasting 2 weeks, moderate pain between the 3rd and 6th weeks, evolving to mitigation after the 7th week. 28 patients suffered recurrent pain at 12 months. In our study, we observed lesions in the thoracic, lumbar, and thoracolumbar regions with wide vertebral involvement and major pain crises, in addition to irradiation of pain and reduced spinal movements.
Keywords: Sickle Cell Disease; Spine; Osteonecrosis; Pain
Sickle cell disease (SCD) is a type of hemoglobinopathy characterized by the presence of hemoglobin S (HbS). It has a higher prevalence in people of African descent and a variable prevalence between countries. In the USA, for example, the heterozygous genotype called sickle cell trait is found in 10% of the population. In sub-Saharan Africa, the sickle cell trait has a prevalence of 10 to 45%. In Nigeria, for example, the prevalence of people with sickle cell trait is around 20 to 30% [1]. In Brazil, its prevalence varies from 6% in the southeast region to 15.7% in the state of Bahia. Sickle cell anemia is an autosomal recessive disease and can be associated with other hemoglobinopathies, especially HbSC, causing a chronic disease marked by progressive vaso-occlusion and degeneration of blood vessels [2,3].
In sickle cell disease, sickle-shaped red blood cells cause vascular occlusion, leading to tissue ischemia and infarction, known as vascular occlusive crisis (VOC) [4]. Patients with SCD have vaso-occlusive crises that can be triggered by cold weather, hypoxia, infection, dehydration, stress, and pregnancy. The inflammatory or hypoxic triggering factors leads to changes in red blood cells, which causes the polymerization of hemoglobin S, resulting in sickled cells. The interaction between sickle cell, leukocytes and vascular endothelium causes a cascade that promotes vasocclusion along the affected endothelium. Vasocclusion and hemolysis lead to damage to various systems in the form of acute pain crisis, acute chest syndrome, changes in splenic function, nephropathy, osteonecrosis, and neurological complications such as stroke. In addition, vasoocclusion and hemolysis can result in several musculoskeletal complications such as pain crisis, osteonecrosis, and infections [5,6].
Patients with sickle cell anemia are at increased risk of developing spinal pathologies such as vertebral osteomyelitis, compression fracture, vertebral vaso-occlusive crises, and osteoporosis. Spine pathologies in different studies are identified and prevalent. Spinal hyperplasia secondary to chronic hemolysis results in changes in skeletal conformation are seen in long bones and spine. In the spine, the softening and collapse of the final plaque results in changes in the concavity resulting in the H-shaped vertebrae seen on simple radiographs [7].
The pathophysiology of the formation of vertebrae in H; can be explained by the ischemia of the growing middle plate and the concomitant growth of adjacent secondary ossification centers [8]. Damage occurs in the central area of the vertebra and the external areas of the plaques are maintained. There are different arteries that supply the different areas of the vertebrae. Blood is offered to the central vertebra by the long branches of the vertebral nutrient artery and the small perforating branches of the periosteum vessels supply blood to the peripheral areas. [9].
Blood vessel occlusion and destructive events occur mainly in the longer vessels than in the shorter ones. The difficulty in supplying oxygen and nutrients leads to the development of avascular osteonecrosis, alteration of the architecture of the vertebra, softening and modification of its shape [10]. In contrast, the short perforating arteries of periosteal vessels serve the peripheral region of the growth plate. These vessels are rich in oxygen and therefore the peripheral end plate continues to grow at a normal rate, while growth is inhibited towards the center. This results in the distinct and well-defined “H” conformation of the vertebral bodies [5].
This work was approved by the Committee of Ethics in Research of the Hospital Universitário Professor Edgard Santos in Salvador, Bahia, Brazil. Inclusion criteria were patients treated in our institution with osteonecrosis in the lumbar and/or thoracic spine. Exclusion criteria were patients with immunosuppressive drug therapy, metabolic disease, or neoplastic disease.
The sample composed of 610 patients from 2000 to 2017 presented 98 osteonecrosis, 48 in the lumbar spine, 40 in the thoracic spine and 10 in both spine segments. Of these, 68 patients were female and 30 male, 46 patients with SC genotype and 52 SS genotypes with ages ranging from 20 to 40 years. Verbal / numerical rating scale (VRS and NRS) from 1 to 10 in the numerical scale, associated with the verbal scale described as, painless, minimal pain, moderate pain and severe pain, was assessed from patients during medical appointments [11] and functional pain scale was done according to Denis, 1983 [12]. All patients had severe pain in the acute phase lasting 2 weeks, moderate pain between the 3rd and 6th weeks, evolving to attenuation after the 7th week, 28 patients suffered recurrent pain at 12 months. Imaging exams were magnetic resonance imaging (MRI), anteroposterior, lateral, and oblique radiographs, making it possible to visualize the intervertebral canal and disc, pedicles, relationships, and morphologies of the intervertebral structures. Data were descriptively skewed through absolute numbers, frequencies, and percentages (Figure 2).
Interrogating and assessing pain, in the thoracic and lumbar spine of patients with sickle cell disease, requires not only an interpretation of musculoskeletal but also visceral pain. Chest pain is often evidence of the occurrence of cardiac disorders, but also might come as a result of bone involvement. The large network of fibers and nerve endings with the sensory and visceral innervation of the chest is wide. Back pain is a common symptom in patients with sickle cell anemia accompanied by osteonecrosis of the thoracic spine, as well as irradiation to distant organs or joints of the upper limb and ribs. In the acute phase of bone infarction, the pain is severe, which progressively decreases with drug treatment during the first week, progressing to moderate or mild pain in the fourth week. During clinical evaluation patients with homozygous presented increased severity of symptoms and pain in both thoracic and lumbar spine compared to SC patients. The majority of these cases are presented in the active age of these patients, with elevated pain being present in their 20 to 30 years. Homozygous hemoglobin are seen together with severity of pain in sickle cell disease.
The radiographic findings reflect depression of the vertebral planes of the vertebral bodies. The “H” shaped vertebra is characteristic of sickle cell anemia, seen in approximately 10% of the patients (Figure 3B and 4). This outcome is seen due to microvascular endplate infarction (Figure 1). In contrast to the rounded concavities seen in osteoporotic “fish-like” vertebrae (Figure 3B), the vertebral planes exhibit a step-like indentation.
All 40 patients with back pain, osteonecrosis and bone infarctions, presented severe pain in the acute phase with irradiation to the shoulders and ribs, progressing to mild pain after the fourth week.
48 patients, with acute low back pain secondary to osteonecrosis and bone infarctions, experienced severe pain, sudden onset, described as burning, shock or throbbing starting in the lumbar spine, more precisely in the affected vertebra, radiating to the lower limb, worsening with the movements of the lumbar spine (Figure 5). This clinical condition evolved at the end of 4 weeks for mild localized pain and return to painless with analgesic application and postural re-education. The 10 patients who presented bone lesions in two vertebral segments (lumbar and thoracic) experienced both forms of clinical manifestations.
People diagnosed with sickle cell disease can develop spinal osteonecrosis. These findings occur frequently and, when present, determine the appearance of signs on characteristic imaging tests [5]. In this work we show spinal X-ray and MRI images of SCD patients with osteonecrosis, osteoporosis leading to H shaped vertebra, which we may attribute to bone infarction. Pain levels were assessed to understand the impact of the bone anatomical modification. We found that the impairment of the vertebral body impacts the support of body weight and local innervations, causing fatigue and pain, which can radiate to the regions of the limbs, chest and viscera. Pain severity is evidenced in homozygous patients. Analgesic application and postural re-education mitigated after four weeks pain levels for more than half of the SS and SC treated patients.
Other groups noticed spinal involvement in SCD patients. Ntagiopoulos et al. (2006) presented a case report of a 58-year-old patient with sickle cell disease who presented the sign of the “fish vertebra” in lumbar vertebrae to the radiological examination [8]. The sign of the fish vertebra develops as biconcave lumbar vertebrae with bone softening. This was verified in the lateral and posterior-anterior radiographs of the spine performed on the patient. The observational study conducted by Miller et al. (2001) with 116 patients (50 children and 66 adults) aged between 3 months and 57 years, found that there was involvement of the thoracic vertebrae and these were in the form of H [13]. In the study carried out, there was no difference between adults and children when comparing bone findings in specific H vertebrae and avascular necrosis of the humeral heads. In our study, we found H-shaped vertebrae in the thoracic and lumbar spines and prevalence in the lumbar thoracic transition.
Balogun et al. (2010) conducted a study with 318 patients aged between 1 and 45 years confirmed with sickle cell anemia for 1 year. Musculoskeletal pathologies, anatomical sites, degree of disease, age at presentation were evaluated. About 37.4% had osteomyelitis, 21.4% developed osteonecrosis, and septic arthritis in 15.3% of patients. It was found that the presence of osteonecrosis in the older age groups with a frequency of 26%. The sites of involvement were the lower limbs in 71% of patients and spinal injuries were rare, being only 0.9%. In this study, the type of spinal involvement was not established [14].
In this study we showed 10% of SCD patients had H-shaped vertebra and reported, radiating back pain. Ohara, et al. (2012) conducted a descriptive study with 27 patients who were aged over 18 years and sickle cell disease in the form HbSS (85.20%), in the form HbSC (7.40%,) and HbSβ (7.40 %) [15]. The study shows that SCD can have repercussions on the spine, since bone infarctions can reach the central regions of the vertebral plateaus, leading to excess growth in the adjacent regions, giving rise to the “H-vertebra”, in which there is central depression plateaus [15]. The level of involvement of the spine has not been defined. Adewoyin (2015) carried out a review on the etiopathogenesis, clinical manifestations and treatment of sickle cell disease in Nigeria [1]. Avascular osteonecrosis of the femoral and humeral head is present in a patient with sickle cell anemia. In adults, who have suffered vertebral infarction and collapse, loss of height occurs. The H-vertebra is the musculoskeletal complication present in these patients and occurs due to the infarction of the vertebral body, giving the shape of a fish mouth present in the radiographs.
Amiri, et al. (2016), followed up 16 adolescent patients with sickle cell disease to determine the pattern of musculoskeletal impairment for 2 years. The age of the adolescents was 12 and 17 years old. Avascular necrosis was present in 37,5% of the adolescents monitored and the femoral head and humerus were the main sites of necrosis. Stress fractures and vertebral collapse were observed in 12,5% of patients. In the observational studies evaluated, it appears that osteonecrosis in the spine of patients with sickle cell disease affected patients older than 18 years. It was found that the studies cited the spine, but did not define the level of involvement of the spine and those who defined it had the lumbar spine as the main region affected by osteonecrosis and the presence of osteonecrosis of the femoral head was reported in most studies [16].
Kosaraju V. et al. (2017) carried out a review of the pathophysiology and the main imaging findings related to the complications of sickle cell disease. In this article, H-shaped vertebrae were cited as the main musculoskeletal complication of sickle cell disease. Vertebral growth can be affected by ischemia of the central vertebral growth plate, resulting in H-shaped vertebrae due to depression of the ends of the vertebral plaques, and sometimes formation of “tower” vertebrae with increased vertebral height without an corresponding increase in circumference. In the vertebral bodies, the configuration of the fish vertebrae can be seen in which the end plates form a soft concave shape [17]. In our study, we show that the spine is a site of involvement by osteonecrosis, the thoracic and lumbar spine being most often reported, with the formation of H-shaped vertebrae and also fish vertebra.
In conclusion, our studies, allowed us to observe thoracic, lumbar, and thoracolumbar lesions with wide vertebral involvement and major pain attacks, irradiation of pain and reduced spinal movements, osteoporosis and vertebral osteosclerosis in adult SCD patients. These outcomes are result of vascular impairment, a common outcome in SCD which probably resulted in vascular impact to the vertebral body, the most affected area seen in the presented images.
The authors declare that there is no conflict of interest regarding the publication of this article.
We would like to note the collaboration with the Hematology and Hemotherapy Foundation of Bahia – HEMOBA.

![]()

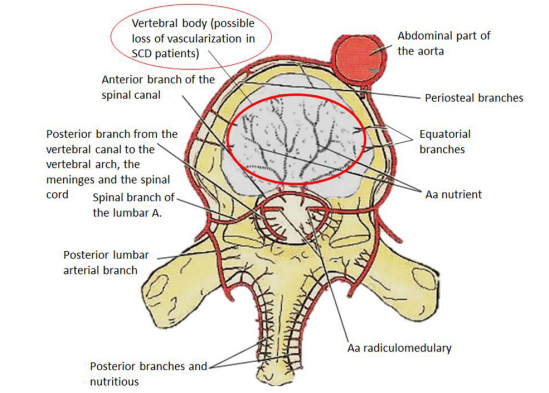 |
| Figure 1: Arterial vascularization of the vertebra, highlighting possible area of vascular impairment in SCD patients. Adapted from: Moore Anatomy 7th edition [9] |
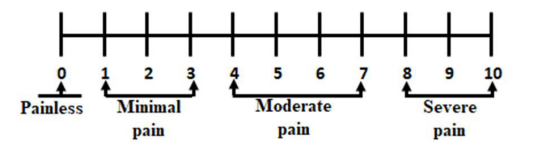 |
| Figure 2: Verbal / numerical rating scale |
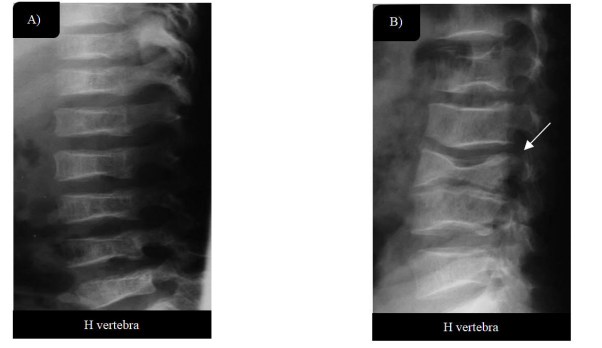 |
| Figure 3: X-rays of the spine in the lateral views, evaluating the structure and architecture of the spine, the conjugation foramina (A) Depression of the thoracic vertebral bodies, with decrease in bone density, a clear expression of osteoporosis; (B) Arrow pointing to lumbar H-shaped vertebrae |
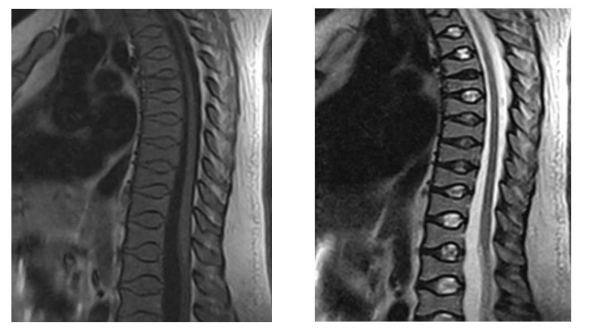 |
| Figure 4: Magnetic resonance image of the thoracic spine in the sagittal plane at T1 and T2 weightings, where the H aspect of the vertebral bodies is observed due to depression of the central portions of the vertebral plateaus usually seen in patients with sickle cell anemia |
 |
| Figure 5: X-ray images of the spine in lateral view showing sclerosis and bone infarctions in lombar vertebrae |
Score |
Pain scale criteria |
1 |
Painless |
2 |
Minimal pain without medication |
3 |
Moderate pain, with occasional use of medication |
4 |
Moderate to severe pain, with constant use of medication |
5 |
Severe pain, with chronic medication use |
|
Absolute numbers |
SS |
SC |
Hemoglobin genotype |
|
52 |
46 |
Age (Years) |
20-40 |
|
|
Osteonecrosis |
98 |
|
|
Lumbar spine |
48 |
23 |
25 |
Thoracic spine |
40 |
21 |
19 |
Both segments |
10 |
8 |
2 |
Female |
68 |
35 |
33 |
Verbal / numeric rating scale in admission |
|
|
|
Painless |
0 |
0 |
0 |
Minimal pain |
0 |
0 |
0 |
Moderate pain |
10 |
3 |
7 |
Severe pain |
88 |
49 |
39 |
Age |
SC Genotypes |
SS Genotypes |
20 to 30 years |
38 |
48 |
30 to 40 years |
08 |
04 |




































