Open Access
Research Article
Max Screen
ISSN: 2455-7641
Copyright: © 2021 Fall S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Introduction: In sub-Saharan Africa, few studies have integrated histological examination with immunostaining ; and our aim was to clarify the histoimmunochemical particularities of lymphoma diagnosed in adult.
Methods: A retrospective (September 2016 - December 2019) descriptive and analytical study concerned an exhaustive recruitment of patients followed at Clinical Haematology Department in Senegal for Hodgkin lymphoma (HL) or non- Hodgkin lymphoma (NHL) selected on the basis of a histoimmunochemical examination, epidemiological, diagnostic, therapeutic and evolutionary data were analysed.
Results: A total of 26 NHL patients (56.5%) and 20 LH cases (43.5%), aged 32-11 and 51-18 years respectively, were selected. Polyadenopathy was noted in 95% of cases of HL and 73.1% of cases of NHL (p=0.002). Patients were at Ann Arbor Stage II-IV in 80% of cases for the NHL and 70% of cases for HL (p: 0 ,317). Type B-Cell NHL entities were Diffuse Large Cell B Lymphoma (34.6%), Follicular Lymphoma (15.4%), Mantle Lymphoma (7.7%), Lymphocytic Lymphoma (7.7%), and Malt Lymphoma (3.8%). The NHL was type T-Cell in 30.8% of cases including 19.2% of anaplastic lymphoma. The HL were classic (80%) and nodular lymphocyte predominant Hodgkin lymphoma (20%). Specific treatment was performed in 82.6% of cases, 28.9% of which were immunochemotherapy. Remission was noted in 52.4% of NHL patients and 70.3% of those with HL.
Conclusion: Our study confirms the immunohistochemical diversity of lymphomas in patients receiving advanced stages of the disease, who have little access to targeted therapy. It remains to make available immunohistochemical and molecular explorations to better define the characteristics of lymphoma in africa.
Keywords: Non-Hodgkin’s Lymphoma; Hodgkin’s Lymphoma; Histoimmunolabelling; Africa
The prevalence of lymphomas is increasing in sub-Saharan Africa, but their incidence is unknown, given the difficulty of setting up a cancer registry [1,2]. The publications most often concern regional single-center or multicenter hospital studies [2-8]. In Senegal, NHL accounted for 45.4% of the causes of hospitalization related to hematologic malignancies [8]. Cytological and histological criteria without immunostaining are often used in the diagnosis of lymphomas from publications in black Africa [2]. This is linked to the difficulties in accessing the immunohsitochemical examination necessary for the WHO classification of natural lymphoid neoplasms [9]. The difficulties are linked to a lack of quality technical platforms on the one hand and staff training [1,2]. For this, initiatives have been developed with partnerships from advanced countries to make available complete pathological examinations, the basis of an objective classification, from which relevant data can be used [1,2]. In Senegal, immunohistochemistry is unavailable, and immunochemotherapy for hematologic malignancies is not subsidized. In sub-Saharan Africa, few of studies have integrated immunohistochemical arguments in the diagnosis of lymphomas [1-6]. We have therefore undertaken this work, with the aim of better specifying the pathological and evolutionary entities of lymphomas diagnosed in adults. The specific objectives were to describe the socio-epidemiological, diagnostic and therapeutic aspects and to determine the prognostic factors.
This is a descriptive retrospective study from September 1, 2016 to December 31, 2019 conducted at the Clinical Hematology Ser- vice of Dalal Jamm Hospital (Senegal) which is a reference center in Oncohematology. We carried out an exhaustive recruitment of patient files followed for Hodgkin lymphoma (HL) or non-Hodgkin lymphoma (NHL). The diagnosis of lymphoma was clinicaly suspected, then retained on pathological examination which included immunostaining data (immunochemistry, immunophe- notyping and / or fluorescence in situ hybridization) from tissue biopsy and / or organ sent by private laboratories in Senegal to dedicated Anatomy laboratories in France. The diagnosis of lymphoma was made on the basis of the 2016 WHO criteria [9]. The tumor mass was assessed using the Ann Arbor classification [10,11]. Depending on their financial situation, patients received in hospital or in outpatient either conventional chemotherapy: CHOP (Cyclophosphamide, doxorubicin, vincristine, Prednisone) COP (Cyclophosphamide, vincristine, Prednisone), ACVP (Bleomycin, Cyclophosphamide, doxorubicin, vincristine, Prednisone) ABVD (doxorubicin, bleomycin, Vinblastine, Decitabine), or immunochemotherapy (Rituximab and conventional chemothera- py).. The evolutionary data (clinical, computed tomography) were for the complete response (CR): disappearance of signs and mass and / or less than 1.5 cm, the uncertain complete response (UCR): residual mass greater than 1.5 cm or regression 75%, partial response (PR): less than 50% of tumor mass, stability (SD) and progression (PD): tumor evolution; according to Cheson’s criteria [12]. Remission included CR, UCR and PR.
Were analyzed the data, socio-epidemiological, diagnostic, anatomopathological subtypes of lymphoma, therapeutic and evolutionary. The Kaplan Meier survival curve was established. The analyzes were descriptive (mean, standard deviation; median with extremes, frequency) and analytical (Chi2 test considered significant for a p value< 0.05).
Out of a total of 63 files identified, 17 lymphomas that were proven only on histological examination were excluded and 46 retained records consisted of 26 NHL cases (56.5%) and 20 HL cases (43.5%).
Epidemiologically (Table 1) 90% of patients with HL and 38.4% of NHL cases are under the age of 45 (p: 0.1 10-3). The sex ratio was 1.22 for the HL and 0.85 for the NHL (p: 0.552). Symptoms at admission (Table 1) are alteration of the state general observed in 50% of patients who were in stage 3-4 of WHO. Cervical polyadenopathy was noted in 95% of HL cases and 73.1% of NHL cases (p: 0.002). Extranodal location was particularly cutaneous (23%), pleuropulmonary (11.5%) and digestive (7.6%) over the NHL. The comorbidities were hypertension (4 cases), diabetes (3 cases), viral hepatitis B co-infection (10 cases). None of our patients had HIV.
In histoimmunochemical analysis (Table 2), type B-cell NHL (B-NHL) are represented by diffuse large B cell lymphoma (DLBCL) in 34.6% of cases, follicular lymphoma (FL) in 15.4% of cases, mantle lymphoma in 7.7% of cases, lymphocytic lymphoma in 7,7% of cases and in Malt lymphoma in 3.8% of cases. DLBCL was a germinative centre in 33.3% of cases. The NHL was T- cell (T- NHL) in 30.8% of cases including 19.2% of anaplastic lymphoma.
Hodgkin lymphoma observations were labelled classic in 80% of cases and nodular lymphocyte predominant Hodgkin lymphoma in 20% of cases.
Prognostically, 80% of the NHL and 70% of the HL were at Stage III - IV of Ann ARBOR (p: 0.317). Specific treatment (Table 3) was performed in 82.6% of patients among whom 28.9% received immunochemotherapy. Remission was noted in 52.4% of NHL patients, 42.9% of whom were in complete reponse. Concerning the HL, the evolution was marked by 70.3% of remission including 41.2% of complète reponse. The median time to follow-up of patients was 888.7 days (37-1247 days). The median survival time was 852 days [37-1078 days] for DLBCL 864 days [597-1131 days] for FL, 305 days [124-486 days] for T-cell NHL and 1026 days [805 - 1247 days] for HL. The percentage of overall survival at 1 year, was 100% for FL, 85.6% for DLBCL, 82.3% for HL and 42% for T-cell NHL (Figure 1). At 3 year, overall survival was 78% for FL, 65% for HL and 43% for DLBCL, (Figure 1).
Lymphomas are dominated by the NHL which represented half in our series (56.5%), and nearly ninety percent (87.8%) of lym- phomas selected on cytohistological criteria in Togo [4]. The NHL is also the first mature lymphoid neoplasia in sub-Saharan Black Africa [3,5,6] and Magreb [7]. The NHL is diagnosed in the mid-fifties [2,3,6] in the African population, which is younger than the Western population [13]. In our study, HL is the least common entity, and it occurs in young adults (32 ± 11 years); which corroborates with certain african studies [2-6].
Revealing symptoms are dominated by polyadenopathy in our series (89.1%) and in Ndiaye et al [8] ( 75%) of Omoti et al [3] with 67.7% lymph node location. This nodal involvement is particularly cervical during HL [3,14]. Extranodal locations, such as skin, pleuro-pulmoaire and digestive, are much more described during the NHL [2], and are not uncommon in patients with HL [14]. In our regions, the difficulty to specify the primary or secondary extranodal NHL is linked on the one hand to the long delay of consultation responsible for the advanced stage of disease at diagnosis and on the other hand to a inefficent technical explorations platform [1,2].
Type B NHL immunohistochemical entities are dominated by DLBCL in our study (34.6%), as published by ElIdrissi et al [7] (47.5%). This finding is also made in a large series compiled in Sub-Saharan and Southern Africa which reported 48.8% of DLCBL [2]. Similarly in Europe, the DLBCL represents a fifth (40.9%) of the NHL [13]. It is most often a germinative centre type DLBCL [15]. Besides DLBCL, follicular lymphoma (FL) is the second immunohistochemical entity of NHL in our study, as described in sub-Saharan publications [3]. Lymphocytic lymphoma and Malt-type and marginal-zone lymphoma are the least common in our regions [3]. We do not have Burkitt lymphoma which is poorly reported in immunocompetent adult subjects in Senegal [8], as noted in our study. NHL with less represented T-cell than B-cell forms. T-cell NHL are also characterized by a diversity of immunohistochic forms dominated by anaplastic lymphoma [2]; This is also noted in our study. As for the NHL, the profile of HL entities is polymorphic, dominated by the classical type including nodular sclerosis with lymphocytic predominance [16], unlike nodular lymphocyte predominant Hodgkin lymphoma which is poorly reported [13].
On a prognosis basis, three-quarters of our patients were at an advanced stage of the disease; This is consistent with the findings of other publications [2,3]. This is due to the diagnostic delay related to the accessibility of responsible scans.
Therapeutically, we observe an underuse of immunotherapy, which results from the inaccessibility of immunophenotyping and molecular biolog [1,17], explaining in our patients the polymorphic evolutionary profile of B-cell NHL, which was better during FL. These difficulties of therapeutic access justify the use of ABVD during the advanced stages of HL, explaining the rate of complete reponse obtained by our patients.
Our study confirms the immunohistochemical diversity of lymphomas in patients receiving advanced stages of the disease, who have little access to targeted therapy that is not readily available. It remains to make available immunohistochemical and molecular explorations to better define the characteristics of lymphomas in Africa.
All authors declare to have no financial and personal relationships with other people or organizations that could inappropriately influence their work.

![]()

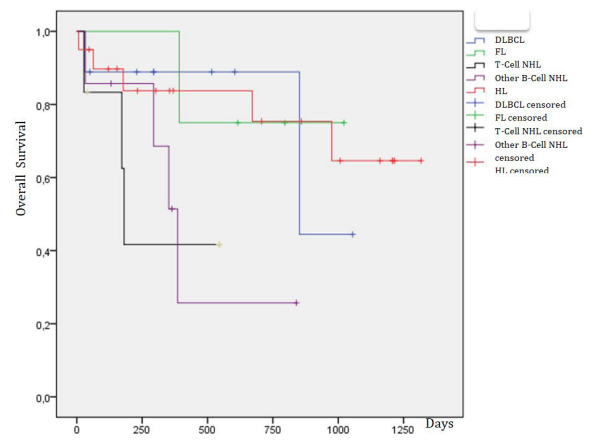 |
| Figure 1: Overall survival curve according type of lymphomas |
Signs |
Type of lymphoma |
P |
||||||||||||
HL |
NHL |
|||||||||||||
LN PL (N= |
SN (N= |
RL (N= |
CM (N= |
TN |
DL CL (N= |
FL N= (N= |
Mant (N= |
LL N= (N= |
Malt (N= |
T NHL (N= |
TN NHL (N = |
|||
Age (years ) |
M± SD |
36 |
33 |
33 |
30 |
32 ± |
52 |
53 |
62 |
63 |
40 |
42 |
51 |
0,01 |
[20-45[ |
3 |
10 |
4 |
1 |
18 |
3 |
1 |
|
|
|
6 |
10 |
||
[45-65[ |
0 |
0 |
0 |
0 |
0 |
2 |
3 |
1 |
2 |
|
1 |
9 |
||
>65 |
1 |
1 |
|
|
2 |
4 |
|
1 |
|
|
2 |
7 |
||
Gender |
H F |
2 |
7 |
1 |
1 |
11 |
5 |
1 |
1 |
1 |
1 |
|
12 |
0,55 |
Symptoms B* |
2 |
8 |
3 |
1 |
13 |
4 |
1 |
1 |
1 |
0 |
|
8 |
0,036 |
|
GA |
2 |
5 |
1 |
1 |
9 |
5 |
1 |
2 |
2 |
0 |
4 |
14 |
0,076 |
|
Lymph nodes |
cervical |
4 |
10 |
4 |
1 |
19 |
7 |
3 |
2 |
2 |
|
|
19 |
0,002 |
Axillary |
1 |
7 |
2 |
1 |
11 |
4 |
3 |
1 |
2 |
|
4 |
1 4 |
||
Inguinal |
2 |
5 |
1 |
1 |
9 |
4 |
1 |
1 |
1 |
|
4 |
11 |
||
Spléno |
1 |
0 |
0 |
1 |
2 |
|
|
|
|
1 |
|
1 |
_ |
|
Cutaneous |
0 |
0 |
0 |
0 |
0 |
1 |
|
|
|
|
5 |
6 |
_ |
|
Pleuro- |
0 |
1 |
0 |
0 |
1 |
2 |
1 |
|
|
|
|
3 |
|
|
Digestive |
0 |
0 |
0 |
0 |
0 |
1 |
|
|
|
|
1 |
2 |
_ |
|
Lymphoma type |
n /N (%) |
Immunohistochemical expression |
|
NHL (N= 26) |
|||
B-NHL |
DLBCL |
9 (34.6) |
CD20, CD3, CD79B, CD5,CD10, |
Follicular |
4 (15,4) |
CD20,CD79,CD10, BCL2, BCL6 |
|
Mantle lymphoma |
2 (7.7) |
CD20,CD79,CD5,CD10,MUM1 |
|
lymphocytic lymphoma |
2 (7.7) |
CD20, CD5,CD23,BCL2, MUM1 |
|
Malt lymphoma |
1 (3,8) |
CD20, CD79 |
|
T-NHL |
Anaplasic lymphoma |
5 (19, 3) |
CD3,CD30, CD4, CD5, EMA, ALK |
Lymphoblastic lymphoma |
2 (7.7) |
CD3,CD5,CD10, CD7, CD34, Ki67 |
|
Sezary lymphoma |
1 (3,8) |
CD20,CD5 |
|
HL (N=20) |
|||
Classic |
Rich in lymphocytes |
4 (20) |
CD20,CD30,CD15,CD3,CD79a |
Nodular sclerosis |
11 (55) |
CD30,CD15,CD3, EMA |
|
Mixed cellulary |
1 (5) |
CD20,CD30,CD3 |
|
Nodular lymphocyte |
4 (20) |
CD20, CD30,CD15,CD3,CD79a, |
|
Type of Lymphoma |
Protocol |
Total |
|||||
CVP |
CHOP |
RCHOP |
R |
ABVD |
R-ABVD |
|
|
NHL n (%) |
3(14,3) |
7 (33.3) |
7 (33.3) |
2 (9.5) |
2 (9.5) |
|
21 |
HL n (%) |
|
|
|
|
15(88.2) |
2 (11.8) |
17 |
|
Response to Treatment |
|
|||||
CR |
PR |
PD |
SD |
Death |
LS |
|
|
NHL n (%) |
9 (42.9) |
2 (9.5) |
2 (9.5) |
1 (4.8) |
3 (14,3) |
4 (19) |
21 |
HL n (%) |
7 (41,2) |
5 (29.4) |
1 (5.9) |
1 (5.9) |
0 ( 0 ) |
3 (17,7) |
17 |




































