Open Access
Research Article
Max Screen
ISSN: 2455-7641
Copyright: © 2021 Omunakwe HE. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: Thrombocytopenia is a reduction in the platelet count below the reference range of 150 x 109 /L. It is the second commonest hematologic disorder, following anaemia in pregnancy. Women with thrombocytopenia in pregnancy have a higher tendency to bleed; postpartum haemorrhage is a major cause of maternal mortality in our setting.
Aims: The aim of this study was to assess maternal thrombocytopenia at initiation of antenatal care in our facility, to determine the prevalence of thrombocytopenia in healthy mothers initiating antenatal care in our centre, assess the platelet indices and assess the severity of thrombocytopenia in women booking at different gestational ages.
Methods: This was a cross-sectional study, over a 6-month period. Women initiating antenatal care were assessed to know their age, parity, and gestational age at booking and 3ml of venous blood was collected in EDTA vacutainer. The platelet counts and assessment of platelet indices was done with Sysmex® Haematology analyser KX-21N.
Results: A total of 1147 pregnant women were included in the study, however 1130 had complete data that was analysed. They had a mean age of 31.6 ± 4.6 years. Their modal parity was para-1 (range 0-6), mean gestational age was 21.1 ± 7.6 weeks (range 4 – 40) weeks. The prevalence of thrombocytopaenia was 11.9%. The mean Platelet count was 214.8 x109/L (range 19 - 873), average Mean Platelet Volume was 10.5 ± 2.7fL, Mean Platelet Distribution Width was 13.5 ± 3.1fL. There was no significant difference in the mean platelet count for women booking in the first, second or third trimester, P= 0.109
Conclusion: The prevalence of thrombocytopaenia in women initiating antenatal care in our setting is high. It is important to screen pregnant women routinely for thrombocytopenia to identify those that will need support through pregnancy and avoid bleeding during parturition or after; post-partum haemorrhage remains a significant cause of maternal mortality in our setting.
Keywords: Thrombocytopenia; Pregnancy; Gestational thrombocytopenia
The platelet count usually ranges from 165–415 x 109/L in non-pregnant people [1]. Thrombocytopenia in pregnancy is a platelet count of below 150 x 109 /L [2]. It is usually responded to by haematologists and obstetricians; it is the second most common haematological disorder in pregnancy after anaemia [3]. Thrombocytopenia is seen in about 5-11% of all pregnancies [4]. Its assessment and management pose a great challenge to obstetricians because of its varied aetiologies. The causes could be pregnancy or non- pregnancy related. Pregnancy-related causes of thrombocytopenia include gestational thrombocytopenia, pre-eclampsia, and acute fatty liver of pregnancy. Non-pregnancy related causes include pseudothrombocytopenia, immune thrombocytopenic purpura and thrombotic thrombocytopenic purpura/haemolytic uremic syndrome. Others are autoimmune disorders such as systemic lupus erythematosus and antiphospholipid antibody syndrome, infections such as sepsis, HIV, Hepatitis B and C virus infections, disseminated intravascular coagulopathy, drug induced, bone marrow suppression, hypersplenism, von Willibrand disease type 2 and nutritional deficiency such as vitamin B12 and folate deficiencies.
Gestational thrombocytopenia is the most common cause of thrombocytopenia in pregnancy accounting for 70-80% of all cases. Hypertensive disorders of pregnancy account for up to 20% while immune thrombocytopenic purpura is seen in 3-4% of cases [5]. Thrombocytopenia is considered more frequent in multiple gestations compared to singleton pregnancies possibly because of PIH [6]. The remaining causes are rare in pregnancy. Causes of significant reduction in platelet count that require to be investigated include: thrombocytopenia which was present before conception, thrombocytopenia in the first two trimesters of pregnancy, platelet count < 75 x 109/L in the 3rd trimester or thrombocytopenia in case of pregnancy with complications [7].
There is paucity of literature on maternal thrombocytopaenia in our environment. Thrombocytopaenia in women initiating antenatal care has not been studied in our centre. This study is aimed at assessing maternal thrombocytopenia at initiation of antenatal care, to determine its prevalence and severity; assess platelet indices and the severity of thrombocytopenia in women booking at different gestational ages.
This was a cross-sectional study of all pregnant women initiating antenatal care at Rivers State University Teaching Hospital between February and June 2019. Their age, gestational age, and parity were documented using a study proforma. Baseline investigations including Full Blood Count and Platelet indices were done with EDTA blood collected by sterile methods using a vacutainer system. The samples were transported to the laboratory using a temperature-controlled carrier. The Sysmex® Haematology analyser KX-21N was used to assess the full blood count.
Severe thrombocytopenia was defined as counts < 50 x 109/L. 50-100 x 109/L was considered moderate thrombocytopenia and platelet count of 100-150 x 109/L was taken to be mild thrombocytopenia in this study.
Data was sorted, coded and analyzed using Statistical Package for Social Sciences (SPSS) IBM version 25.0 (Armonk, NY). Ethical approval for the study was received from the Ethics Committee.
A total of 1147 pregnant women were included in the study, however 1130 had complete data that was used for analysis. They had a mean age of 31.6 ± 4.6 years, 362 (32%) were less than 30 years old and 211(18.7%) were more than 35 years of age. Their modal parity was para-1 (range 0-6). Majority (53.3%) of the participants were primiparous women. The mean gestational age was 21.1 ± 7.6 weeks (range 4 – 40) weeks, only 68 (6%) initiated ANC by the 8th week of gestation. Table 1 shows the baseline characteristics of the study population.
Table 2 shows the grading or classification of platelet values. Of the 1130 women initiating antenatal care, 996 (88.1%) had normal platelet values while 134 (11. 9%) had thrombocytopaenia (Figure 1). One hundred and twelve (83.6%) women had mild thrombocytopenia while 18 (13.4%), and 4 (3%) had moderate and severe thrombocytopenia respectively. Of the 134 women with thrombocytopenia, 20 (15%), 71 (53%), 43 (32%) occurred in first, second and third trimesters respectively (Figure 2).
Table 3 shows the mean gestational age and blood cells. The mean Packed Cell Volume was 32.74% (range 11-46), the average White Cell count was 7.94 ± 0.63 X 109 /L, and the mean Platelet count was 214.8 ± 63.5 x109 /L (range 19 – 873). In women booking in the first trimester, the mean platelet count was 223.9 ± 74.9 x109 /L, in the second trimester 215.4 ± 59.0 x109 /L and in the third trimester 207.3 ± 63.1 x109 /L. The Mean Platelet Volume was 10.5 ± 2.7fL, Mean Platelet Distribution Width was 13.5 ± 3.1fL. There was no significant difference in the mean platelet count for women booking in the first, second or third trimester, P= 0.109. There was a weak negative correlation between the MPV and the different severities of thrombocytopenia (Pearson’s R- 0.115, P< 0.001). Table 4 shows no statistically significant association between grades of thrombocytopenia and the different trimesters of pregnancy [X2=2.913, p= 0.233 (95% confidence interval: 0.226, 0.243)].
The aim of this study was to determine the prevalence of thrombocytopenia in women initiating antenatal care at RSUTH, assess the platelet indices and the severity of thrombocytopenia in women booking at different gestational ages. The prevalence of thrombocytopenia in our study was 11.9%; like the report from Geneva [8], which had 11.6% and Pradesh, India [8] which had 11.4% of the women assessed presenting with thrombocytopenia. The prevalence of GT in our centre was however more than 8.4% reported by Chauhan et al [9] in Indian women and 7.7% in Addis Ababa [10]. However, it was less than 13.5% which was reported amongst pregnant women in Lagos [11]1 and 15.3% in Ghana [12].
The mean platelet count in our study was 214.9 ± 63.5 x 109 /L; similar to 212.74 ± 63.28 x 109 /L reported in another tertiary hospital in Port Harcourt [13] and higher than 193 ± 46 x 109 /L reported in Ibadan [14] and 204.48 ± 57 x 109 /L in a more recent study from Lagos Nigeria [15]. However, it was lower than 228.29 ± 65.6 x 109 /L reported in Lagos [16]2 and 222.38 ± 58 x 109 /L in Markudi [17]. There was no difference between the first, second and third trimester when the platelet count was considered like in other studies [18]. A study by Jesse et al [19] showed that the average platelet count in pregnant women reduced throughout pregnancy till term and counts < 100x109 /L in pregnant women may be due to some other causes apart from pregnancy itself.
Majority of the women (84%), had mild thrombocytopenia compared to moderate and severe thrombocytopenia. Classifying thrombocytopenia based on trimester of pregnancy, it was found that thrombocytopenia occurred most in second trimester followed by third trimester with least occurrence in first trimester (Figure 2). Although the platelet count decreased from first to third trimester, there was no difference in the mean platelet count across the trimesters of pregnancy p = 0.109. Our finding corroborates that of other studies [11,13,18]. Platelet is known to decrease with increasing gestational age due to increased consumptive coagulopathy especially in pregnancies complicated by preeclampsia/eclampsia, other forms of hypertensive disorders, HELLP Syndrome [8]. Gestational thrombocytopaenia could account for our finding in this present study population since most of the women initiating antenatal care had no medical condition complicating their pregnancies. However, a repeat platelet count at 6 weeks postpartum would be helpful in confirming the diagnosis of gestational thrombocytopaenia.
Also, from the present study there was no statistically significant association between grades of thrombocytopenia and the different trimesters of pregnancy (X2=2.913, p= 0.233).
A Pearson’s correlation was run to determine the relationship between mean platelet value and different grades of thrombocytopenia, a weak negative correlation was found and was statistically significant (r = -0.115, p < 0.001). The lower the older or mature platelet, the higher the mean platelet volume due to increase output of younger and lager platelets from the system. The mean platelet volume is an index of the average platelet size, and it increase as the bone marrow compensates for rapid consumption of platelet with release of younger and larger platelets.
Platelet lifespan reduces and the MPV increases slightly during pregnancy [20]. Increased MPV signifies increased platelet activation and in pregnancy may be due to impaired uteroplacental circulation [21]. The MPV is a precise measure of platelet size, it is considered a marker and determinant of platelet function. Large platelets would have higher MPV levels, are haemostatically more reactive and raise higher amounts of the prothrombotic factor thromboxane A 2, increasing the tendency to thrombosis [22].
The prevalence of thrombocytopenia in this group of women is 11.9%. It is important to screen pregnant women routinely for thrombocytopenia, to identify those that will need support through pregnancy and avoid bleeding complication during parturition or after; post-partum haemorrhage remains a significant cause of maternal mortality in our setting.

![]()

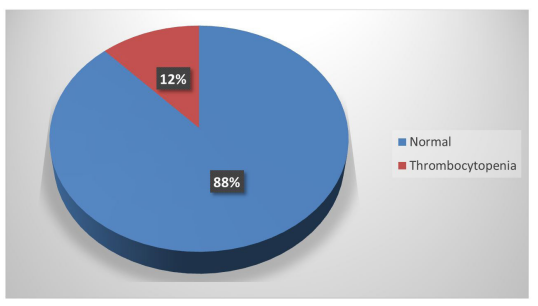 |
| Figure 1: Classification of platelet values of women initiating antenatal care |
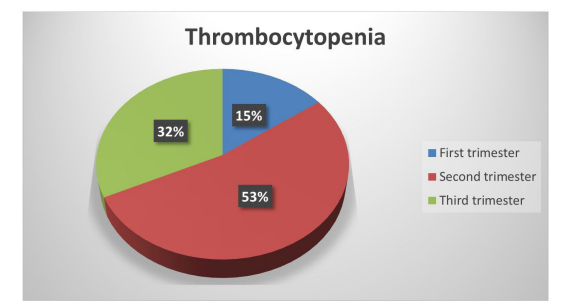 |
| Figure 2: Occurrence of thrombocytopenia according to the trimester of pregnancy |
Variable |
No. |
Percentage |
Age (years) |
|
|
15-19 |
7 |
0.6 |
20-24 |
61 |
5.4 |
25-29 |
294 |
26.0 |
30-34 |
470 |
41.6 |
35-39 |
244 |
21.6 |
40-44 |
48 |
4.2 |
45-49 |
6 |
0.5 |
Mean age (±SD) |
31.6 ±4.5 |
|
Total |
1130 |
100 |
Parity |
|
|
0 |
82 |
7.3 |
1 |
602 |
53.3 |
2 |
271 |
24.0 |
3 |
100 |
8.8 |
4 |
56 |
5.0 |
5 |
14 |
1.2 |
6 |
5 |
0.4 |
Total |
1130 |
100 |
Classification |
Frequency |
Percentage |
Normal platelet (> 150 X 103) |
996 |
88.1 |
Thrombocytopaenia |
134 |
11.9 |
Mild (100-149 × 103) |
112 |
9.9 |
Moderate (50-99 × 103) |
18 |
1.6 |
Severe (<50 × 103) |
4 |
0.4 |
Total |
1130 |
100 |
Variable |
Mean |
SD |
Gestational age (weeks) |
23 |
2.1 |
PCV* (%) |
32.8 |
3.1 |
WBC** (X 106) |
7.9 |
6.7 |
Platelets |
214.9 |
63.5 |
First trimester |
223.9 |
74.9 |
Second trimester |
215.4 |
59.0 |
Third trimester |
207.3 |
63.1 |
Platelet Volume (fL) |
10.5 |
2.7 |
Platelet distribution width (fL) |
13.5 |
3.1 |
|
Thrombocytopenia |
|
|
|
|
Trimester |
Yes |
No |
Total |
X2 |
p -value (95% CI*) |
First |
20 (9.6) |
189 (90.4) |
209 (100) |
2.913 |
0.233 (0.226,0.243) |
Second |
71(11.4) |
550 (88.6) |
621 (100) |
|
|
Third |
43(14.3) |
257 (85.7) |
300 (100) |
|
|
Total |
134 (11.9) |
996 (88.1) |
1130 (100) |
|
|




































