Open Access
Research Article
Max Screen
ISSN: 2454-3284
Copyright: © 2023 Brinderjeet Kaur. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Endometriosis is a estrogen-dependent disorder commonly found in pelvis or rare instances anywhere in the body. It is benign and has a chronic course. Complaints of pain, tender mass, cyclical association with menstrual cycle are almost pathognomonic. We present a rare presentation of endometriosis as vaginal wall cyst in a 32 year old female and without any clinical history of endometriosis either in past or present. The isolated presentation of endometriosis as a cyst in vagina is a rare presentation. The case is glaring example of occurrence of endometriosis at unusual extra uterine location. It is essential for gynecologists to keep endometriosis as differential diagnosis when encountering similar cysts in vaginal region.
Keywords: vaginal wall mass; endometriosis
Endometriosis is the presence of ectopic deposits of endometrial tissue. These deposits are typically present in the pelvis primarily in ovaries, pouch of douglas, broad ligaments, round ligament, uterosacral ligament, uterus, fallopian tubes and bowel. These account for > 96 % of endometriosis cases. Less common sites include abdominal wall, omentum, perineum, genitourinary sites ( ureters , bladder and utrethra ) cervix . Vagina accounts for only 0.02 % of cases. (1, 2).
A woman aged 32 years old presented to gynecology OPD with complaints of something coming out of vagina, sense of heaviness and discomfort in vaginal region especially during sitting for past 6 months.
There were no complains of pain during menses and no complains of difficulty in micturition or defecation. Her bowel and bladder habits were normal. She attained menarche at 13 years of age had normal menstrual history with no history dysmennorhoea, pelvic pain or abnormal intermenstrual bleeding. She had history of normal conceptions with two children and one missed abortion which was followed by dilatation and curettage done 6 years back. The first baby was delivered normally 8 years back and the second baby by cesarean section 7years back. The rest of medical history was unremarkable. She underwent sterilization about 6 years back. On examination her vitals were stable and on per vaginal examination a 5x4 cm circular non tender cyst was seen arising from the midportion of right anterior vaginal wall 2.5 cm away from the urethral orifice. The cyst was firm in consistency, fluctuant, could not be moved from side to side in horizontal plane or vertical. No clear demarcation could be found to its attachment to the anterior wall of the vagina. The previous Pap smear was normal.
In view of the presence of vaginal cyst the differential diagnosis included -inclusion cyst, leiomyoma , fibroepithelial polyp , haemangioma , condyloma , bartholian cyst , endometriosis, gartner’s duct cyst , urethral diverticulum and skene’s gland cyst.
Ultrasound was done (figure -1), which revealed normal sized uterus with endometrial thickness of 5 mm and a small cyst measuring 3x3 cm seen in the anterior vaginal wall. A MRI pelvis was done which revealed a 2.5x2.5x1.5 cm ovoid circumscribed non enhancing lesion in the mid upper vagina with intrinsically intense T1 hyperintensity (not simple fluid T2 signal) (figure -2a) and minimal T2 hyperintensity (figure -2b) and without any enhancement on post contrast sequences (figure -2c ) , consistent with a debris filled benign cyst .Patient was counseled to go for excision of the cyst followed by biopsy . But she did not turn up on the elective day.
After a gap of a month, the patient came prepared for the procedure. Relevant pre operative investigations were done, which included blood group, complete blood count, viral markers and the case was posted for removal of the anterior vaginal wall cyst. After general anesthesia, the patient was put in lithotomy position and under aseptic precautions posterior vaginal wall was retracted with sims speculum and a 5x4 cm big circular cyst was identified arising from the mid portion of anterior vaginal wall. On manipulation chocolate colored fluid came out the most dependent spot on the cyst (Figure 3-5). This was indicative of endometriotic nature of the cyst. By sharp and blunt dissection the entire cyst was removed with cyst wall intact (Figure -6) and the sample was sent for histopathological reporting. Haemostasis achieved and the vagina was reapproximated. Intra and post operative period was uneventful. Patient was given a dose of Inj Leuprolide 3.75 mg was given and discharged on same day. The report revealed endometrial gland, diffuse haemosiderin laden macrophages and fibrosis and no evidence of dysplasia or malignancy. The clinical suspicion of endometriosis was substantiated by the histopathology which proved that it was vaginal endometrioma.
The case report highlights the enigmatic nature of endometriosis. The diagnosis of endometriosis at this site is unexpected and rare. The presence of endometriosis outside the peritoneal cavity is surprising and its diagnosis is challenging without histological confirmation (3). Endometriosis can ‘masquerade ‘as several other conditions often misleading the diagnosis or delaying its confirmation. (4) However, the incidence of endometriosis at the site of vagina is a rare entity. The particular interest in this case report is isolated finding of vaginal endometrioma . There are cases were deep infiltrating endometriosis ( DIE ) infiltrates the vaginal wall and creates effects similar to our finding of vaginal endometrioma (5)
The pathogenesis of endometriosis remains controversial ( 6 , 7 ) and multifactorial. The implantation theory proposed by Sampson in 1972 remained the widely accepted one for long time. This theory proposed the lesions are secondary to implantation and proliferation of regurgitated endometrial cells in an ectopic position. Angio and lymphatic theory, impairment of immune system, heritable tendencies and secreted products of endometriotic lesions may contribute to explain the pathogenesis in some cases. (7,,8).From an anatomic point of view , two theories have been proposed . First is “ in situ “ development through coelomic metaplasia . Secound is endometrium dissemination in ectopic places by mechanisms like retrograde menstruation , lymphatic and / or vascular dissemination and direct endometrial invasion . According to modern theory of induction , endometriosis could be the end result of local metaplasia induced by the prescence of endometrium (9).Most authors agree with the endometrial origin of ectopia epithelium rather than the mesothelial one . However, lack of an univocal etiopathogenesis of endometriosis creates controversy – if endometriosis is a single disease or it represents group of different diseases with an etiology and histologic clinical aspects which re specific and independent . In present case the proposed etiology could be trauma during normal delivery and dilatation and curettage. Similar etiology has been proposed following trauma while performing cone biopsy, curettage, following use of electro cautery. (10) This ‘Iatrogenic implantation theory’ probably explains the endometriosis that develop through mechanical transpositions during surgery. (11). Another theory proposed is the immune reaction like transforming growthbfactor (TGFᵝ) , prostaglandin E2 , placental protein 14 or glycodelin (PP14) nad interlukein 10 . (12) . It is proposed an environment rich in these factors involved non specific suppression of the cell mediated immunity , well correlated with the defected activity performed by natural killer cells (NK ) at a local ;evel in endometriosis . (12)
Although the list of differentials of a vaginal mass may be exhaustive., a targeted history , examination and investigations are ideal to focus and histology to confirm the diagnosis.(13) A Gartner’s duct cyst represents mesonephric remnants and complicates diagnostic differentiation by location of the mass , as it can be found in the anterolateral vaginal wall . Urethral diverticulum is more proximal and post void leakage and milking of the urine from the urethra are more typical of an urethral diverticulum . Skene’s gland cyst is more distal.
Ultrasound being a reasonably accessible, non invasive, safe imaging modality is usually the initial investigation of choice. An endometrial cyst on Ultrasound may vary in appearance from a well defined hypoechoic masses to complex cystic structure. (14) Urethral diverticulum on ultrasound appear as anehoic or hypoechoic . MRI appears to be superior imaging modality. MR features are completely concordant with diagnosis of endometrioma . Blood products appear are usually T1 hyperintense and less T2 signal than simple fluid. Due to the prescence of the lesion in the vagina –an atypical location the MRI features only added to the confusion. It was learnt that urethral diverticulum in T1 images appear as decreased intensity and T2 hyperintense in stark contrast to lesions containing blood such as endometriotic cyst , skene’s duct with haemorrhage . (13)
We suggest that surgical intervention for both diagnosis and treatment of such cysts should be done. This should be performed in all cases to prevent recurrence and malignant transformation, which is rare but possible. (11,14) Being an isolated vaginal endometrioma medical management of endometriosis was given postoperatively to prevent recurrence. It involves hormonal therapy with the goal of decreasing local estrogen production. (1) This inhibits tissue proliferation and local inflammation at endometriotic implants.
The symptoms of endometriosis are of varied range. Endometriosis may be suspected in patient presenting with a swelling in the vagina. Vaginal implantation of endometrial tissue in areas which are less likely to be involved poses questions on etiology. We speculate operative procedures done vaginally may be the causative factors. The management recommended is surgical excision followed by medical management.
Nil
Nil

![]()

 |
| Figure 1: LUSG suggestive of 3x3 cm anterior wall cyst with differential of Gartner 's cyst or Bartholian cyst |
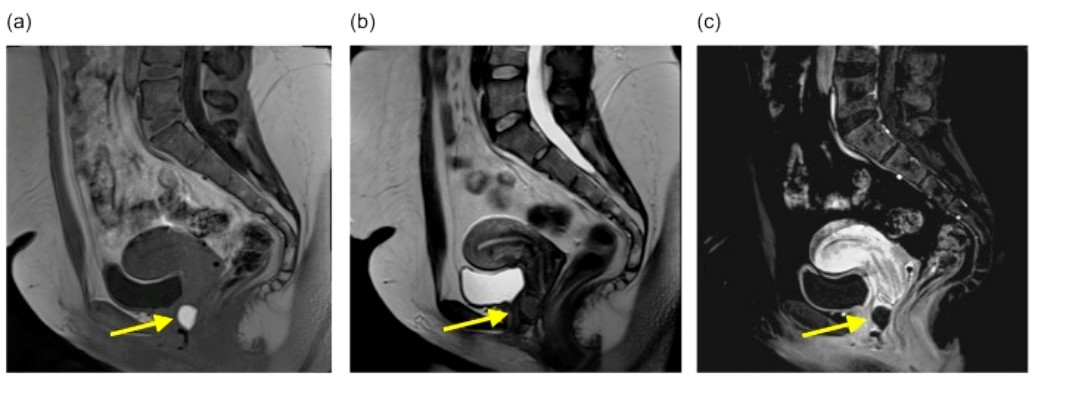 |
| Figure 2: MRI images a) hypertensity T1 weighted well circumscribed lesion in vagina typical of debris filled cystb) T2 only slight T2 hyper intenseC) T1 weighted post contrast substraction sequence likely benign cyst |
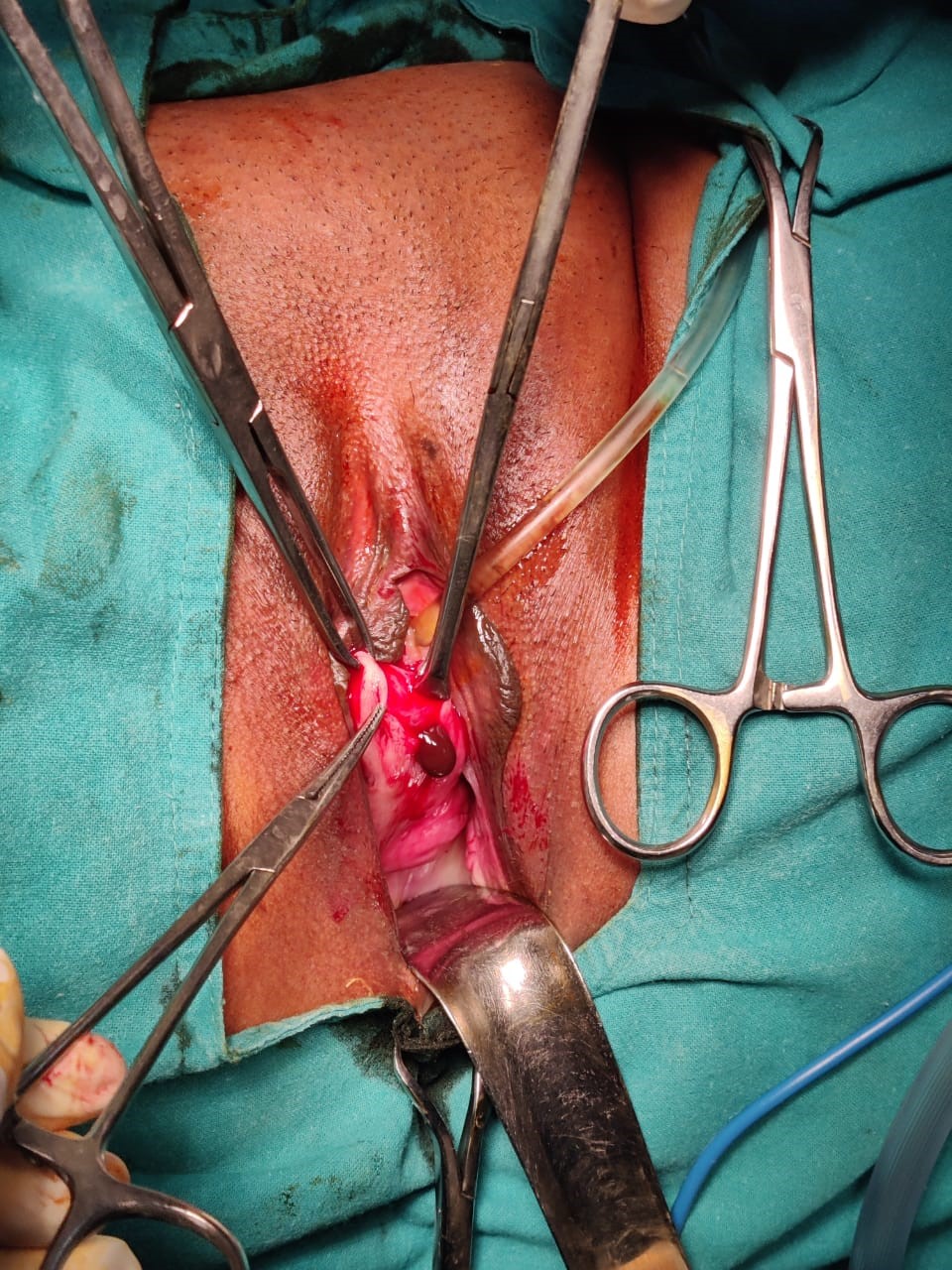 |
| Figure 3: chocolate colour fluid came out on manipulation of cyst |
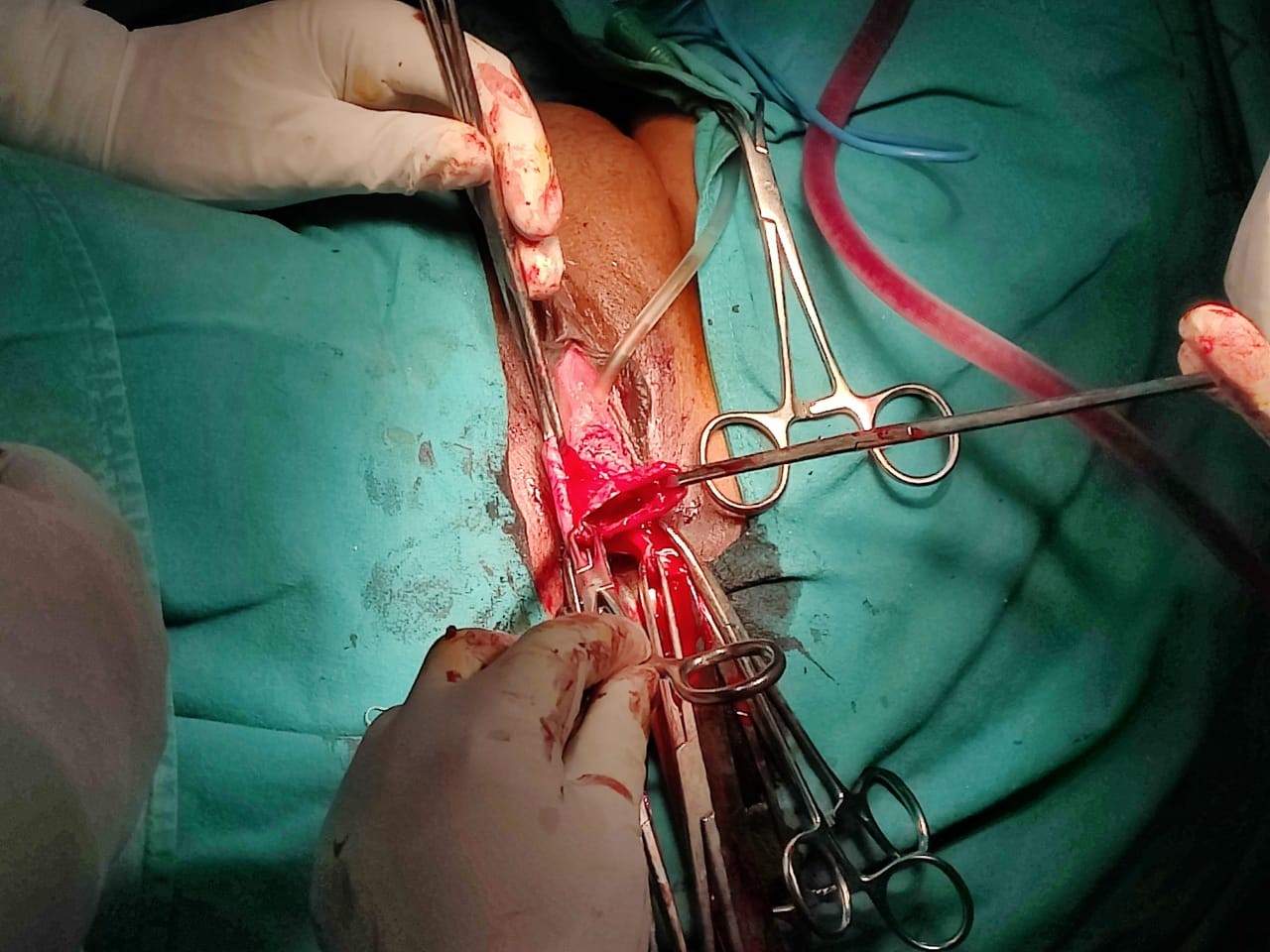 |
| Figure 4: Surgical removal of endometrial cyst done |
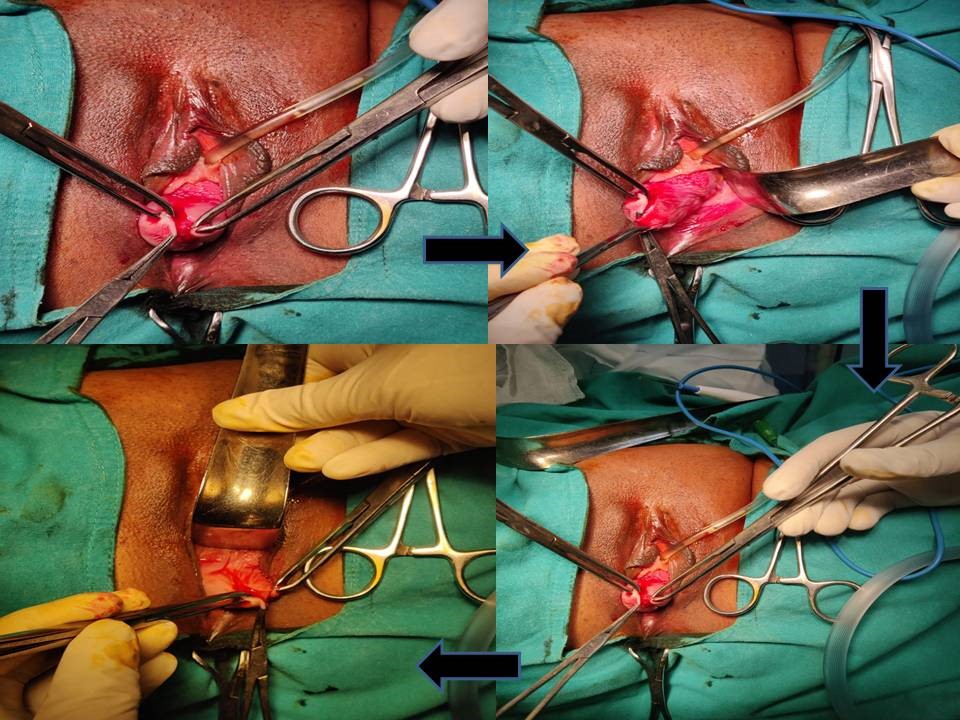 |
| Figure 5: Steps of removal of cyst |
 |
| Figure 6: Entire cyst wall removed and sent for HPE |




































