Open Access
Research Article
Max Screen
ISSN: 2454-3284
Copyright: © 2019 Somé DA. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Objective:To report a case of heterotopic pregnancy with ectopic egg location from a hypoplastic horn, raising diagnostic and therapeutic difficulties during its management.
Material and Methods:This was a descriptive study. Using one case study design, the case was seen in the Department of Gynecology, Obstetrics and Reproductive Medicine of Souro Sanou University teaching hospital (SSUTH), in Burkina Faso, on June 18, 2018. The observation made revealed the history of the patient, the clinical and preclinical signs, and data related to the treatment.
Results:A 28 year-old woman, parity two, consulted during her third pregnancy for pelvic pain without metrorrhagia. An ectopic pregnancy was suspected on clinical examination. An obstetrical ultrasound performed showed a heterotopic pregnancy with a normal intrauterine fetus of 13 weeks of amenorrhea (WA) and another intra-abdominal fetus that died at 24 WA. After performing laparotomy, it has been observed a malformed uterus with the residual right horn carrying the dead fetus. A mini incision was made to extract the egg and reveal a lack of communication between the residual horn and the pregnant uterus. During this heterotopic pregnancy, the fetuses had an age difference of 13 weeks with the first implantation of the ectopic egg. Then, she gave birth normally for the third time.
Conclusion:A heterotopic pregnancy with delayed fertilization and implantation for more than two months is exceptional. Difficult to be diagnosed, it required an emergency laparotomy to save the mother and the intra-uterine egg.
Keywords: Case Report; Heterotopic Pregnancy; Ultrasound; Laparotomy; Burkina Faso
List of abbreviations:ASRM: American Society of Reproductive Medicine; EGSE: European Society of Gynecologic Endoscopy; ESHRE: European Society of Human Reproduction and Embryology; JHPIEGO: Johns Hopkins Program for International Education in Gynecology and Obstetrics; SSUTH: Souro Sanou University Teaching Hospital; WA: Weeks of Amenorrhea
Prevalence of uterine malformations was 1 to 6.7% in the general population [1,2], 0.17% to 7.3% in infertile women [2-5] and 3.8% in fertile women[6,7]. A rudimentary horn pregnancy is estimated to occur in 1 of every 76,000 pregnancies [2]. Uterine hypoplasia/aplasia is responsible for 4% of malformations. A pregnancy in a rudimentary horn can be isolated or associated with another intrauterine implantation. This ectopic pregnancy is a life-threatening maternal pregnancy because the major risk is cataclysmic hemorrhage by rupture of the rudimentary horn during the first or second trimester of pregnancy [8], in which case it is exceptional that a live birth should occur [5]. Overall prevalence of pregnancies on rudimentary horns was 1/40 000 to 1/76 000 [3,4,9]. Heterotopic pregnancies had a frequency of 1/30000 to 1/100 [10,11]. The prevalence of those located in a hypoplastic horn is 1 case for 2 to 3 million pregnancies [10]. A ditopic pregnancy conceived successively at intervals of months, with implantation of the extra-uterine pregnancy in a rudimentary horn, is extremely rare. We found no publication about such a case in the literature consulted. The authors, in this study, focused on the diagnosis difficulties and the treatment given.
This was a descriptive study. Using one case study design, the case was seen in the Department of Gynecology, Obstetrics and Reproductive Medicine of Sourô Sanou University Teaching Hospital (SSUTH), in Burkina Faso, on June 18, 2018. The observation made revealed the history of the patient, the clinical and ultrasound signs, and data related to the treatment.
The patient was married, housewife, 27 years old and residing in rural area of Burkina Faso. She previously gave birth normally to two live children 9 and 6 years old. Menstruations returned 5 months after the last delivery and remained regular, once a month. She consulted at the District Hospital for pelvic pain and 2.5 months delay in menstruations. An ultrasound examination was prescribed for «suspicion of ectopic pregnancy and discordance between uterine size and the age of pregnancy».
An abdominal-pelvic ultrasound performed, concluded as follows: «single intrauterine evaluative pregnancy of 13 weeks of amenorrhea (WA) associated with an abdominal pregnancy non-evaluative since the age of 24 WA».
Patient’s general examination was normal. However, the obstetrical examination revealed an oblong abdominal mass which was more to the right side than to the left, bigger than what could be expected at the age of 13 years of pregnancy (Figure 1). There was no vaginal bleeding. The larger diameter of this abdominal mass (uterine height?) was 22 cm. The uterus had a soft consistency and a size smaller than the mass which corresponded to the right uterine horn.
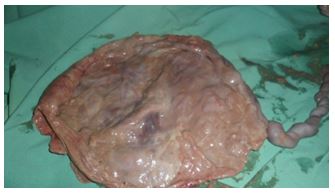
In view of the clinical and ultrasound results, the diagnosis of heterotopic pregnancy with abdominal location of the extrauterine one was retained and an emergency laparotomy indicated. At the coeliotomy, an enlarged uterus was discovered. Its right horn was oblong, larger than the uterus and of large transverse diameter giving the image of a bilobate uterus (Figure 2). The mass, measuring about 10 cm by 5 cm, was soft and fetal parts could be touched through its wall. This hypoplastic stump was in continuation in its medial portion with the right fallopian tube and ovary which, both appeared normal.
The patient got a pre-anesthetic visit on the same day and urgent laboratory tests were performed including blood group / rhesus system and blood count. Under a spinal anesthesia, incision of Pfannestiel was performed. After opening the abdominal cavity, was discovered a bilobate mass corresponding to gravid uterus and gravid rudimentary right horn (Figure 2). A 5 cm horizontal mini-hysterectomy was performed on this aplastic uterus (photo 3) to extract a dead female fetus (Figure 3 and 4) weighing 550g and a placenta (Figure 5 and 6), of 150g. There was no communication between uterus and this horn, but the mass was fine, with no visible decidua.
The horn’s wound was closed by a one plane suture using resorbable thread 2/0 followed by tubal sterilization using the Pomeroy technique [12]. Urinary tract exploration has been limited by the intrauterine evaluative pregnancy. The hemostasis being perfect, we closed the fascia with a simple over lock with an absorbable thread and then the skin with nylon. A histological examination of the dead fetus and placenta was requested but not accepted by the patient’s parents. No complications occurred after the operation. She then delivered a boy alive at the 38 WA by vaginal way at the SSUTH; this child is now 17 months old, well and apparently healthy.
Several classifications concern congenital anomalies of the female genital tract. Musset’s (1964) distinguishes 4 types of anomalies [13]. The most commonly used classification is the American Society of Reproductive Medicine (ASRM) classification (1988) [14]. The one established by the European Society of Human Reproduction and Embryology/ European Society of Gynecologic Endoscopy (ESHRE/EGSE) (2013), distinguishes three subgroups [15]. Our observation corresponds to a pseudo-unicorn uterus [16]. It is the atypical incomplete right unilateral uterine aplasia with Musset’s canaliculated horn [3]. It corresponds to ASRM classes IIb [1,4,17] and U4AC0V0 of ESHRE/EGSE [15].
Embryologically, the fallopian tubes, uterus and upper 2/3 of the vagina come from the Müller canals [4]. The formation of the genital tract begins as early as the sixth week of gestation and ends in the sixteenth week. A lack of caudal migration or incomplete migration of the canals to the urogenital sinus will result in complete or incomplete uterine atresia or aplasia [4]. Incomplete aplasia is thought could result from incomplete formation of the Müller canals before the tenth week of pregnancy. The reported malformation may be due to incomplete right unilateral mülllerian aplasia. In 83 to 90% of cases, the rudimentary horn is compartmentalized [8,18] but can carry a pregnancy [17]. The anomaly is on the right in 2/3 of the cases. The explanation would be the more caudal progression of the left Müller Canal compared to the right [3].
Migration of gonocytes or zygote was unusual. Propelled into the abdominal cavity, the oocyte is caught by one of the fallopian tubes [19]. Sperm cells that have migrated through the left fallopian tube escape into the abdominal cavity. They are sucked through the right tubal fringes; pass through the abdominal ostium; so fertilization of the oocyte can occur. Fertilization is also possible intraperitoneal and the egg is then sucked into the fallopian tube [19], in order to migrate to the blind cavity
The diagnosis of a rudimentary horn is difficult, often unexpected about pregnant woman with no evocative signs. The clinical picture is that of an ectopic pregnancy [20]. Standard ultrasound contributes little to diagnosis [8]. Its sensitivity is only 26% [20]. It makes it possible to diagnose 22% of cases during the gynecological period and 29% during pregnancy [5]. Indeed, ectopic pregnancy can simulate intrauterine pregnancy [21]. The best non-invasive examinations are magnetic resonance imaging and three-dimensional ultrasound, except for some risks of errors [22]. Their sensitivity is from 83 to 90% [1,22,23]. Unfortunately, they are expensive and their practice is not routine.
Confirmation of the intraoperative diagnosis justifies a hypoplastic uterine hysterectomy [5,24,25]. In gynecological periods or in case of complications, this attitude is systematic. However, some precautions should be taken when storing the egg in the normal uterus. Mobilization of the uterus should be minimal. While hysterectomy causes these uterine manipulations and can also create a cornual uterine scar. Leaving the rudimentary cavity in place will not participate in menstruation [19] because the existence of a cervix is essential for menstruation. To prevent further pregnancies in the rudimentary horn, hysterorraphy was supplemented by homolateral tubal sterilization.
The particularity of this heterotopic pregnancy is the coexistence of two pregnancies conceived months apart. The ectopic one housed in a hypoplasia horn makes the case exceptional and difficult to diagnose. The treatment should save the mother and the intrauterine fetus but also avoid the occurrence of pregnancy on rudimentary horn

![]()

 |
| Figure 1: Irregular abdominal pelvic mass |
 |
| Figure 2: Bilobal uterus |
 |
| Figure 3: Extraction of the dead fetus of 24WA from the rudimentary horn |
 |
| Figure 4: Fetus |
 |
| Figure 5: Placenta |
 |
| Figure 6: Hysterorraphy of the canaliculated horn |




































