Open Access
Research Article
Max Screen
ISSN: 2454-3284
Copyright: © 2019 Zhang Z. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Weight loss is an efficient therapy for obese polycystic ovary syndrome (PCOS) patients. Here we evaluate the effect of dietary weight reduction on clinical performance in obese PCOS patients. Medical records of fifty obese PCOS patients (age 27 ± 5 years) who had calorie-controlled dietary intervention were reviewed. The patients had a 1200-kcal/day diet until ovulation or for up to three months. Changes in body weight, body mass index (BMI), blood pressure, menstruation, acne, and hirsutusm, serum levels of endocrine hormones and adipocytokines, glucolipid metabolism index and insulin resistance were assessed. Menstrual cycle, ovulation and relapse in the following six months were also reviewed. All patients had menstrual disorder, 43 had acne, and 26 were hirsute. After weight loss, the BMI decreased from 27.89 ± 3.06 to 25.70 ± 2.42 kg/m2(p < 0.001). Acne and hirsutusm was improved in 39 and 14 patients, respectively. Regular menstruation was restored in 26 patients and lasted for 3.12 months on average. Endocrine hormones levels, adipocytokines levels, glucolipid metabolism and insulin resistance were shifted toward balance. Weight relapse was seen in 11 patients. No side effects occurred. Dietary intervention in obese PCOS patients can improve relevant clinical problems but weight relapse is an issue.
Keywords: Weight Loss; Polycystic Ovary Syndrome; Obesity; Calorie Controlled Diet
Polycystic ovary syndrome (PCOS) is a common disorder affecting 5%-10% of premenopausal women [1]. It is characterized by chronic absence of ovulation, amenorrhea or oligomenorrhea, infertility, obesity, hirsutism and ovarian cystic enlargement. An epidemiological survey shows that more than 50% of obese people suffer from PCOS, confirming obesity is a major risk factor [2]. The most important hormonal changes in obese patients include increase of androgens, insulin secretion and insulin resistance [3]. Insulin resistance plays an important role in the process of PCOS [4]. PCOS also increases the risk of other diseases such as diabetes, coronary artery disease, and endometrial carcinoma
Weight loss had been the first-line therapy for obese PCOS patients, which can block the vicious circle between obesity and endocrine metabolism, preventing long-term complications. Dietary intervention has been used to improve obesity. However, dietary therapy has been questioned and bariatric surgery and pharmacotherapy is proposed alternatively [5,6]. It has been showed gastric bypass surgery and its consequent weight loss in overweight PCOS patients can results in multiple clinical improvements [7]. Recent studies reveals dietary intervention has impact on gut microbial gene richness [8] and the richness of human gut microbiome is correlated with metabolic markers and is associated with obesity [9], suggesting dietary intervention may be still feasible. Therefore an assessment on the effect of dietary weight loss on clinical performance in obese PCOS patients is required.
In the study, we retrospectively reviewed the medical records of obese PCOS patients who had calorie controlled diet and compared the clinical manifestations, endocrine hormone levels, sugar and lipid metabolism and the cytokine levels before and after weight reduction. We attempt to evaluate the clinical feasibility of the implementation of dietary intervention (Figure 1).
This retrospective study was approved by the Ethics Committee of Hangzhou Obstetrics and Gynecology Hospital and written consent was obtained from all patients.
Medical records of obese PCOS patients who were diagnosed and had a dietary weight-loss treatment between January 2016 and January 2018 at Hangzhou Obstetrics and Gynecology Hospital were retrieved and reviewed. Fifty cases were enrolled. The included patients were all diagnosed according to Rotterdam criteria. The average age of the patients is 27 ± 5 years old. They all received a 1200-kcal/day diet until ovulation or for up to three months otherwise. Seven patients restored ovulation within three months. Their medical records also covered six-month follow-up. No medication that could affect sex hormone levels and glucolipid metabolism was taken throughout the diet treatment and the six-month following-up. Exclusion criteria were that BMI< 25kg/m2 , or the patient had any of the following diseases: congenital adrenal cortical hyperplasia, Cushing’s syndrome, tumors secretion of androgens, hyperprolactinemia, premature ovarian failure, hypothalamic amenorrhea, thyroid dysfunction or any other diseases that can cause hyperandrogenemia or cause ovulatory dysfunction (Figure 2).
We collected information for analyses including body weight, BMI, blood pressure, menstruation, hirsutusm, acne, ultrasonographic reports and blood test reports on serum levels of prolactin (PRL), estradiol (E2), luteinizing hormone (LH), follicle-stimulating hormone (FSH), total testosterone (TT), fasting blood-glucose (FBG), fasting insulin (FINS), total cholesterol (TC), triglycerides (TG), high density lipoprotein (HDL), low-density lipoprotein (LDL), apolipoprotein A-1 (Apo A-1), apolipoprotein B (Apo B), leptin (LEP), adiponectin (ADPN), dehydroepiandrosterone sulfate (DHEAS), sex hormone binding globulin (SHBG), lipoprotein a (Lp(a)), insulin-like growth factor 1 (IGF1), and insulin-like growth factor binding protein 3 (IGFBP3). We also reviewed patients’ insulin resistance homeostasis model assessment index (HOMA-IR) and free androgen index (FAI) for evaluation of insulin sensitivity and androgen activity, respectively. Attention was also paid on adverse effects of weight loss, such as gastrointestinal reaction, hypoglycemia, and syncope (Figure 3).
Statistical analyses were performed by SPSS 17.0. Data are presented as mean ± SD. Significance of difference were evaluated by t-test. Pearson correlation method was used for correlation analysis. A p-values < 0.05 was considered significant.
Clinical data before and after treatment were listed in Table 1. All included patients had menstrual disorder (1 polymenorrhea, 1 oligomenorrhea, and 48 amenorrhea or secondary amenorrhea). The incidences of acne and hirsutism were 86% (43/50), and 52% (26/50), respectively. Acne was mainly distributed on face, chest and back, and mostly associated with seborrheic dermatitis. Hirsutism was assessed by Ferriman-Gallwey score. Hard, long, and dark hair was commonly seen on the upper lip, chins, forearms, legs, thighs, ventral midline and around areola in hirsutism patients. However, after treatment, the BMI of the patients decreased from 27.89 ± 3.06 kg/m2 to 25.70 ± 2.42 kg/m2 (p < 0.001). 26 (52%) patients restored regular menstruation, which, however, was only lasted for 3.12 ± 0.65 months. 90.7% (39/43) of the patients improved acne. Improvement was defined by decreased quantity and seborrheic dermatitis disappearance and most improvements occurred on face. 53.85% (14/26) of patients improved hirsute with decreased score from 10.88 ± 2.36 to 8.65 ± 1.90 (p < 0.001). Improvements were mainly on ventral midline, crus. We also found hirsute improvement had a significant positive correlation with weight loss (r = 0.670, P = 0.000). The serum levels of androgens including luteinizing hormone (LH), total testosterone (TT), and dehydroepiandrosterone sulfate (DHEAS) decreased significantly (p < 0.05). Meanwhile, serum sex hormone binding globulin (SHBG) level increased (p < 0.05). In addition, the free androgen index (FAI) dropped (p < 0.05) significantly. The serum levels of insulin-like growth factor 1 (IGF1) decreased. The insulin resistance homeostasis model assessment index (HOMA-IR) decreased (Table 2). Meanwhile, serum levels of fasting insulin (FINS) and fasting blood-glucose (FBG) decreased significantly (p < 0.05). The decrease of serum leptin (LEP) level (p = 0.001) and increase of serum adiponectin (ADPN) was also (p < 0.05) significant (Table 3).
Numerous studies show obesity is a major risk factor for hypertension [10]. It has been suggested 1-kg weight loss can reduce 1-mmHg blood pressure [11]. There was one patient with hypertension. The blood pressure of the rest of the patients was in normal range and stably maintained. The low hypertension incidence in this study may be due to the young age (27 ± 5 years old) of the patients and the short course of PCOS. Here due to the small sample size of hypertension patients, correlation could not be performed. But the blood pressure of the hypertension patient declined from 142/95 mmHg to 135/88 mmHg after 6-kg weight loss, which is consistent with previous studies. Weight loss associated side effects were not seen in this study, suggesting the dietary treatment could be a feasible therapy method. The risk may be quantified based on a larger sample size. However, weight relapse was seen in 11 patients.
The improvement of menstrual disorder may be due to weight relapse as dietary intervention was stopped after treatment. Clinical practice has proved that most obese PCOS patients that lose about 5%- 10% body weight can obtain regular menstruation [12]. Here the patients with recovered menstrual period lost 8%-17% body weight, comparable to the previous description. Menstrual disorder of PCOS patients directly reflects the endocrine disorder, which suggests weight loss may improve endocrine disorder as well. The results also indicated weight loss can improve acne and hirsutism. Hyperandrogenemia is the main cause of acne and hirsute. Weight loss may reduce the biological activity of androgens and subcutaneous fat tissue, thus contributing to the improvements
SHBG, a steroid glycoprotein synthesized in the liver, can specifically bind to sex hormones and down regulate the biological activity of sex hormones. Body fat accumulation would reduce the level of SHBG gradually and raise the androgen levels consequently. FAI, LH, TT and DHEAS are closely related to hyperandrogenemia and insulin resistance [13-17]. The shift of androgen levels was in accord to the acne and hirsutism outcomes, confirming their roles of hyperandrogenemia in PCOS. The IGF1 pathway is involved in androgen synthesis and insulin resistance [18,19]. The shift of IGF1 and IGFBP3 levels confirmed the improvement of endocrine disorder and suggested the insulin resistance might be reduced. The changes in endocrine hormone levels are also consistent with the improvement of menstrual disorder.
Among PCOS patients, the incidences of impaired glucose tolerance and insulin resistance are 20% - 40% and 30%-50%, respectively [20]. This study showed in obese PCOS patients the insulin resistance incidence reached 80%, which is well above average. Insulin resistance also plays an important role in the pathogenesis and progression of PCOS. It increases the level of glucose in blood and leads to excess production of insulin, which further causes the imbalances of lipid and hormone levels [4,21,22]. The decreased HOMA-IR, FINS and FBG levels suggested that the insulin resistance improved after weight loss. That is consistent with previous studies [23,24].
Abnormal sugar metabolism leads to the lipid metabolism disorder [25]. Serum levels of several components of lipid metabolism index including TC, HDL and Apo B were significantly changed after weight loss, indicating the lipid metabolism disorder consequently improved. In addition, The HDL level has a negative correlation with the risk of coronary heart disease, while TG and LDL levels are positively correlated with that [26,27]. The increased HDL and decreased TG and LDL levels showed that weight lost could balance lipid metabolism and may then reduce the risk of long-term cardiovascular diseases.
LEP is closely related to appetite, synthesis and secretion of sex hormones. In peripheral, a high level of LEP in follicular liquid interferes follicle and oocytes maturation, and suppresses ovulation. A high concentration of LEP in blood affects the granular cell, restrains aromatase activity, and prevents the transformation from estrogen to androgen, resulting in increased blood androgen levels. Leptin may also lead to IR through the energy and metabolic pathways. Thus, it participates in the pathogenesis of PCOS. Therefore, the reduction of LEP level observed here was consistent with weight loss, and the shifts of androgen and insulin resistance level. ADPN can increase the insulin sensitivity [28,29] suggesting the increased ADPN level after weight loss could also contribute to the improvement of insulin resistance.
This study shows dietary intervention in obese PCOS patients can effectively recued weight, and improve menstrual disorder, acne and hirsutism via adjusting endocrine hormone levels, adipocytokine levels as well as glucolipid metabolism that are associated with PCOS pathogenesis such as insulin resistance and hyperandrogenemia. The performance of dietary weight-loss is comparable with previous studies [30,31]. No side effects were seen in study. However, weight relapse is still an issue of this method. We conclude dietary weight loss can be clinically implemented with precaution on weight relapse, and the subsequent weight maintained is recommended after weight loss.
None declared
ZZ designed the study. JH and ZZ collected the data, performed statistical analysis and drafted the manuscript. Both authors read and approved the final manuscript.
The authors are grateful to all members of the Department of Gynecology Nanjing Medical University, Affiliated Hangzhou Hospital. The authors have no potential conflicts of interest.

![]()

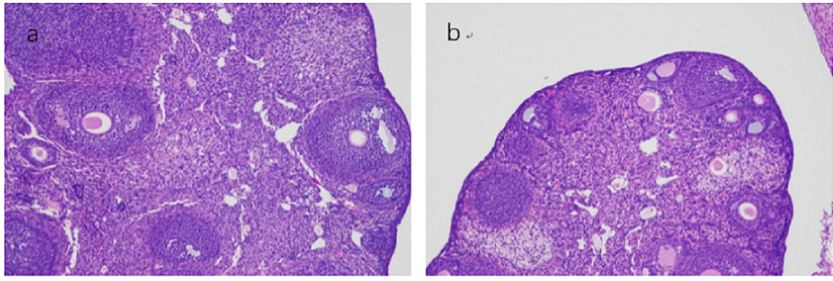 |
| Figure 1: (a and b) Shows present ovary shape in control and PCOS group, respectively |
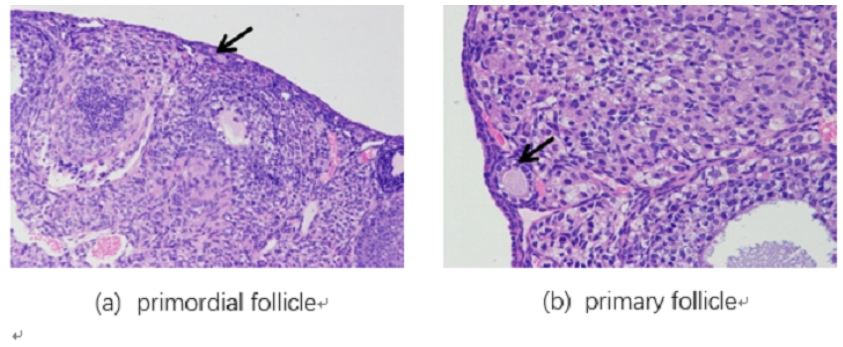 |
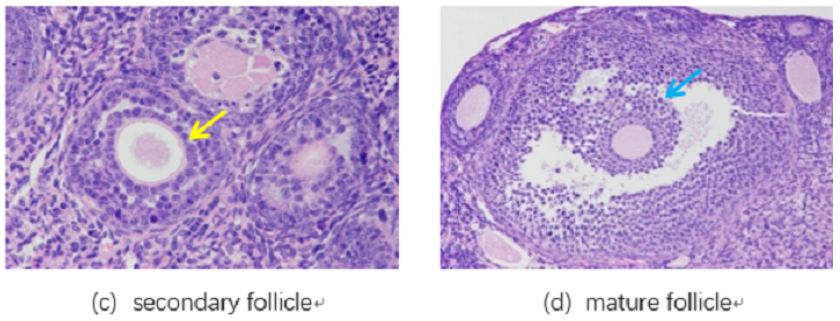
| Figure 2: (a,b,c and d) Represent HE staining pictures of primordial, primary, secondary, mature follicle, respectively |
 |
| Figure 3: Immunohistochemical staining for Nppc (the top two lines) and Npr2 (the bottom two lines) in ovarian tissues, including primordial (column 1), primary (column 2), secondary (column 3), and mature follicles (column 4) in normal and PCOS mice ovarian tissues. The background staining of each picture was violet blue, and positive staining for Nppc and Npr2 expression appeared as yellow or brown |
General indicators |
PCOS |
Control |
P value |
Weight (mg) |
17.91±0.89 | 16.41±0.80 | 0.011 |
E2 (pg/ml) |
92.94±12.95 | 105.50±14.15 | 0.289 |
T (ng/ml) |
4.56±2.40 | 0.03±0.03t | 0.014 |
FSH (mIU/ml) |
8.19±2.53 | 8.09±0.83 | 0.957 |
INS (mIU/ml) |
4933.36±614.00 | 4622.84±572.49 | 0.458 |
GLU (mmol/L) |
4.74±0.82 | 3.44±0.42 | 0.045 |
HOMA |
1042.84±235.64 | 699.05±29.71 | 0.042 |
Follicular staging |
Control group |
PCOS group |
P |
Primordial follicles |
393.54±292.10 | 478.06±500.93 | 0.642 |
Primary follicles |
1588.20±1160.94 | 2933.98±1750.77 | 0.048 |
Secondary follicles |
5671.86±2790.69 | 9252.30±4588.79 | 0.023 |
Graafian follicles |
18419.56±341.80 | 31253.88±4107.71 | 0.03 |
Follicular staging |
Control group |
PCOS group |
P |
Primordial follicles |
499.75±542.05 | 875.10±1112.24 | 0.448 |
Primary follicles |
1524.34±945.76 | 3000.98±1819.98 | 0.041 |
Secondary follicles |
6062.68±2861.65 | 10862.60±2854.98 | 0.007 |
Graafian follicles |
13811.36±1896.15 | 31185.75±5181.68 | 0.031 |




































