Open Access
Research Article
Max Screen
ISSN: 2454-3284
Copyright: © 2019 Jain N. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Intra-uterine copper devices (IUCD) are one of the most widely used reversible contraceptive methods used in India due to its lost cost, easy availability and long duration of action. However it is associated with few complications, one of the most important among which is uterine perforation and IUCD migration. IUCD might migrate into abdominal cavity, intestine and very rarely into the urinary bladder. Authors hereby review the literature regarding presentation, diagnosis and management of migrated IUCD in the urinary bladder via a rare case of 35 years old woman who presented with suprapubic pain since 1 month and found to have lost Copper T in the urinary bladder, which was inserted 14 years back postpartum. Laparotomy with cystotomy was done and complete IUCD was retrieved from wall and cavity of bladder successfully.
Keywords: Copper T; Displaced IUCD; IUCD Complications; Migrated IUCD
Intra-uterine copper devices (IUCD) are one of the most widely used reversible modes of contraception in India. Copper T 380A has been included in national family planning program in India, and hence available at free of cost at all government medical facilities. Although it is associated with few complications, but missing Copper T is one of the most commonly encountered complications. This missing Copper T might get displaced from uterine cavity due to uterine perforation and migrate into abdominal cavity, intestine or urinary bladder. Migrated IUCD in bladder is mostly asymptomatic, but may present with lower urinary tract symptoms. To prevent future complications, removal of migrated Copper T should be done. Removal can be done by cystoscopy or suprapubic cystotomy depending on adherence to bladder wall and protrusion into the vesical cavity. Authors hereby will review the literature regarding migrated IUCD into the urinary bladder via a case of lost IUCD found in the urinary bladder.
35 years old, multigravida woman presented to outpatient department of gynaecology department with complaint of suprapubic pain. There was no history of bleeding or burning during micturition. She was prescribed antibiotics for urinary tract infections. But, her pain was not relieved. She took repeated course of antibiotics, but still pain was persistent. Then, an ultrasound was advised on which she was found to have displaced IUCD in the abdominal cavity with doubtful impingement over the urinary bladder.
Obstetric history revealed that she had a vaginal delivery 14 years back, after which got Copper T inserted at a health centre. Shelf life of Copper T was 10 years. However, after two years she again conceived. She went to a private practitioner, who examined her and told that there are no visible Copper T threads, so she was told that Copper T has been expelled unknowingly and that’s why she has conceived. She delivered a tem healthy baby vaginally. After two years, she underwent bilateral tubal ligation (salpingectomy) procedure. She was comfortable since then.
On examination, her vitals were normal. On per speculum examination, IUCD threads were not seen. On per Vaginum examination, uterus was retroverted, normal in size with normal adnexa. Blood investigations were done, which were found to be normal. On urine analysis, pus cells were found and infection with E.Coli was found.
A contrast enhanced CT scan was done, on which migrated IUCD was found along posterior wall of bladder, distal end with threads in the cavity and both horizontal limbs completely adhered to the wall (Figure 1). Due to its unique presentation, with adhered part of IUCD in the wall of bladder, decision of laparotomy was taken.
On laparotomy, abdomen was open by midline vertical incision. Abdominal cavity was found to be normal. Uterus and bilateral adnexa was normal. However, adhesions were found between posterior wall of bladder and anterior wall of uterus at one point. Probably, this might be the part of uterus which perforated, because of which IUCD get displaced and migrated from uterine cavity& got adhered over the bladder. Copper T threads were visualised over the bladder wall (Figure 2a). Cystotomy was done by horizontal incision over the dome of bladder and vertical limb of IUCD was found in the cavity (Figure 2b). Both horizontal limbs were broken and were embedded deeply in the bladder wall (Figure 2c). Hence, complete IUCD was retrieved successfully from different sites of bladder (Figure 2d). Bladder was resutured in layers. Water tight closure was ensured. Suprapubic catheter along with urinary catheter was kept for three weeks. Post-operative period was uneventful and patient was discharged under satisfactory conditions.
IUCD are one of the most common method of contraception used in India. These are one of the most reliable, cost effective, long acting, and reversible method of contraception. Its failure rate is around 0.5-1/1000 cases [1].
It is associated with few complications such as pelvic pain, abnormal uterine bleeding, dysmenorrhea, pelvic infection, expulsion, uterine perforation and migration into the adjacent organs such as sigmoid colon, urinary bladder. Although these complications are rare, but can interfere with woman routine activities because of which, IUCD might be required to be removed. These lost IUCDs should be diagnosed promptly and removed without any delay by minimally invasive procedures such as laparoscopy, hysteroscopy & cystoscopy. However, if these procedures fail, laparotomy might be required to be done.
One of the extremely rare complications of IUCD insertion is uterine perforation and migration of IUCD into the urinary bladder. The estimated incidence 0.87/1000 cases, but the exact incidence is difficult to estimate due to its extreme rarity and mostly asymptomatic nature of presentation [2].
Uterine perforation due to IUCD can be primary or secondary. Primary perforation occurs at the time of insertion of IUCD, manifested as severe abdominal pain [3]. Secondary perforation is a delayed event, proposed to be occurring due to gradual pressure necrosis of uterine wall [4]. The exact mechanism of uterine perforation and migration of IUCD is not yet clear; however few hypotheses have been postulated. One of the most commonly accepted postulation is that spontaneous perforation of uterus due to IUCD occurs due to physiological uterine contraction, especially during postpartum phase when uterus is undergoing involution.
Once uterine perforation occurs, it might remain in the peritoneal cavity or migrate into adjacent organs. In most of the cases (80%), it remains in the peritoneal cavity. Once migrated, it might penetrate various organs such as omentum, recto sigmoid colon, appendix, urinary bladder, small bowel, iliac veins or even adnexa [5,6]. Migration into the urinary bladder usually occurs due to detrusor muscle contraction. However, this process might take months to years to happen [7].
Women who are at high risk of having uterine perforation and migration of IUCD includes lactating women, previous caesarean section, history of abortions, history of uterine curettage and history of any other uterine or cervical surgeries.
In the case discussed here, IUCD was inserted during lactation phase, which might be the cause of uterine perforation. This patient had a normal delivery after IUCD insertion. So, probably uterine perforation happened during insertion while migration might have occurred during delivery. Another high risk factor was history of uterine curettage done twice due to incomplete abortion.
Mostly, such cases remain asymptomatic. Hence these cases have delayed presentation and are difficult to diagnose. However, few patients might present early with complaint of missing thread. Most commonly, it presents lately with lower urinary tract symptoms such as suprapubic pain, dysuria, haematuria, burning micturition, recurrent urinary tract infections. Sometimes, patients might present with pelvic pain especially during menstrual cycles. Cyclical haematuria has also been reported in few cases. In the case discussed here, patient presented with suprapubic pain after 14 years of IUCD insertion.
Diagnosis of misplaced IUCD into the urinary bladder requires high clinical suspicion. Usually patients give history of IUCD insertion and on examination IUCD threads are not visible. In such cases, imaging modality shall be done to locate IUCD. X ray pelvis is usually the first diagnostic modality to diagnose misplaced IUCD. X ray is usually taken with uterine sound placed in the uterine cavity, which helps in deciding the location of IUCD. However, on X-ray, the exact location of misplaced IUCD is difficult to diagnose. Hence, ultrasonography is the most commonly used modality to diagnose the misplaced IUCD and to find its location. However, in certain cases, ultrasonography is not able to identify the exact position and site of migrated IUCD in the bladder, hence, MRI might be required to find the exact location of lost IUCD and thereby, deciding the mode of management.
Lost IUCD mostly remain asymptomatic. However, prolonged presence of IUCD into the bladder might lead to complications such as calculi formation, cystitis, recurrent urinary tract infections and adhesions formations. However, once diagnosed it should be removed as soon as diagnosed. Minimally invasive procedures are the first line of management. Cystoscopy is one of the best modality to remove it since it is both diagnostic and therapeutic [8]. However, in cases where IUCD is adhered to the bladder wall or associated with large vesical calculi, laparotomy is done with suprapubic cystotomy. Urinary Catheter is kept for two to three weeks.
While reviewing the literature, it was found that few cases of migrated IUCD in the urinary bladder have been reported. Authors hereby, are discussing some of these cases to discuss pathogenesis, clinical presentation, diagnosis and management of these cases. In a case study, it was found that till date only 25 such cases of uterine perforation by IUCD and migration into the bladder have been reported [9].
In 2006, Y. Nouira, et al. published a case series of six cases describing migrated IUCD in the bladder. All of these cases were found to have intra-vesical IUCD along with bladder stone [10]. Mechanism of this migration was proposed as a progressive event, occurring due to endometrial inflammation along with enzyme liberation from copper T device. In all of these cases, IUCD was removed by minimally invasive procedure. By cystoscopy, whole of the copper T was retrieved along with calculi. All cases were uneventful, except one, in which a punctuate bladder perforation occurred while pulling IUCD. This case was managed conservatively and patient was discharged under satisfactory condition. Thus, it was concluded that migrated IUCD in urinary bladder can be associated with complications such as calculi formation, thus shall be removed promptly. Removal can be done successfully by cystoscopy and open surgery shall be avoided.
In 2007, Esfahani, et al. reported a case of intra-vesical migration of IUCD. The clinical presentation of this case was unique. A 28 year old woman with four live issues, presented with complaints of dysuria, haematuria and frequency of micturition. She also had complaint of disseminated pelvic pain which used to occur especially during menstrual cycles. These complaints were present since 4 years. She also had history of cystocoele repair & rectocoele repair surgery. After surgery, she had recurrent urinary tract infection, without fever and chills, which was not responding to antibiotics. Ultrasonography was done, on which she was found to have migrated IUCD in the urinary bladder along with a calculus. Cystoscopy was done as a first line management; however neither calculi nor IUCD was visible. Hence, laparotomy was done and calculus of 2cm was found in upper left side of bladder along with IUCD, stucked to calculus. Both were removed completely. Hence, it was concluded that in a woman presenting with recurrent lower urinary tract symptoms, migrated IUCD in bladder should be suspected and once diagnosed, shall not be neglected [5].
In 2010, M.Tosun, et al. reported a case of 28 years old woman with 8 weeks of pregnancy who was found to have migrated IUCD in the urinary bladder. Cystoscopy was performed under general anaesthesia and it was found that tail & body of IUCD was penetrated into the bladder mucosa and become embedded in the posterior wall of bladder. The tail was grasped by forceps and whole unit was removed successfully. The patient was discharged on day 3 without any complications and pregnancy was continued. Hence, it was concluded that 1cystoscopy can be done successfully even during antenatal period [11].
In 2018, Mon-Lai Cheung, et al. described a case of 34 year old woman, fifth gravida, who presented with leaking per Vaginum. Caesarean section was done due to preterm rupture of membranes and suspected chorioamnionitis. On post operated day 5, patient developed with high grade fever with suspected intra-abdominal collection. CT scan was done which revealed a displaced IUCD with tip penetrating in the lumen of urinary bladder near its anterior portion. Cystoscopy was done but IUCD could not be visualised, since it had not penetrated the mucosa of bladder. Hence, laparotomy was done and IUCD was removed from serosal & muscular is layer of urinary bladder. So, it was concluded that although laparoscopy/cystoscopy should be considered as first modality to remove lost IUCD. However, in certain cases, laparotomy needs to be done [12].
Uterine perforation and migration of IUCD into the urinary bladder is one of the most crucial complications associated with IUCD insertion. To prevent such complications, proper case selection and proper training should be given to paramedical staff for safe insertion. Patient should be counselled for regular follow up. A clinician must be vigilant to diagnose such cases. Once a case is diagnosed, it should be removed promptly to prevent future complications. Cystoscopy is the ideal method to remove it, however in certain cases; laparotomy might be required to be done.

![]()

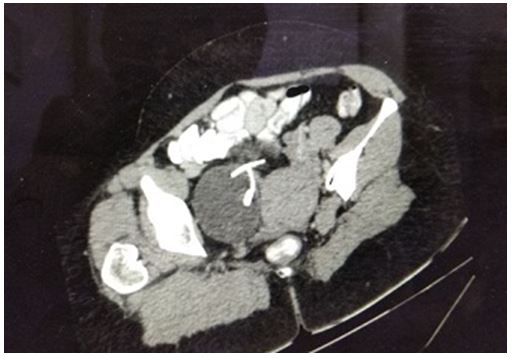 |
| Figure 1: Contrast CT scan image of pelvis showing IUCD in the urinary bladder with vertical limb in the cavity and horizontal limbs outside |
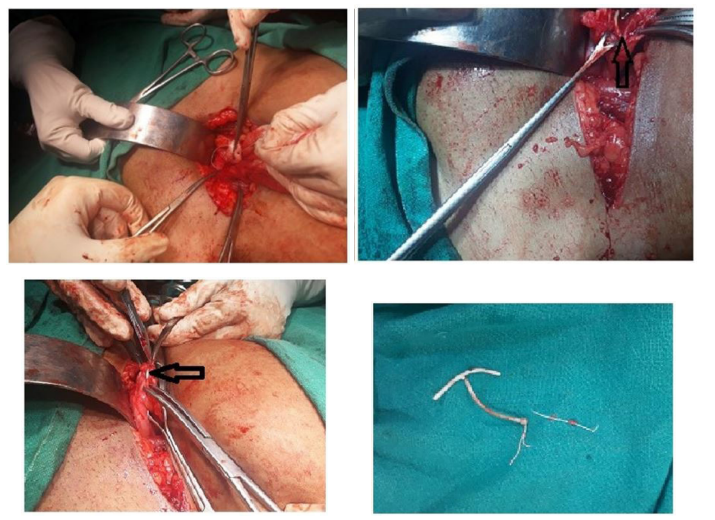 |
| Figure 2: Laparotomy image showing Copper T retrieval from urinary bladder (a) Laparotomy image showing Copper T thread outside the bladder wall; (b) Laparotomy image showing vertical limb of Copper T retrieved from the cavity of urinary bladder; (c) Laparotomy image showing horizontal limb of Copper T embedded in the wall of urinary bladder; (d) Image of complete Copper T, retrieved from urinary bladder with both horizontal limbs, vertical limb and both threads |




































