Open Access
Case Report
Max Screen
ISSN: 2454-3284
Copyright: © 2019 E. Khilkevich. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
The incidence of urinary tract endometriosis ranges from 0.3 to 12% of all women affected by endometriosis. Endometriosis has been successfully treated at General Surgery Department of National Medical Research Center of Obstetrics, Gynecology and Perinatology named after V.I. Kulakov in Moscow. In the 2012-2016 period, we performed 23 bladder resections, ureterolysis in 35 patients, 3 ureteral resections with reimplantations, 3 ureteral resections and uretero-ureteral anastomosis. All these procedures were performed for urinary tract endometriosis. We present 2 cases of urinary tract endometriosis in women of reproductive age. The possibilities of hormonal therapy in the treatment of endometriosis are limited. Surgical intervention with complete removal of endometrial tissue is the most effective; however, the probability of recurrence still remains high, especially in young patients.
Keywords: Ureteral Endometriosis; Bladder Endometriosis; Deep Infiltrating Endometriosis; Hydronephrosis
Deep infiltrating endometriosis (DIE) is a specific entity in which endometriotic lesions penetrate the walls of any pelvic organ or/and the retroperitoneal space to a depth of at least 5 mm [1-3]. The incidence of urinary tract endometriosis (UTE) ranges from 0.3 to 12% of all women affected by endometriosis [4]. It is known that isolated endometriosis of the urinary tract practically does not occur. Bladder endometriosis accounts for 84% of all UTE cases. About 5-20% of patients suffer from ureteral endometriosis [5]. The left ureter is most frequently affected. This fact can be explained by anatomical features. The location of the sigmoid colon contributes to the isolation of the left adnexa; as a result immune cells cannot reach the endometrial cells trapped into the peritoneal environment from the left fallopian tube. Ureteral endometriosis can lead to the obstruction of the urinary tract and, as a consequence, to hydroureteronephrosis with the decrease in the functional activity of the kidney. The clinical manifestations of UTE may be abdominal pain radiating to the lumbar area, renal colic, hematuria, cyclical dysuria [6].
Endometriosis has been successfully treated at General Surgery Department of National Medical Research Center of Obstetrics, Gynecology and Perinatology named after V.I. Kulakov in Moscow. In the 2012-2016 period, we performed 23 bladder resections, ureterolysis in 35 patients, 3 ureteral resections with reimplantations, 3 ureteral resection and uretero-ureteral anastomosis. All these procedures were performed for urinary tract endometriosis. We present 2 cases of the urinary tract endometriosis in women of reproductive age.
A 38-year-old woman was admitted to General Surgery Department of our center for periodic abdominal pain radiating to the lumbar area, and cloudy urine. Her menstrual cycles were normal. The woman was never pregnant. She underwent myomectomy with coagulation of external genital endometriosis by laparoscopic approach. On physical examination of the woman no abnormalities were revealed. Laboratory test results were normal.
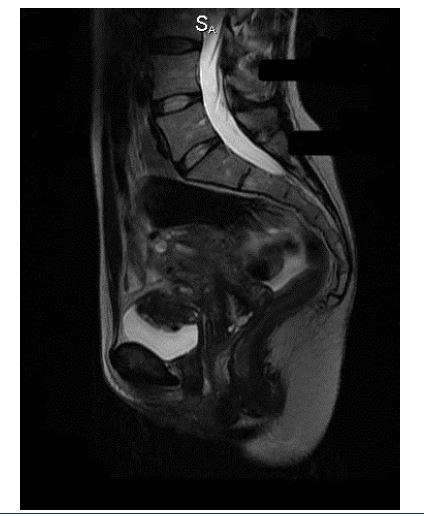
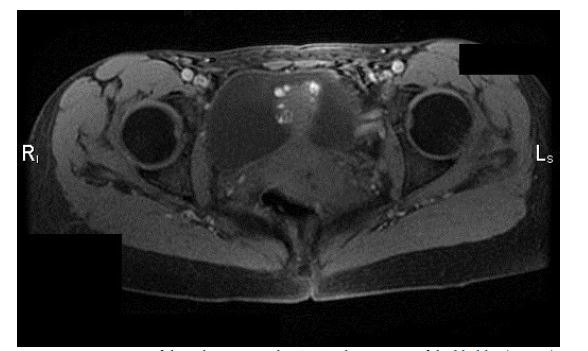
The patient presented with the pain in the lower abdomen and cloudy urine. Urinary tract ultrasonography showed left sided hydroureteronephrosis. The patient underwent ureteroscopy with ureteral stent placement. A magnetic resonance imaging (MRI) scan showed local stenosis of the left distal ureter. Its length is more than 1cm and it is characterized by the presence of a perifocal zone of fibrous changes (Figure 1). These changes could be both endometrial and post-inflammatory ones.
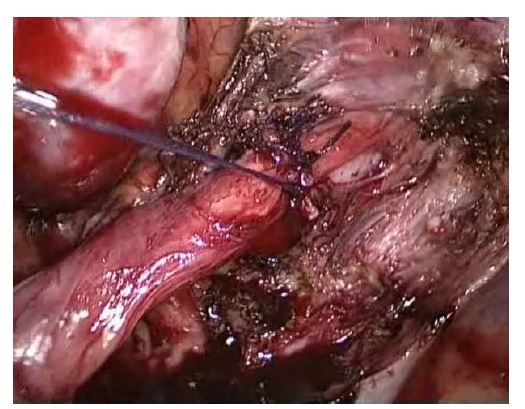
After analysis of the patient’s complaints and the results of clinical evaluation and instrumental tests, it was decided to perform operative treatment by laparoscopic approach. On visualizing the pelvic organs of the patient on the left lateral surface of the pelvic wall measuring 2.5 × 3.0 cm (, in the projection of the left ureter, endometrioid infiltrate was revealed. It was dense, immobile, and tuberous, Figure 2). On the periphery of the infiltrate, the dissection of the peritoneum was performed with an L-shaped dissector and mobilization of the complete infiltrate was started (Figures 3 and 4). It was revealed that the left ureter was blocked by endometrioid infiltrate from all sides; it was deformed and thinned all over. Considering the signs of ureteral invasion, it was decided to perform a complete resection of the ureter (Figure 5).
Cystoscopy was performed; the bladder was filled with 150 ml of physiological solution, the mucosa being without pathological changes. In the left ureter, the stent that had been placed before still functioned. The right ureter was located in the typical place, rhythmically excreting trickles of transparent urine. Within the proximal 0.5 cm of infiltrate, the main section of the ureter was intersected, the stent was removed. Endometrioid infiltrate was completely excised and evacuated from the abdominal cavity through the trocar hole. After excision of endometrioid heterotopy from the edge of the ureteral cut, the distal ureter was mobilized. The left ureter was stented again (Figure 6). Uretero-ureteral end-to-end anastomosis with 0000 Vicryl sutures was performed (Figures 7 and 8). No extravasation was observed in the anastomosis site.
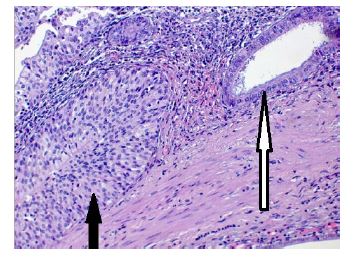
The postoperative period proceeded without any complications. The patient received antibacterial, infusion, and anti-inflammatory therapy. The patient was discharged on the 6th postoperative day in a satisfactory condition. Subsequently, she had postoperative follow up visits to a gynecologist and urologist. The urinary catheter was removed on the 7th postoperative day. The stent was removed after three weeks (on the 21st postoperative day). The pathohistologic specimen demonstrated the presence of endometrioid heterotopies in the ureter wall (intrinsic endometriosis of the left ureter with endometrial glandular cells and stromal tissue) (Figure 9). As postoperative medical treatment, the patient was prescribed dienogest 2 mg a day for 6 months.
A 34-year-old woman was admitted to our department for painful prolonged (up to 14 days) menstruation, painful urination from the 5th to the 10th day of the menstrual cycle. The woman had been smoking on average 6-7 cigarettes a day for 15 years. She suffered from chronic pancreatitis, chronic gastritis, urolithiasis, varicose veins of the lower extremities. Her menstrual cycles were regular but prolonged (from 6 to 14 days) and painful. The patient had a pregnancy which resulted in spontaneous delivery. She underwent hysteroscopy with diagnostic endometrial scraping for menorrhagia. The patient had been observed by gynecologist for 10 years, she was diagnosed adenomyosis, small myoma of the uterus. The patient took combined oral hormonal contraceptives containing 30-mg Ethinyl Estradiol and 3-mg Drospirenone for 8 years.
A gynecologist revealed a mass in the bladder region on bimanual examination. The patient was referred to the urologist. Suspecting a tumor at the bladder wall, cystoscopy with biopsy was performed. Pathologic specimens demonstrated papillary-polypoid cystitis. The patient was prescribed conservative therapy which had a temporary effect. After 8 months the patient noted worsening of the condition, namely increased intensity of dysuric disorders. After 7 months she consulted the specialists of our centre. On bimanual examination a nodal mass 3 cm in size was palpable through the anterior fornix of the vagina. The nodule was mobile and painful on palpation. The patient was recommended to perform an MRI examination of the pelvic organs. MRI studies revealed the II degree of diffuse adenomyosis, external genital endometriosis and endometriosis of the bladder (Figures 10a and b). Moreover, MRI showed pelvic adhesions, varicose veins of the uterus, left ovarian varicosities, paraurethral cyst.
After the analysis of the patient’s complaints and the results of clinical examination and instrumental tests, it was decided to perform operative laparoscopy. The patient underwent bladder resection, excision of endometriosis of the uterovesical fold, cystoscopy. On performing cystoscopy, the mass with multiple bluish vesicles 4 × 3 cm in size was visualized. The ureteral orifices were 4 cm from the mass (Figure 11). In order to minimize intraoperative risks of damage to the uterus and provide better visualization, ureteral catheters 6 Fare were installed in the lumen of the ureters (Figure 12).
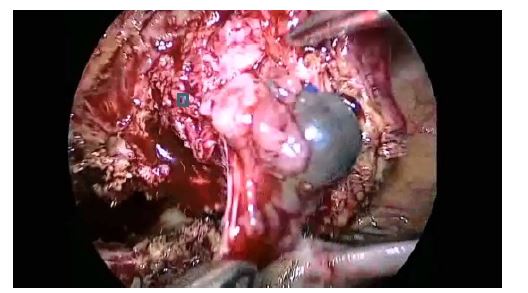
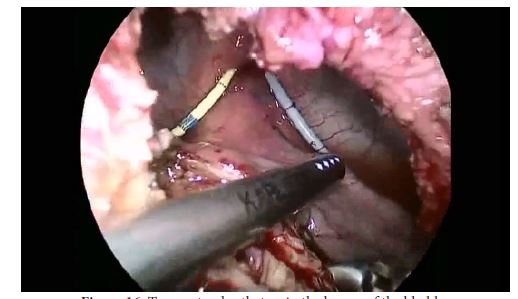
Before the uterus, an infiltrate was identified which involved the uterus, large omentum, round ligaments of the uterus, the bladder, and the dome of the cecum (Figure 13). The infiltrate was divided by sharp and blunt dissection. The bladder was separated from the uterus and it was mobilized at a distance of 4 cm from the margin of the infiltrate (Figure 14). The dissection of the bladder wall along the endometrioid infiltrate was performed gradually layer by layer to the mucous membrane. At the margin of the infiltrate, the lumen of the bladder was opened (Figures 15 and 16). Complete removal of the infiltrate was performed. In addition, the part of the infiltrate remaining on the bladder wall was excised before the appearance of the bleeding sites. The resected part of the bladder with endometrioid infiltrate and the fragments of endometrioid infiltrate were removed in the plastic container though the left trocar hole. The wall of the bladder was sutured in double layer (mucocutaneous and serous-muscular) with Vicryl sutures (Figures 17 and 18). Sides of the sutures were sealed. The abdominal cavity was washed and drained. No extravasation was observed. Pelvic drainage was installed at the end of the procedure. Foley catheter 18F was inserted into the bladder.
Hysteroscopy and separate diagnostic scraping of the endometrium were also performed. The postoperative period was complicated by urolithiasis; the patient experienced an attack of renal colic on the 2nd day after the operation.
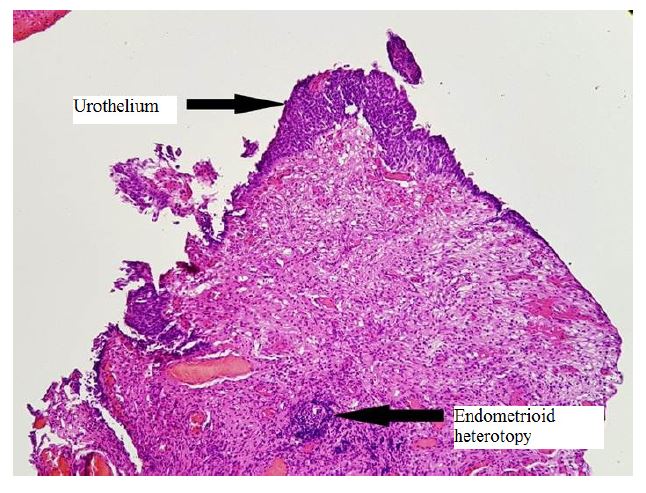
She received antibacterial, antispasmodic, anti-inflammatory therapy that had a positive effect. Monitoring of the amount and color of urine was performed on the Foley catheter; the patient had an ultrasound of the kidneys, bladder, and abdominal organs. Postoperative diuresis was sufficient, color of urine restored to normal on the 5th day after surgery. On the 8th day after the operation, the patient underwent cystography, which showed the tightness of the suture on the wall of the bladder, and the urinary catheter was removed. On the 10th day postoperative sutures were removed. On the 12th day the patient was discharged in a satisfactory condition. Subsequently, she had postoperative follow up visits to a gynecologist and urologist. The histological picture of bladder endometriosis is shown in (Figure 19). Pathologic specimen demonstrated the presence of endometrioid heterotopy with high expression of estrogen and progesterone receptors in glands and stroma (H-score> 250) in urothelium (bladder epithelium) (Figure 20). Immunohistochemical test demonstrated the expression of Ki-67 in 20% of cells in the endometrioid heterotopy, and in 30% in the region of urothelium (Figure 21).
As postoperative medical treatment, the patient was prescribed dienogest 2 mg a day for 6 months. But she had to stop taking it earlier due the side effects of this preparation: the patient experienced pains and breast engorgement.
Difficulties in managing patients with endometriosis are associated with an extremely variable clinical picture and the severity of the course of the disease; the tactics depend on the age of the patients, the form and stage of the disease, the symptoms, reproductive problems, risks, side effects and economic cost-effectiveness of treatment [1].
The ratio of the frequency of the urinary system endometriosis (bladder/ureters/ kidney/urethra) is 40:5:1:1, respectively [7]. In our clinical cases there was endometriosis of the bladder and left ureter, which confirms the high incidence of these urinary tract locations of endometriosis. The clinical picture of the urinary tract endometriosis is variable and depends on the localization, depth and size of the lesion. In the asymptomatic course of the disease, endometriosis can be revealed during diagnostic laparoscopy or visual research methods when a woman presents with infertility. When endometriosis affects the organs of the urinary tract, patients may complain of periodic pain in the lumbar region, painful urination, and dysuria. The pathognomonic sign for the bladder endometriosis can be the presence of blood in the urine, especially during menstruation days.
In our cases, patients complained of periodic pains in the lower abdomen, cloudy urine, and pain when urinating from the 5th to the 10th day of the menstrual cycle. According to the literature, about 50% of women with urinary tract endometriosis were subjected previously to surgical interventions in the small pelvis [2]. Our patient with the left ureter endometriosis had undergone an operation for external genital endometriosis laparoscopically 3 years before, which is confirmed by this observation.
When endometriosis affects the organs of the urinary tract, the main task is to prevent renal failure due to the frequent development of hydronephrosis on the affected side [6]. Hormonal therapy affects the focus of endometriosis, but does not eliminate ureter obstruction if it is present. Endometriosis in the bladder is not sensitive to hormonal therapy [8]. The optimal method of treatment is resection of the bladder and complete excision of the infiltrate [9,10]. In the case of ureteral endometriosis, specialists of our centre performed left ureteral resection, stenting, and uretero-ureteral end-to-end anastomosis by laparoscopic approach. The patient with bladder endometriosis had a resection of the bladder, excision of endometriosis of the uterovesical fold also laparoscopically.
The main aim of surgical intervention is a complete removal of endometrial tissue to improve the effectiveness of treatment and reduce the risk of recurrence of the disease. Surgical treatment of ureteral endometriosis can be performed as ureterolysis, ureteroneocystostomy or ureteroectomy, applying end-to-end anastomosis. Functional activity of the bladder can be preserved due to the resection of the bladder with removal of the tissue of the organ affected by endometrioid heterotopy [2].
Specialists in gynecology and urology should consider the probability of endometriosis of the urinary tract and suspect the presence of this pathology in women of reproductive age with hydronephrosis and pain in the lower abdomen. Surgical intervention with complete removal of endometrial tissue is the most effective; however, the probability of recurrence still remains high, especially in young patients.
Written informed consent was obtained from the patients for publication of this case reports and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.

![]()

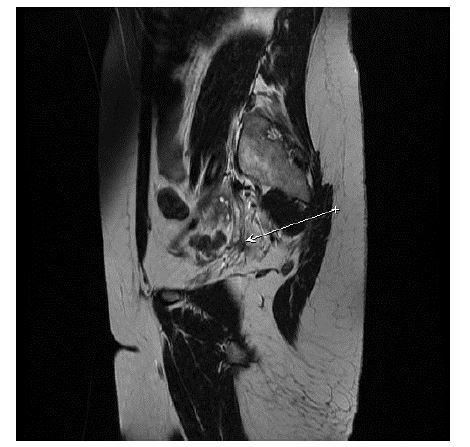 |
| Figure 1: MRI scan showing local stenosis of the left distal ureter with the length of >1cm characterized by the presence of a perifocal zone of fibrous changes |
 |
| Figure 2: The projection of the left ureter showing endometrioid infiltrate which is dense, immobile, tuberous and measuring 2.5 × 3.0 cm |
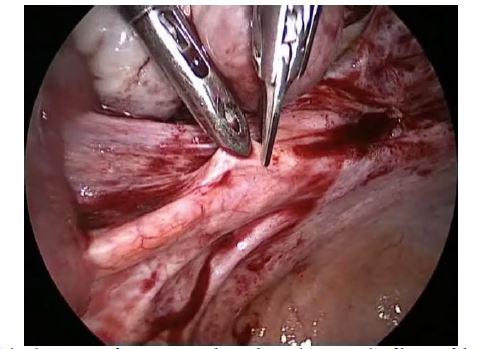 |
| Figure 3: The dissection of peritoneum above the endometrioid infiltrate of the left ureter |
 |
| Figure 4: The dissection of the infiltrate with an L-shaped dissector |
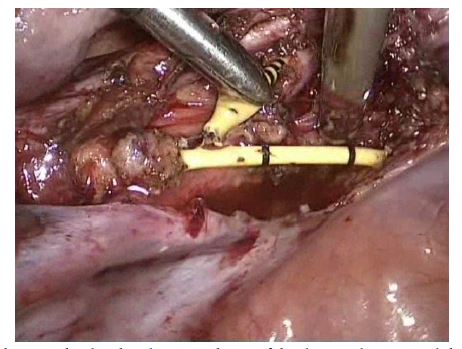 |
| Figure 5: Fragment of the operation showing the distal and proximal part of the dissected ureter and the previously inserted urethral catheter |
 |
| Figure 6: Cystoscopy. Ureteral catheterization |
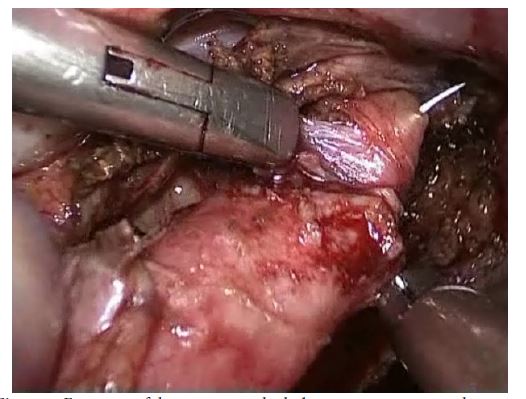 |
| Figure 7: Fragment of the operation which demonstrates suturing the ureter |
 |
| Figure 8: Uretero-ureteral end-to-end anastomosis with 0000 Vicryl sutures |
 |
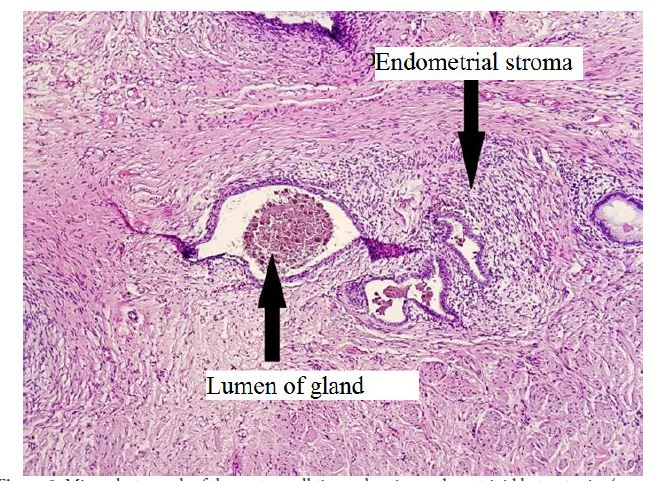 |
| Figure 9: Microphotograph of the ureter wall tissue showing endometrioid heterotopies (arrows) |
  |
| Figure 10: MRI scan of the pelvic organs showing endometriosis of the bladder (arrows) |
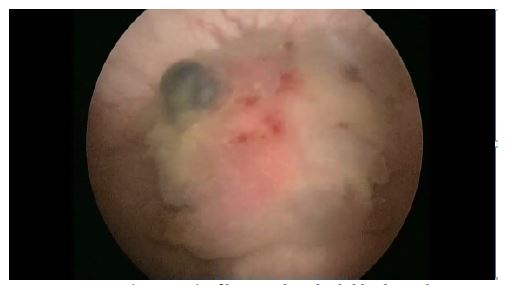 |
| Figure 11: Cystoscopy. Endometrioid infiltrate with multiple bluish vesicles 4 × 3 cm in size |
 |
| Figure 12: Cystoscopy. Ureteral catheterization |
 |
| Figure 13: Abdominal view. The infiltrate identified before the uterus involves the uterus, large omentum, round ligaments of the uterus, the bladder and the dome of the cecum |
 |
| Figure 14: The bladder during the mobilization at a distance of 4 cm from the margin of the infiltrate |
 |
| Figure 15: The view of endometrioid infiltrate in the lumen of the bladder |
 |
| Figure 16: Two ureteral catheters in the lumen of the bladder |
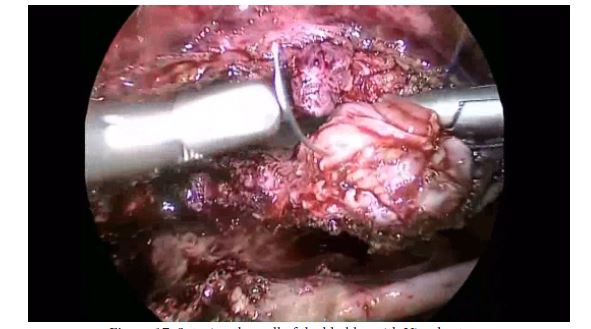 |
| Figure 17: Suturing the wall of the bladder with Vicryl sutures |
 |
| Figure 18: The final view of the operation |
 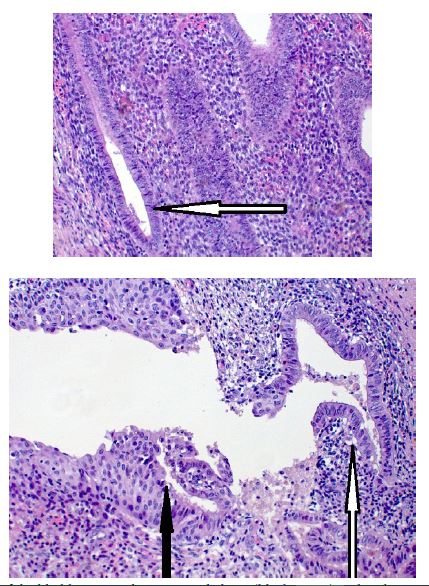 |
| Figure 19: Microphotograph of the bladder tissue showing urothelium (black arrow) and endometrioid heterotopy (white arrow) |
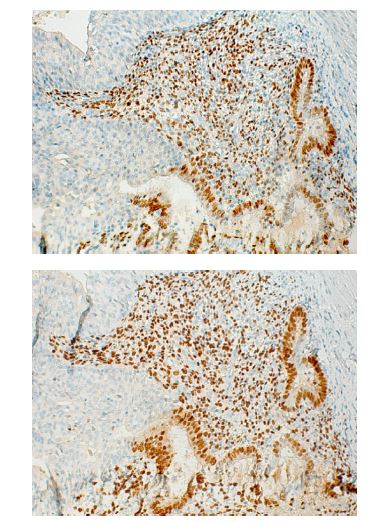 |
| Figure 20: Presence of endometrioid heterotopy with high expression of estrogen and progesterone receptors in glands and stroma (H-score> 250) in urothelium (bladder epithelium) |
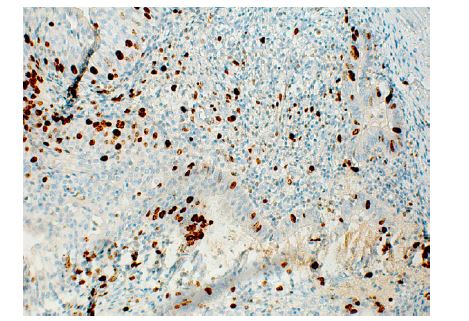 |
| Figure 21: Immunohistochemical test demonstrated the expression of Ki-67 in 20% of cells in the endometrioid heterotopy, and in 30% in the region of urothelium |




































