Open Access
Research Article
Max Screen
ISSN: 2575-5501
Copyright: © 2023 Zaim Gashi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
There is presented intrasphincetric injection management of achalasia, an esophageal dysmotility disorder involving an abnormal relaxation of the lower esophageal sphincter. Botulinum toxin A is a well-described treatment for achalasia, in patients who is contraindicated others modality due to comorbidity, especially in older age. We describe a case of a successful treatment of achalasia in the 83-old man with botulinum toxin A, as efficacy and very safe method for symptomatic relieve of these patients.
Keywords: Achalasia; Endoscopy; Botulinum Toxin; Injection
Achalasia represents the absence of lower esophageal sphincter relaxation and absence of normal peristalsis of the esophageal body, showed in incidence of 1-2 patients in 100 000 people. Causes of achalasia are of unknown ethiology or secondary causes. It is present equally in men and women, at every age [1,2,3]. Presence of alarm symptoms, such as dysphagia, weight loss, regurgitation, chest discomfort, anemia, family history of cancer, warrant further investigation. Specific testing is needed to distinguish achalasia from other disorders. For diagnosis, upper endoscopy, esophagogram, high resolution esophageal manometry are needed. In distinguished cases, abdomen and chest CT scan and pH testing are performed as well. There are several treatment modalities for achalasia. Botulin toxin injection is known since 1995, from Pasricha and Kalloo. Botulin toxin injection is an effective and safe treatment [4,5].
Our presentation is a success story and the first injection in our state, of Botulinum toxin in order to improve the symptomatic dysphagia, in a 73-year-old man, who had cardiopulmonary contraindications for surgery.
Our presentation is a successful story of the injection of Botulinum toxin in order to improve the symptomatic dysphagia, in a 73- year-old man, who had cardiopulmonary contraindications for surgery. Even after 6 months he feels quite well.
We hypothesized that locally injected botulinum toxin, a potent inhibitor of the release of acetylcholine from nerve endings, could be effective in the treatment of achalasia.
A 73-year-old male was referred to our institute with atypical chest pain, epigastric pain, and dysphagia, associated with weight loss. Physical evaluation shoved signs for one slight anemia and for atrial fibrillation in heart auscultation and extended expirium with slight wheezing due to obstructive chronic bronchitis. In the laboratory values, showed HGB 100, WBC 10.0, CPR 15. Others laboratoric values were in the reference values. His evaluation at the referring institution included a esophagogram study that showed an esophagram tertiary contractions with esophago-esophageal reflux and distal esophageal stricture with especially appearance of “bird’s beak” sign and a endoscopic evaluation, who are eliminates others benign and malignany pathology. For this aim was made and CT scan. The lower esophageal sphincter was visualized endoscopically by identification of the sphincteric rosette, typically seen at the squamocolumnar junction. Evaluation for scleroderma and autoimmune disease was negative. A trial of nifedipine was likewise unsuccessful, but his dysphagia continued to progress with further weight loss and a body mass index (BMI) of 16.2. The patient not reported occasional alcohol use and social smoking history.
After addmited to our institute, the patient reported a dysphagia with continued slight weight loss. Were processed diagnostic procedures such as mentioned above. Without treatment, his dysphagia worsened and he lost more weight, dropping to a BMI of 16.2. His Eckardt score was 9 (dysphagia: 3, pain: 2, regurgitation: 2 and weight loss: 2), and he was treated for dehydration in the emergency department twice. Because medical management had failed to resolve her symptoms, due to cardioerespiratory contraindication for Heller myotomy, verified from anesthesiologists and cardiologists and due to elderly age, local botulinum toxin A injection into the LES were considered. The patient was processed with esophagogastroduodenoscopy (EGD) and botulinum toxin A injection aliquots of 1 ml each (20 units of botulinum toxin per mililiter of saline) were injected into quadrants, for a total of 80 units, injected circumferentially into the submucosa just proximal to the LES.
After the procedure, into some days, the patient reported significant relief from dysphagia, and his Eckardt score improved to 2 (dysphagia: 1, pain: 0, and regurgitation: 1 and weight loss: 0). Before intrasphincteric injection of Toxin Botulin, Eckardt score was 9 (dysphagia: 2, pain: 2, regurgitation: 2 and weight loss: 3). Eckardt score is used to assess the severity of achalasia symptoms (Table 1)[6].
It is based on four major achalasia symptoms: dysphagia, regurgitation, chest pain, and weight loss. It is used to evaluate the efficiency of a treatment durring the follow-up. Clinical remission was defined as a Eckardt score of 3 or less during follow-up, and failure of treatment (or relapse) as a score of 4 or more. Patient was contacted by telephone about every four weeks to assess the clinical response to the injection and also questioned about the occurrence of potential complications of the injection, such as fever, chest pain, systemic weakness, influenza-like illness, and reflux. He gained approximately 4.8 kilograms and he BMI increased from 16.2 to 18.2. He underwent a second treatment of botulinum toxin A injection after eight months, due to reappearance of achalasia symptoms. Roughly eight months after delivery, the patient’s Eckardt score returned to 7.
Local injection of botulinum toxin is currently being used in the treatment of several disorders characterized by skeletal-muscle spasm (such as strabismus and a variety of dystonias), with good results and few adverse effects.[7]
Esophageal achalasia is an esophageal motility disorder involving the smooth muscle layer of the esophagus and the lower esophageal sphincter (LES)[8]. It is characterized by incomplete LES relaxation, increased LES tone, and lack of peristalsis of the esophagus (inability of smooth muscle to move food down the esophagus) in the absence of other explanations like cancer or fibrosis.[9][10][11] Dysphagia is the most prominent symptom.
Treatment options include diet modification, calcium channel blockers, nitrates, EGD with 30-35 mm of ballon dilation, botulinum toxin A injection, total parenteral nutrition, per oral endoscopic myotomy (POEM), Heller myotomy, and, in severe cases, percutaneous endoscopic gastrostomy (PEG) placement with enteral tube feedings.[12] Each of these interventions has potential risks, but laparoscopic surgical myotomy in cardiorespiratory patients and elderly age, is relatively contraindicated.
Botulinum toxin A injection is an attractive treatment option for, unlike other medications used to treat achalasia, the injections have local rather than systemic effects.
Injections of botulinum toxin is safe, simple and nonexpensive treatment for elderly patients with achalasia. This confirmed in our case presentation. Patient was wery satisfied with improvement of his symptoms. During his follow-up, not showed occurrence of above potential complications of the injection.
Limitation of our study was a esophagomanometry, which in our gastroenterologic center not performed due to absence of this device. But, endoscopic examination was performed from a endoscopic expert and priory results with esophagogram and CT scan, to excluded a malignant process.
Second limitations was absence of more cases and research from multicenter study.
A strong improvement from injection of Botox may help confirm a diagnosis of achalasia, and this showed our case study.
This case report ilustrates the safe treatment of achalasia with LES injection of botulinum toxin A. The effect was not long lasting, as is typical for this type of treatment, and our patient required repeated séance with botulin toxin eight months after first seance.

![]()

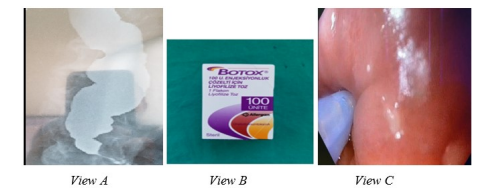 |
| Figure 1: Achalasio (A) Botulinum toxin that was injected (B) and endoscopic image of injection (C) |
Score |
Weight loss (kg) |
Dysphagia |
Retrosternal pain |
Regurgitation |
0 |
None |
None |
None |
None |
1 |
<5 |
Occasional |
Occasional |
Occasional |
2 |
5-10 |
Daily |
Daily |
Daily |
3 |
>10 |
Each meal |
Each meal |
Each meal |




































