Open Access
Research Article
Max Screen
ISSN: 2575-5501
Copyright: © 2018 Hormati A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Foreign body ingestion is a common occurrence among children and adults with certain risk factors including advanced age and psychiatric diseases. However, in clinical practice we encounter healthy adults who are diagnosed with unintentional foreign body ingestion and are not able to remember it. These cases may be complicated by gastrointestinal perforations in case of ingesting sharp objects. Only clinical suspicion would help clinicians for prompt diagnosis in such cases
This article introduces a young woman who presents to the gastroenterology clinic with epigastric pain. Since her symptoms did not improve with medical treatment, she underwent upper gastrointestinal endoscopy and a toothpick was found in the duodenum with penetration in both ends that the patient denied its ingestion. She discharged after 24 hours of successful removing of the foreign body with no complication in a 1 month follow up.
Keywords: Foreign Bodies; Abdominal Pain; Esophagoscopy
Foreign body ingestion is a common event that can be defined as accidental or intentional ingestion of substances or even food and medications [1].
Ingested objects often pass through the gastrointestinal tract without any complication [2]. However, the presence of long, sharp, narrow and hard bodies such as bones (fish and chicken) or toothpicks may result in rupture of gastrointestinal tract and its further complications including perforation and peritonitis, which may be fatal [2,3].
Foreign body ingestion is common in children [1] but in adults, it occurs in certain populations including old patients, patient with mental disturbance, alcoholics, prisoners and patient with psychiatric problems [4]. However, in practice, we encounter a not small group of healthy adults who have ingested foreign bodies unintentionally without any underlying risk factor [1].
In This article, we introduce a young female presented with abdominal pain and underwent upper GI endoscopy due to lack of response to medical treatment.
In endoscopy, a foreign body was detected with penetration into the duodenum.
A 27 years old female was presented to gastroenterology clinic with complaint of abdominal pain with superiority in the epigastric region and right upper quadrant of abdomen. She had no underlying illness.
Due to the patient’s low age and absence of alarm signs, she underwent empirical therapy with proton pump inhibitors (PPI) and H2 blockers but the symptoms didn’t change over the course of several months.
Since medical treatment did not improve her symptoms, the patient underwent upper GI endoscopy for further examination.
In endoscopy, a foreign object and an ulcer of 10×10 mm, which caused by the foreign body, were seen in the duodenum. Considering the bilateral penetration of the foreign body into the duodenal wall, it was released on one side by angled forceps and was removed from the duodenum (Figure 1).
Since both edges of foreign body were sharp and there was risk of complication such as injury and perforation of esophagus while retrieving, the endoscope was removed and a hood was placed on the head of the endoscope, then the head of the foreign body was taken by endoscopy and using snare and entered the hood.
It was extracted from esophagus successfully without causing complications such as perforation.
The extracted foreign body was an 8-cm long toothpick which the patient was unable to recall its ingestion.
She was discharged after 24 hours observation in the hospital ward, with good general condition. No complication was detected in one month follow up and her symptoms were fully recovered with an 8 weeks period of PPI treatment.
Foreign body ingestion is a common clinical issue. Since the ingested material passes spontaneously and uneventfully through gastrointestinal tract, most patients are monitored by a conservative approach [5].
The risk of complications depends on the shape of ingested objects; objects with sharp point or edges represent the greatest risk [6].
Long and thin objects hardly pass through the digestive tract and are more likely to be stucked. Generally, objects greater than 2 centimeters in diameter don’t pass through the pylorus and tend to be in the stomach, while objects longer than 5cm are usually identified in the duodenum upon further exploration [4].
Since there may be a long gap between the time of foreign body ingestion and incidence of symptoms, the diagnosis is somehow complicated [4].
Toothpick is usually used in the oral cavity and its characteristic features of – long, sharp ends, thin, and indigestible nature –can lead potentially to life-threatening complications if it is ingested [7,8]. The difficulty in detecting them on plain X-ray increases this potential risk [7].
Only 12% of patients could clearly remember the ingestion of the toothpick. This means that a large number of them don’t receive medical attention which leads to migration of the ingested object down the gastrointestinal tract and occasionally causes damage to the extra intestinal organs and vessels occasionally [9].
Damage caused by toothpick is often seen in men (88%).Most patients present with abdominal pain and symptoms often occur 1 to 15 days after ingestion [9].
The most common parts of the gastrointestinal tract damaged secondary to accidental ingestion of the toothpicks are duodenum and sigmoid colon.
Severe injuries may occur if the toothpick penetrates from gastrointestinal tract to nearby organs including: pericardial effusion and cardiac tamponade, liver abscess, duodenum fistulas and also vascular injuries [7].
About therapeutic interventions in patients referred because of foreign body ingestion; in 10-20% of cases, endoscopic intervention is indicated and surgery is required in 1% of cases [10]. Generally, decision about therapeutic interventions needed in these patients depends on several factors such as: the patient’s age, material ingested, location and number of the foreign body and the necessity of removing it and also technical abilities of the endoscopist [4].
The timing of intervention is also influenced by the risk of complications (perforation or obstruction) [4].
It’s recommended that sharp object be removed even in asymptomatic patients due to the risk of perforation and complication such as peritonitis and abscess [4]. The treatment of the choice depends on the anatomical location in which the object is lodged [1].
Most physicians prefer endoscopy because it reduces the need for surgery and it’s also cost effective, available and feasible to investigate other concomitant diseases [4].
As the final point, it’s important to consider foreign body ingestion as a differential diagnosis of abdominal pain with undiagnosed cause. Because of wide range of differential diagnosis of abdominal pain, it’s necessary to have clinical suspicion and precise clinical viewpoint to identify this incident as the cause of abdominal pain correctly [12,13].

![]()

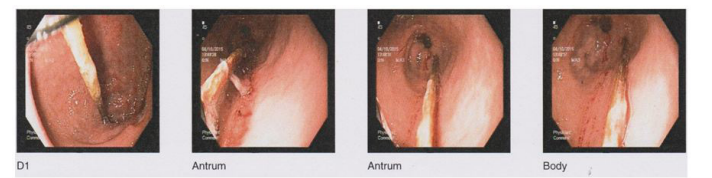 |
| Figure 1: Removing the ingested toothpick from duodenum |




































