Open Access
Research Article
Max Screen
ISSN: 2575-5501
Copyright: © 2018 Osman N. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Squamous cell carcinoma of the gallbladder is rarely reported, comprises less than 1% of all gall bladder cancer and portends a worse prognosis than the more common adenocarcinoma.
We report a 80-year-old female who presented with acute onset epigastric pain. She was operated on based on a presumptive diagnosis of acute on top of chronic cholecystitis with cholelithiasis according to clinical and ultrasonographic findings. Histopathological examination of the thickened wall of the gallbladder revealed well to moderately differentiated keratinized squamous cell carcinoma invading full wall thickness and infiltrating the liver. Further examinations revealed no other primary site for the tumour. Gallbladder cancer should be considered as part of the differential diagnosis in elderly patients presenting with cholecystitis
Keywords: Gallbladder; Squamous cell carcinoma; Cholecystitis
Gall bladder carcinomas (GBC) represent the fifth most common cancer of the digestive tract (2 - 4%) [1]. GBC is more common in women older than 50 years and usually of the adenocarcinoma type [1,2]. Pure primary SCC is rarely reported and accounts for less than 1% of all GBC [1].
Squamous cell carcinoma (SCC) of the gallbladder (GB) is usually detected at an advanced stage with infiltration of adjacent organs and hepatic metastases, has a low tendency towards lymph node metastases, rapid growth pattern and poor survival [2]. The overall prognosis of SCC is worse than adenocarcinomas and adenosquamous carcinomas [1]. The majority of the patients die around 6 months after diagnosis without radical surgery. Surgical intervention offers some possibility of long-term survival. The efficacy of radiotherapy and chemotherapy is debatable [3]. Abdominal ultrasonography (U/S) is the first diagnostic procedure performed for suspected biliary disease [4]. However, radiologic studies may be limited whereas GBC has overlapping symptoms with cholecystitis [4]. Most cases are not diagnosed preoperatively. Typically, a GB mass is found incidentally in patients presenting with nonspecific signs and symptoms that mimic acute cholecystitis. The proper diagnosis of GBC can only be confirmed by histopathological evaluation of the resected GB [1].
We present a case report of Saudi female with accidentally discovered pure SCC of the gallbladder with a vague presentation of calcular cholecystitis.
A 80-year-old Saudi female presented with persistent onset of epigastric pain and vomiting for one month prior to hospital admission in the year 2017. On physical examination she was acutely ill with respiratory distress and pleural effusion. She was afebrile (36.5 °C). Her pulse rate and blood pressure were 101/min and 115/60 mmHg, respectively. The abdomen was tender but there was no physical sign of peritonitis. Laboratory data showed leukocytosis, neutrophilia and anemia. Liver function tests showed total protein: 4.42 g/DL, albumin 2.63 d/DL, ALT:9.4 IU/L, AST: 14.1 IU/L, Alkaline phosphatase: 282 IU/L, total bilirubin: 0.864 mg/dL, and direct bilirubin: 0.460 mg/dL. Other serum chemistry profiles were unremarkable. The patient lacked general signs of malignancy such as weight loss or jaundice
Abdominal ultrasonography showed thickened gallbladder wall with multiple gall stones in favor of acute calcular cholecystitis without obvious mass. Computed tomography (CT) was not done preoperatively, as no suspicion found with ultrasonography. With the presumptive diagnosis of acute on chronic cholecystitis, the patient received supportive care and antibiotics. Then, she underwent laparoscopic cholecystectomy. During laparoscopy, anatomy was disturbed and GB was embedded in the liver which was very hard. So, conversion to laparotomy was made. Duodenum, omentum and transverse colon were dissected from GB. The fundus of GB found to be occupied with a mass partly hard and partly necrotic. Also, the liver bed found to be invaded. GB was opened accidentally and many stones were removed. Cholecystectomy was done with resection of that part of the liver that was hard and the specimen was sent to histopathology. No lymph nodes were enlarged.
Gross examination of the gallbladder revealed only wall thickening of 3.5cm. No lymph nodes were dissected. The liver part was received as three friable pieces of tissue, the largest was 8x8cm and the smallest was 4.5x3 cm (Figure 1).
Microscopic evaluation for the gall bladder revealed a well to moderately differentiated keratinized SCC invading full wall thickness to the serosal surface (Figure 2). Angiolymphatic invasion was present. The tumour lacked any glandular differentiation. The examined sections from the liver showed infiltration by keratinized moderately differentiated SCC with extensive areas of necrosis and fibrosis (Figure 3). Postoperative CT revealed multiple hepatic focal lesions at right lobe with intervening hypodense liver parenchyma. No evidence for primary tumour in colon, lung, kidneys, spleen, pancreas, adrenals or urinary bladder. No pathologically enlarged paraortic or mesenteric lymph nodes seen. All other examinations were negative for the primary origin of the squamous cell carcinoma and the patient was sent to an oncology hospital for further evaluation and treatment.
GBC is rare. In a population- based registry conducted by Ministry of Health in Saudi Arabia, the incidence rate of primary GBC was 1.5 for both females and males in the year 2013 [5].
GBC is asymptomatic at early stages. When symptomatic, the presentation is similar to biliary colic or cholecystitis [6]. If both are present in an elderly patient accompanied by weight loss and anorexia, gall bladder cancer should be considered [7]. Hepatic metastases are more frequent in SCC than adenocarcinoma of the gallbladder [1]. SCC is usually diagnosed when the tumour is large in size and locally advanced. SCC growth is faster, more aggressive and worse in prognosis than adenocarcinoma. [8]. On the contrary, a previous study reported that pure SCC of the gallbladder was less aggressive than adenocarcinoma [9].
SCC of the gallbladder is thought to arise from the basal cell layer of the epithelium. It is also hypothesized that it can arise from the squamous metaplasia or squamous differentiation of a pre-existing adenocarcinoma [1]. This suggests that chronic irritation from gallstones may trigger differentiation of gallbladder glandular cells into metaplastic squamous cells that would undergo malignant transformation. It was reported that about 12% of GBC has squamous metaplastic cells evident in adjacent mucosa [1].
Laparoscopy should not be done if gallbladder cancer is suspected. If during initial laparoscopy the diagnosis is suspected, conversion to an open laparotomy should be done for a curative resection [7].
A retrospective study on 26 patients with confirmed GBC, who initially had presumptive diagnosis of acute cholecystitis. Diffuse wall thickening was evident in 15 (57.6%) cases and 11 (42.3%) cases exhibited intraluminal mass [4]. On the other hand, 9 cases of SCC of the gallbladder were diagnosed by use of U/S-guided aspiration cytology out of 322 cases with gallbladder mass lesions (2.8%). Thus, cytology studies of biliary fluid should be investigated as a preoperative potential safe tool for the early detection and diagnosis of SCC of the gallbladder [6,10].
Pure GBC is rare. The initial diagnosis should be by abdominal U/S and CT. GBC should be suspected in elderly patients with diffuse thickening of GB wall. Radical resection of the gall bladder is the mainstay of treatment for patients with locally invasive SCC and offers the only chance for cure. The extent of tumour invasion at the time of diagnosis is the most important parameter for survival. For tumours discovered on histopathological evaluation after cholecystectomy, no further surgical treatment is needed. For advanced tumours radical resection is done [7]. Postoperative radiotherapy and chemotherapy may be used [7]. Moreover, immunotherapy, especially dendritic cell therapy is expected to improve survival especially in stage IV GBC [11].
There are no conflicts of interest.

![]()

 |
| Figure 1: Gross findings of resected gall bladder and liver: The wall of the gall bladder is thick (magnification x40). |
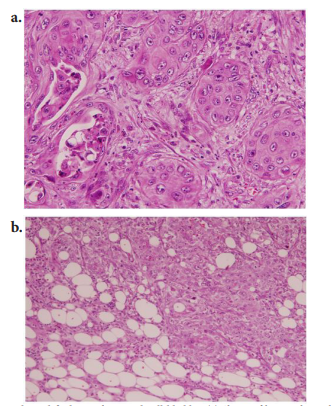 |
| Figure 2: Histological findings of resected gall bladder. (a) Sheets of large polygonal malignant squamous cells containing keratin (individual cells or keratin pearls) and intercellular bridges (hematoxylin and eosin staining, magnification x40). (b) malignant squamous cells infiltrate the serosal layer (hematoxylin and eosin staining, magnification x20) . |
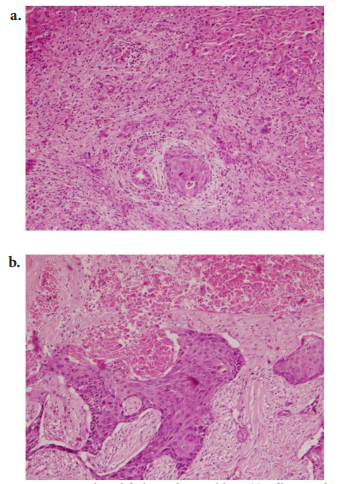 |
| Figure 3: Histological findings of resected liver. (a) infiltration of hepatic tissue by solid group of malignant squamous cells containing individual cell keratinization (hematoxylin and eosin staining, magnification x20). (b) infiltration of hepatic tissue by sheets of malignant squamous cells with wide areas of necrosis and fibrosis (hematoxylin and eosin staining, magnification x40) |




































