Open Access
Research Article
Max Screen
ISSN: 2639-9253
Copyright: © 2023 Francesca Rossi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background and Purpose: Ischemic stroke is a treatable medical emergency. The diagnosis of stroke is mainly clinical and not always so obvious. Intravenous thrombolysis treatment with altepase IV and endovascular treatment have been proved as fist-line beneficial options for eligible patients who have acute ischemic stroke. However, approximately 30% of patients who experience an acute neurological deficit compatible with ischemic stroke fall into the category of "stroke mimics".
Methods: We recruited prospectively all consecutive patients admitted to our emergency department for suspected acute ischemic stroke for 32 days, collecting for each patients a series of clinical and radiological variables. The study objective is to determine the frequency and the clinical characteristics of stroke mimics and the variables that predict mimics.
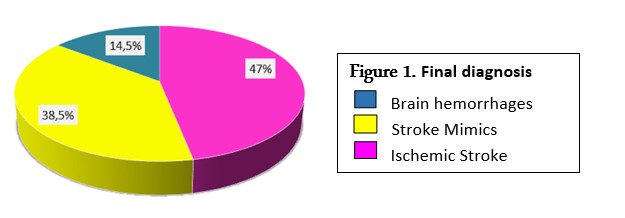
Results: Out of 96 patients (60% females), thirtyseven stroke mimics were identified, resulting in a frequency of 38.5%, versus 46.8% of ischemic stroke and 14.5% of brain hemorrhage. The main causes of stroke mimics were epileptic seizures, sepsis and brain lesions. Multivariate analyses show two clinical items that independently predicted the diagnosis of mimics stroke: altered consciousness and fever.
Conclusions: In a third of the patients with suspected stroke the presenting symptoms were due to conditions other than a cerebrovascular event. In an era of time-dependent reperfusion techniques, it is crucial that an accurate and prompt diagnosis is made: rapid identification of a stroke mimic prevents treatment with thrombolytics and the possible complications from such treatment, avoids unnecessary and costly investigations and inappropriate long-term prevention treatment.
Keywords: stroke; stroke mimics; emergency; diagnosis
Stroke is the second leading cause of death and the third one for disability worldwide for all ages, as well as the leading cause of disability in the elderly. Ischemic stroke represents the main subtype (80% of cases) and thrombo-embolic events are the main cause of acute ischemic stroke [1].
Over the last 15 years, a series of studies have been published showing that an early recanalization represents the most important modifiable predictive factor for the patient's outcome. Currently, options treatment for acute ischemic stroke are intravenous thrombolysis with altepase IV within 4.5 hours (as reported by the ECASS III [2] and IST-3 studies [3] and the Italian ISOSPREAD guidelines on prevention and therapy stroke) and mechanical thrombectomy within 6 hours, as reported by American Heart Association/American Stroke Association guidelines [4]. According to these studies, there are no longer any age or severity limits (both in the sense of mild stroke and in high severity) and other contraindications become less mandatory. Earlier treatment and recanalization is clearly associated with improved mortality rate and clinical outcome due to the prevention of neuronal ischemia. However, from the literature it emerges that about 20-30% of patients who access the Stroke Unit with a clinical presentation compatible with an ischemic cerebral event have a different discharge diagnosis, falling into the category of "stroke mimics" [5-7]. The term 'stroke mimics' is an "umbrella term" rather than a diagnosis: once the stroke diagnosis is excluded, in fact, the term refers to numerous nonvascular disease processes that manifest with acute neurologic deficit. The importance of a correct differential diagnosis lies not only in identifying the underlying pathology in order to guide a correct therapeutic process, but above all to avoid, where possible, that these patients receive thrombolytic treatment at the risk of bleeding side effects[8].
The most frequent diseases that cause stroke mimics are the following: migraine (aura) [9], seizures[10], Todd's paralysis, syncope, dizziness, hypo-hyperglycaemia [11], metabolic imbalances, severe anemia or other conditions that determine cerebral hypoperfusion, hypertensive crisis, sepsis, peripheral neuropathies, Guillain-Barré or Miller-Fisher syndrome, degenerative neurologic disorders, multiple sclerosis [12], space-occupying brain injuries (e.g neoplasms [13], subdural hematomas, brain abscesses, arteriovenous malformations), somatic conversion disorders. These conditions must be quickly considered and therefore excluded or confirmed by physicians, in order to correctly and promptly manage patients with real ischemic stroke and at the same time, formulate a correct differential diagnosis. Several studies [14,15] have evaluated the stroke mimics rate in different settings and have identified clinical and imaging features associated with a final diagnosis of stroke mimic, including clinical symptoms, vital signs, neurological signs, stroke severity, and even neurological impairment at discharge. The purpose of our study was to answer two questions: what proportion of patients with suspected stroke has a stroke mimics? Which diseases causes stroke mimics? What variables can predict whether a patient has a stroke mimics?
This was an observational, prospective study of consecutive patients more than or equal to 18 years of age, admitted to the emergency department at the Policlinic San Martino Hospital in Genoa, Italy, from 10/09/2019 to 11/10/2019 (32 days total) with signs or symptoms of suspected acute ischemic stroke: aphasia, amaurosis, diplopia, dizziness, bilateral blindness, alternate syndromes, hemiparesis-hypoaesthesia, dysarthria, ataxia, dysphagia, impaired consciousness. The primary source of study patients came from the emergency department physicians and triage staff. Some cases of acute neurological syndrome are not reported by triage, but other overlapping sources (informatics database of the emergency department, stroke unit, and neurology ward) were used to ensure that all patients with brain attack were identified. Each patient was examined by the emergency physician and neurologist, except for five patients in whom the diagnosis of stroke mimics was obvious from the emergency physician's assessment. The decision to stop the study after 32 days was dictated by the fact that the percentage of stroke mimics detected was substantially higher than other clinical trials and it was decided at regional level to modify the protocol of "stroke centralization". Hence the desire to perform a preliminary longitudinal study, with the desire to expand the number after the revision of the Stroke Protocol that was scheduled for December 2019. Unfortunately, the advent of endemic disease from SarsCov-2 temporarily froze the project.
All patients provided informed consent for data processing. For this type of study, further specific consent was not required. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ischemic stroke has been diagnosed since the medical history and the examination were completely typical for a vascular brain event and there was supportive or noncontradictory brain imaging. In unifying the results obtained in classes, transient ischemic attacks were included in the definition of ischemic stroke, primarily because they are both vascular events, secondly because the onset of a TIA is an additional risk factor for the development of stroke. A mimics stroke was defined when clinical, anamnestic and radiological-instrumental details suggested a non-vascular etiology and another more convincing clinical explanation. In the definition of brain hemorrhage both intraparenchymal and subarachnoid hemorrhages have been grouped.
For each patients, information collected included:
1) demographic variables (age and sex) and modality of presentation in hospital (by ambulance or by private vehicle).
2) past medical history (including previous stroke or transient ischemic attack), heart disease, other comorbidity (e.g. neoplasm, degenerative neurologic disorders) vascular risk factors (smoking, high blood pressure - defined if reported in medical history or if antihypertensive therapy has been undertaken-, diabetes mellitus - defined if reported in medical history or if hypoglycaemic therapy has been undertaken-, dyslipidemia - defined if reported in anamnesis, or if LDL cholesterol value ≥120 mmol/L or triglycerides ≥150mmol/L [16], or finally if therapy has been undertaken-), atrial fibrillation, anticoagulant drugs, antiplatets drugs;
3) risk factors for stroke mimics (cognitive impairment, medical history of migraine, epilepsy, malignancy or psychiatric disorders);
4) history of the present event, including nature of the neurological symptoms and change in symptoms over time;
5) general examination, including fever, blood pressure, heart rate, oxygen saturation, signs in other systems;
6) laboratory findings (eg, anemia, hypoglycaemia, hyperglycaemia, ionic changes, elevated C-reactive protein values, hyperammonemia…)
7) neurological examination, which has been divided into:
-motor deficits: paresis, ataxia, dysphagia
-speech disorders: aphasia, dysarthria
-cognitive deficits: spatial disorientation, apraxia, hemisomatoagnosia
-alterations of the state of consciousness: sleepy state or coma, confusion or agitation
-negative or doubtful neurological examination
8) radiological findings (CT, MRI) and other instrumental investigation useful for final diagnosis (eg, EEG, color doppler)
Statistical analyses were performed using IBM SPSS for Windows version 21.0, in which all the clinical parameters collected in an online database were recorded and accessible only to the personnel involved in the study. Once the cases of hemorrhagic strokes were excluded from the total sample (96 patients), we dichotomized the final diagnosis in stroke or mimics stroke to allow the analysis of the clinical characteristics that distinguished between the two conditions. The differences between the two groups were assessed using descriptive statistics and standard significance tests. The characteristics of the patients for the univariate analysis are compared in relation to all the final results used the Chi-square test. Multivariate analyses was performed to determine the clinical factors that independently predicted mimics or stroke; based on a predictive model, in which the variables for the statistical analysis were selected using a well-established penalized maximum likelihood regression model implemented in the R package glmnet [17].
We recorded a total of 96 patients who entered the emergency room for a total of 32 observation days, with signs or symptoms compatible with suspected ischemic stroke. The patients were aged between 22 and 99, of which 39 were men (40%) and 57 women (60%). The final diagnosis was stroke mimics in 37 patients (38.5%), ischemic stroke in 45 (46.8%) and brain hemorrhages in 14 (14.5%), like in Figure1.
The causes of stroke mimic are detailed in Table 1. According to the literature, the most frequent cause was an epileptic seizure, in 10 patients (27%): one Todd's paralysis, a crisis in the course of fever and dysionia, two states of epileptic illness, some partial crises. The second most relevant cause was sepsis in 8 patients (21%), whose the most frequent site was the chest. Newly diagnosed brain lesions initiated with a ictal-like clinic represents 13.5% of mimics: a mesencephalic pontocavernoma, a glioblastoma, two cases of cerebral metastasis and an atypical meningioma. Metabolic changes were found to be present in 5.4% of cases of severe glycemic changes (one patient has 42 mmol/L and another patient 729 mmol/L, both diabetics), and in 2.7% of cases of symptomatic hyponatremia (125 mmol/L). A patient with mimics stroke was subjected to thrombolysis: she was a 75-year-old woman with many cardiovascular risk factors (arterial hypertension, diabetes mellitus, a previous stroke, epileptic note, on antiplatets therapy) who presented level reduction of consciousness with right upper limb paresis and smoothing of the genius nose sulcus (NHISS 15). The final diagnosis was found to be a complex partial epileptic seizure. Control brain CT post thrombolysis was negative for bleeding.
Table 2 describes all the clinical characteristics of the patients recruited in the study and each variable taken into consideration (eg. Sex, cardiovascular risk factors, drugs, comorbilities..), distinguishing between mimics stroke and stroke, once excluded from the totale of 96 patients the 14 cases of brain hemorrhage. .
Table 3 includes only significant data: There was no significant relevance between the two groups as regards sex, presentation modality with self-presentation or ambulance (taking into account however that this was the only variable of the study with some missing data), previous stroke, cardiovascular risk factors, antiplatelet or anticoagulant therapy, a history of headache, psychiatric disorders or cognitive impairment. A mimics was more likely if there was a known history of epilepsy (p < 0,05), if the patient had alterations of the state consciousness (p < 0,05), fever (p < 0,05), changes in blood glycemia (p = 0,05) and if neurological examination was negative (p < 0,01). Stroke was more likely if the patient had motor deficits (p < 0,01), cognitive deficits and when CT was diagnostic (p < 0,05).
After multivariate analyses (Table 4 and Figure 2), two clinical items independently predicted the diagnosis of mimics stroke: the presence of altered consciousness and fever; conversely, the presence of motor deficits predicted ischemic stroke.
In our study, out of 96 patients admitted to the emergency room with a diagnosis of suspected ischemic stroke, more than a third of the patients (38.5%) had a conditions other than a cerebrovascular event: a mimics stroke. This data is somewhat higher than many hospital-based studies (eg, 1.4% to 15%), perhaps by their different selective entry criteria and because they were retrospecitive, with more bias [18,19]. Other studies instead report stroke rates similar to ours. A very large but retrospective study about stroke mimics was published in 2013: the goal was to determine the presentation modalities and the incidence of mimics stroke. The analysis included 8,187 patients of which 30% had a stroke mimic. Patients with a stroke mimic were younger, preferentially women, patients without any risk factors and often arrived to the emergency department via personal vehicle. In a study of the bedside clinical assessment of suspected stroke, Hand et al. showed that an exact time of onset, definite focal symptoms, a high National Institute of Health Stroke Scale (NIHSS) score, being able to lateralise the signs to the right or left side of the brain and being able to determine a clinical stroke syndrome predicted a stroke, while cognitive impairment and abnormal signs in other systems predicted a mimics[5]. Garg et al. [15] made diagnosis of stroke mimics in 27.9% of patients, by the absence of infarction on post-thrombolysis DWI obtained within 24-72 hours from treatment; mimics were younger, with fewer vascular risk factors and had lower glucose on presentation. But in prior studies, patients without neuroimaging evidence of acute ischemic infarction may have been excluded from the stroke mimic group if the clinical diagnosis was suspected to be a cerebrovascular etiology [20,21]. Finally, with regard to the previous experience of our hospital, in 2018 was published a prospective study which enrolled, for one year, patients diagnosed with suspected cerebral ischemic event with the main objective of identifying thrombolysis rates and at the same time the causal factors of a possible non-treatment. Out of a total of 819 patients entering the emergency room, only 459 patients had a real ischemic event and the remaining 359 cases (43.8%) had a diagnosis of hemorrhagic stroke, TIA or stroke mimics [22].
Our study is in agreement with the literature regarding the conditions that mimics stroke: epileptic seizures, sepsis, brain injuries, syncope, migraine and metabolic changes are frequently reported in previous studies. On the contrary, neuropathies or iatrogenic causes are less frequent. We report that seizures are one of the most commonly diagnosed stroke mimics in patients presenting to our emergency department. The development of a focal weakness after seizures was described by Robert Bentley Todd in 1849 and is thought to occur through over-activity and subsequent exhaustion of the primary motor cortex. When other areas of the brain are affected by seizure, other transient deficits can manifest, such as dysphasia, sensory symptoms or visual field deficits.
Our analysis has shown a greater probability of being faced with a mimics stroke in the presence of a history of epilepsy, if the patient has impaired consciousness, fever or glycemic changes and if the neurological objective examination is negative or doubtful. The predictive model identified two clinical independent variables to predict the diagnosis of mimics stroke: the presence of altered consciousness and fever. Also taking into account that the percentage of stroke mimics patients with cardiovascular risk factors and previous ischemic events is substantially similar to the group of ischemic strokes, the need for neurologists and emergency physicians to perform an accurate assessment of the patient to reach a correct diagnosis of ischemic stroke and to start the patient to thrombolytic therapy is strengthened.
Compared to other studies, we believe that ours can be useful because the main variables that can help physicians to make a differential diagnosis between mimics and stroke are clinical. The stratification of the risk of the patient with suspected ischemic stroke is essential to carry out the correct treatment in the times indicated and reduce the risk of brain damage and consequent disability. To make a differential diagnosis between stroke and stoke mimics it is necessary to take into account various factors over the clinical examination, the help of laboratory and radiological tests: age and other demographic data, vascular risk factors, onset and progression, duration of symptoms, nature of symptoms ("positive" versus "negative), precipitating factors and associated symptoms.
Lastly, we decided to apply the FABS score, published by Goyal and colleagues in 2016 [23], to our patients. The score was create to screen and stratify stroke mimics from ischemic stroke and is based on six variables (one point for each): absence of facial droop, negative history of atrial fibrillation, age < 50 years, systolic blood pressure < 150mmHg at presentation, history of seizures and isolated sensory symptoms without weakness at presentation. According to Goyal’s results, who calculated the probabilities in terms of percentage, as the number of points of the Score increases, it increases from the probability of being in front of a mimics. We added a statistical comparison between stroke mimics and ischemic stroke, using the χ2 test: a mimics was more likely (p = 0,01) when FABS Score is 3 (Table 5).
Ischemic stroke is a medical emergency. Taking into account that the approved recanalization treatments are intravenous thrombolysis with rt-PA within 4.5 hours of onset (9 in selected patients) or, alternatively, mechanical thrombectomy or intraarterial thrombolysis (in selected patients with major stroke and cerebral artery occlusion medium or severe contraindications to thrombolysis) within 6 hours of symptom onset, a correct and prompt diagnosis is essential. However, the diagnosis of ischemic stroke is mainly clinical and not always so obvious. Despite the aid of radiological, laboratory and instrumental investigations, the emergency medical approach remains basic, to perform rapid differential diagnostics and to guide the subsequent therapeutic diagnostic process. For these reasons, it is mandatory that the emergency doctors know all the possible causes of mimics stroke.
We thank the triage staff of our Emergency Department for assisting with patient recruitment.
None
The authors declare that they have no conflict of interest.

![]()

 |
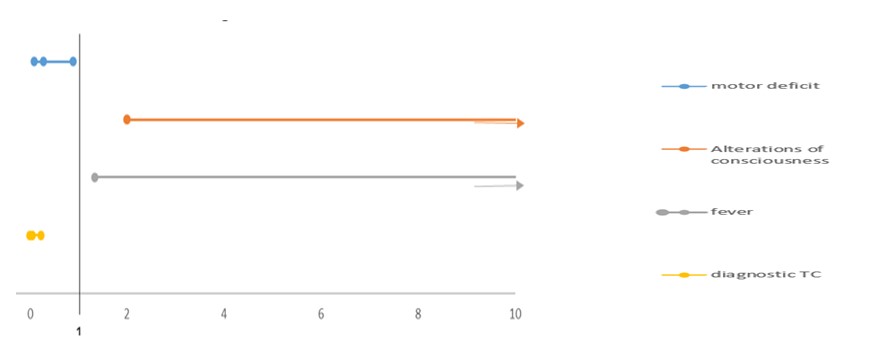 |
| Figure 2: The predictive factors of stroke mimics: aleterations of consciousness and fever |
Condition |
Total Number (%) |
Epilepsy |
10 (27%) |
Sepsis |
8 (21%) |
Brain lesions |
5 (13.5%) |
Migraine |
3 (8.1%) |
Syncope |
3 (8.1%) |
Peripheral neuropathy |
2 ( 5.4%) |
Hypo – hyperglycaemia |
2 ( 5.4%) |
Hypertensive crisis |
2 ( 5.4%) |
Hyponatremia |
1 (2.7%) |
Iatrogenic |
1 (2,7%) |
Total |
36 (100%) |
|
all patients |
mimics stroke |
ischemic stroke |
|||
Median age |
80 (22-99) |
79 (22-93) |
80 (43-99) |
|||
Female sex |
51 |
(62,2%) |
22 |
(29,5%) |
29 |
(64,4%) |
Self-presentation |
11 |
(17,5%) |
8 |
(24,2%) |
3 |
-10% |
Medical hystory and risk factors |
|
|
|
|
|
|
Previous stroke |
21 |
(25,6%) |
9 |
(24,3%) |
12 |
(26,7%) |
Smoke |
12 |
(14,6%) |
4 |
(10,8%) |
8 |
(17,8%) |
Hypertension |
46 |
(56,1%) |
19 |
(51,4%) |
27 |
-60% |
Diabetes mellitus |
14 |
(17,1%) |
7 |
(18,9%) |
7 |
(15,6%) |
Dyslipidemia |
15 |
(18,3%) |
7 |
(18,9%) |
8 |
(17,8%) |
Heart deseases |
8 |
(9,8%) |
5 |
(13,5%) |
3 |
(6,7%) |
Atrial fibrillation |
17 |
(20,7%) |
6 |
(16,2%) |
11 |
(24,4%) |
Anticoagulant drugs |
16 |
(19,5%) |
8 |
(21,6%) |
8 |
(17,8%) |
Antiplatets drugs |
34 |
(41,5%) |
17 |
(45,9%) |
17 |
(37,8%) |
Epilepsy |
5 |
(6,1%) |
5 |
(13,5%) |
0 |
0% |
Migraine |
4 |
(4,9%) |
3 |
(8,1%) |
1 |
(2,2%) |
Psychiatric disorders |
1 |
(1,2%) |
1 |
(2,7%) |
0 |
0% |
Cognitive impairment |
13 |
(15,9%) |
8 |
(21,6%) |
5 |
(11,1%) |
Neurological examination |
|
|
|
|
|
|
Speech disorders |
38 |
(46,3%) |
13 |
(35,1%) |
25 |
(55,6%) |
Motor deficits |
49 |
(59,8%) |
13 |
(35,1%) |
36 |
-80% |
Cognitive deficits |
13 |
(15,9%) |
2 |
(5,4%) |
11 |
(24,4%) |
Alterations of consciousness |
7 |
(8,5%) |
6 |
(16,2%) |
1 |
(2,2%) |
Negative/doubtful neurological examination |
16 |
(19,5%) |
12 |
(32,4%) |
4 |
(8,9%) |
Other findings |
|
|
|
|
|
|
Fever |
7 |
(8,5%) |
6 |
(16,2%) |
1 |
(2,2%) |
Hypo - hyperglycaemia |
3 |
(3,7%) |
3 |
(8,1%) |
0 |
0% |
Diagnostic CT |
29 |
(35,3%) |
5 |
(13,5%) |
24 |
(53,3%) |
|
All patients |
Mimics Stroke |
Ischemic stroke |
Significant |
|||
Past Medical hystory and risk factors |
|
|
|
|
|
||
Epilepsy |
5 |
(6,1%) |
5 |
(13,5%) |
0 |
(0%) |
0,01 |
Neurological examination |
|
|
|
|
|
|
|
Motor deficits |
49 |
(59,8%) |
13 |
(35,1%) |
36 |
(80%) |
0,00 |
Cognitive deficits |
13 |
(15,9%) |
2 |
(5,4%) |
11 |
(24,4%) |
0,02 |
Alterations of consciousness |
7 |
(8,5%) |
6 |
(16,2%) |
1 |
(2,2%) |
0,02 |
Negative/doubtful_neurological examination |
16 |
(19,5%) |
12 |
(32,4%) |
4 |
(8,9%) |
0,00 |
Other findings |
|
|
|
|
|
|
|
Fever |
7 |
(8,5%) |
6 |
(16,2%) |
1 |
(2,2%) |
0,02 |
Hypo - hyperglycaemia |
3 |
(3,7%) |
3 |
(8,1%) |
0 |
(0%) |
0,05 |
Diagnostic CT |
29 |
(35,3%) |
5 |
(13,5%) |
24 |
(53,3%) |
0,00 |
Variables |
OR |
95% Cis |
Motor deficit |
0.28 |
0.09 - 0,89 |
Alterations of consciousness |
29.58 |
2.00 - 1546,91 |
Fever |
16.48 |
1.33 - 782,94 |
Diagnostic CT |
0.04 |
0.00 - 0,22 |
FABS Score |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
Ischemic Stroke |
4 |
10 |
20 |
9 |
2 |
0 |
0 |
Mimics Stroke |
1 |
2 |
11 |
17 |
4 |
2 |
0 |
Probability of Mimics (χ2 test) |
0,24 |
0,03 |
0,17 |
0,01 |
0,27 |
0,11 |
- |
Probability of Mimics (%) |
0,2 |
0,16 |
0,35 |
0,65 |
0,66 |
1 |
- |




































