Open Access
Research Article
Max Screen
ISSN: 2639-9253
Copyright: © 2021 Legramante JM. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: Since December 2019, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic has reached catastrophic proportions. Many patients required admission to the intensive care units (ICU), stressing the capacity of public health systems. The workload in the emergency departments (ED), especially the ICU, has dramatically increased, creating a pressing need to optimize resources through risk stratification for critically ill COVID-19 patients. For this reason, prognostic tools and biomarkers were urgently needed. No data are still available on the role played by new biomarkers as mid regional-proadrenomedullin (MR-proADM) in the clinical management and risk stratification of ICU patients with COVID-19-related pneumonia. To fill in this gap, the main objective of this study is to assess the role of MRproADM as compared with SOFA clinical score and with the most used biomarkers in stratifying the in-hospital mortality risk in COVID-19 patients affected by pneumonia and complicated with acute respiratory distress syndrome (ARDS).
Methods: Data from 66 consecutive patients admitted to the emergency department with a diagnosis of COVID-19-induced interstitial pneumonia and ARDS were analyzed. Epidemiological, demographic, clinical, laboratory, treatment, and outcome data were assessed, along with the SOFA score. C-reactive protein (CRP), interleukin-6 (IL-6), procalcitonin (PCT), and mid-regional proadrenomedullin (MR-proADM) blood levels were also evaluated at the admission.
Results: Pooling all the variables together in a multivariate analysis and considering the whole observation period, CRP and the SOFA score appeared to be the only independent predictors of death. When we applied the same analysis to the group of patients who survived versus patients who died in the first week of disease, MR-proADM was the only independent predictor of mortality in the short-term period.
Conclusion: This study shows that MR-proADM seems to represent the most powerful biomarker for predicting death in critical COVID-19 patients where the outcome can happen earlier, within one week, thus representing a good predictor for disposition of patients from emergency department to ICU.
Keywords: COVID-19; Biomarkers; MR-proADM; Pneumonia
List of abbreviations: AUC: Area under the ROC Curve; CAP: Community-Acquired Pneumonia; CMIA: Chemiluminescent Microparticle Immunoassay; COVID-19: Coronavirus Disease 2019; CRP: C-Reactive Protein; ED: Emergency Department; ICU: Intensive Care Unit; IL6: Interleukin-6 (IL-6); MR-proADM: Mid-Regional proadrenomedullin; PCT: Procalcitonin; PSI: Pneumonia Severity Index; ROC: Receiver Operating Characteristic Curve; RT-PCR: Real-Time Reverse Transcription-Polymerase Chain Reaction; SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2; TNFα: Tumor Necrosis α; WHO: World Health Organization
Since December 2019, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic has spread all over the world and reached catastrophic proportions. The disease caused by SARS-CoV2 has been named COVID-19 (coronavirus disease 2019). The clinical spectrum of SARS-CoV-2 infection appears to be wide, encompassing asymptomatic infection, mild upper respiratory tract illness, and severe viral pneumonia with respiratory failure. Most of these latter patients required admission to the ICU, stressing the capacity of public health systems and resulting in a high mortality rate. This situation is complicated by the fact that the nonspecific clinical features of severe COVID-19 pneumonia make it difficult to distinguish it from other causes of severe pneumonia [1,2].
As a result, the workload in emergency departments, especially intensive care units (ICUs), has dramatically increased, creating a pressing need to optimize resources through risk stratification for critically ill COVID-19 patients.
Since predicting the trajectory of the illness at symptom onset is difficult and sometimes the patients’ clinical condition tends to worsen abruptly, prognostic tools and biomarkers are urgently needed. However, to date, there is no specific biomarker for identifying viral pneumonia that has a high sensitivity and specificity [3]
C-reactive protein (CRP) is one of the most commonly used biomarkers to evaluate inflammatory processes, but it does not have a high sensitivity for community-acquired pneumonia (CAP). While a high CRP value (>100 mg/L) can indicate a severe bacterial infection, lower values are common in both viral infections and noninfectious diseases [4], thus excluding this marker from being useful for pinpointing etiology, at least when used alone.
Procalcitonin (PCT) is another biomarker that is widely used as an aid for diagnosing bacterial infection and managing antibiotic therapy. It is produced by the C cells in the thyroid and during infection, the CALC-1 gene is activated and upregulated to increase the production of PCT in endocrine glands and many parenchymal tissues [5]. PCT can predict microbial etiology in pneumonia [6]. On the other hand, in patients with a high PSI (classes III-V), PCT has proven to be a good prognostic marker rather than a diagnostic marker [7].
In an attempt to distinguish between the different etiologies of CAP, Kruger et al. reported that PCT, CRP, and white blood cell count values were significantly higher in CAP patients whose pneumonia had a typical bacterial etiology than in cases with an atypical bacterial or viral etiology [8].
Mid-regional proadrenomedullin (MR-proADM), a more stable fragment of the rapidly degrading active adrenomedullin (ADM) peptide, is a promising biomarker indicating endothelial dysfunction and thus predicting severity and long-term adverse outcomes in CAP. In 2006, Christ-Crain et al. showed that the level of MR-proADM, in contrast to CRP levels and leukocytes, increased in tandem with CAP severity [9]. In addition, MR-proADM has already been positively assessed for its ability to predict unfavorable outcomes in patients with influenza virus-induced pneumonia [10]. Moreover, mid-regional proadrenomedullin has been recently reported to be able to stratify the clinical risk in patients affected by CAP [11]. Therefore, as demonstrated in other studies, MRproADM obtained within 6 hours from arrival at the hospital has considerable prognostic value, independently of the causal agent of CAP and, if associated with PSI and CURB-65, it improves prognostic accuracy [11,12]. Furthermore, MR-proADM plasma concentrations increase in response to deteriorating microcirculatory integrity and the resulting capillary leak, which represent the first step towards an alteration of the endothelial barrier function [13]. Concerning this aspect, a recent study has shown that Adrenomedullin RNA blood expression was significantly higher in patients with severe COVID-19 than in patients with less severe disease [14].
Interestingly, Li H. et al. [15] hypothesized that in critical patients with COVID-19-related pneumonia, the integrity of the epithelial-endothelial barrier was severely interrupted, describing a particular syndrome denominated “viral sepsis”. Recent studies also show that proinflammatory cytokines and chemokines such as tumor necrosis factor-α (TNF- α) and interleukin-6 (IL-6) were significantly elevated in COVID-19 [16,17] and that this cytokine storm might play a role in the pathophysiology of SARS-CoV-2 infection [18].
Despite the many findings reported so far and even though recent studies have reported a good predictor value for MR-proADM in patients with pneumonia COVID-19 related [19,20], no data are still available for this biomarker in the clinical management and risk stratification of ICU patients with severe viral pneumonia and acute respiratory distress syndrome (ARDS) related to COVID-19.
To fill in this gap, the main objective of this study is to assess the role of MR-proADM as compared with SOFA clinical score and with the most used biomarkers in stratifying the in-hospital mortality risk in COVID-19 patients affected by pneumonia and complicated with ARDS.
The present study has an observational, retrospective single-center design. Data from 66 consecutive patients admitted to the Emergency Department of Policlinico Tor Vergata (Rome, Italy) from March to May 2020 with a diagnosis of COVID-19-induced interstitial pneumonia and ARDS were analyzed. The study was approved by the Local Ethics Committee (approval number 87/20) and was performed in accordance with the Declaration of Helsinki. Written informed consent was waived due to the rapid emergence of this infectious disease.
A diagnosis of COVID-19 was made by detecting the SARS-coronavirus 2 in respiratory specimens (collected via nasopharyngeal swab) and through radiological imaging, in accordance with WHO interim guidelines.
All patients recruited were admitted to the ICU.
Adult patients aged more than 18 years were included in the present study, all affected by a SARS-CoV-2 infection with respiratory failure at the time of their admission.
For patients in the ICU, the epidemiological, demographic, clinical, laboratory, treatment, and outcome data were extracted from the electronic clinical records and compiled (Table 1). The Sequential Organ Failure Assessment (SOFA) score was calculated due to its role in clinically characterizing infected patients using the Third International Consensus Definitions for Sepsis and Septic Shock [21].
Either chest X-rays or computed tomography scans were performed, depending on the physician's clinical assessment, and these were further reviewed by the emergency department’s radiologist. When necessary, analyses of blood culture, sputum, urine, bronchial aspirate, and/or bronchoalveolar samples were also performed.
The final diagnosis was considered as that provided by the ICU physician at the time of discharge. A patient follow-up was performed at 28 days.
All baseline blood samples were collected immediately after ED admission. For serum and plasma specimens, blood samples were rapidly centrifuged upon arrival to the laboratory at 4500 xg for 5 minutes.
Blood examinations evaluated in the present study were C-reactive protein (CRP), interleukin-6 (IL-6), procalcitonin (PCT), and mid-regional proadrenomedullin (MR-proADM).
CRP (normality value < 5 mg/L) levels were measured in serum using an Abbott ARCHITECT c16000 (Abbott, North Chicago, USA) clinical chemistry analyzer. IL-6 (normality value < 50 pg/mL) was detected in serum by IMMULITE 2000XPi (Siemens Medical Solutions Diagnostics, USA), using a solid-phase, enzyme-labeled, chemiluminescent sequential immunometric assay.
PCT (normalityvalue< 0.5 ng/mL) was detected in serum via Architect BRAHMS PCT assay. The Abbott ARCHITECT i2000SR is a chemiluminescent microparticle immunoassay (CMIA). MR-proADM (normality value < 0.55nmol/L) was measured, using a time-resolved amplified cryptate emission assay on EDTA plasma samples (TRACE BRAHMS MR-proADMKryptor, BRAHMS AG, Hennigsdorf, Germany). All biochemical tests, with the exception of IL-6, were performed with a turnaround time of 1 hour.
The primary endpoint was the one-week mortality rate, which represents the mortality mainly due to the SARS-CoV-2 infections, and the secondary endpoint was the 28-day mortality rate, which is likely influenced by comorbidities and over infections
Associations between candidate variables and mortality were assessed using both univariate and multivariate logistic regression analyses, and odds ratios were calculated. The following variables were included in the multivariate logistic regression: MRproADM, CRP, PCT, IL-6 and SOFA score. Data on the included variables were available for all enrolled patients (no missing values). The discriminatory power of the analyzed variables for predicting mortality was tested by means of a receiver operating characteristic (ROC) curve analysis with area under the ROC curve (AUC) determination.
For the logistic regression, variables were dichotomized according to cut-off values either commonly identified in the published literature or derived during the data analysis for this study, using the Youden index arising from the ROC curve analysis. Survival curve differences with MR-proADM cut-off set to 2,5nmol/L were tested using log-rank test.
All analyses were performed with R software version 3.6.0. Tests were considered statistically significant if they yielded two-tailed p-values of < 0.05.
The final study population consisted of 51patients (15 of the 66 included patients were excluded due to concomitant bacterial infections) enrolled from March to May 2020 during the SARS-CoV-2 pandemic.
The demographic and clinical characteristics of the study populations are summarized in Table 1. The patient population had a median age of 69 years and the comorbidities and mortality rates are listed in Table 1.
The characteristics of COVID-19 patients who died within one week in comparison to those patients who died after the first week are reported in Table 2 and did not show significant differences.
Table 3 shows the results of the univariate analysis performed to investigate the possible predictive role of biomarkers and the SOFA score in risk stratification of patients with severe respiratory failure and COVID-19-related pneumonia. All biomarkers had a strong association in predicting overall mortality, with the exception of PCT and IL-6, which showed a weaker predictive power (Table 3).
In the ROC analysis for survival, the AUC was higher for MR-proADM and SOFA when compared to the other biomarkers analyzed (Figure 1 and Table 3).
The important role of MR-proADM as predictor of mortality in COVID-19 patients affected by ARDS and admitted to ICU is further confirmed by the survival curve (Figure 2).
Pooling all the variables together in a multivariate analysis and considering the whole observation period, CRP and the SOFA score appeared to be the only independent predictors of mortality in patients affected by severe COVID-19-related respiratory failure (Table 4).
When we applied the same analysis to the group of patients who survived versus patients who died in the first week of disease, MR-proADM was the only independent predictor of mortality in the short term (Table 4).
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) outbreak has had an enormous impact worldwide. Although most patients infected by SARS-CoV-2 had only a mild illness, about 5% of patients suffered severe lung injury or even multi organ dysfunction [22], requiring ICU admission.
This means that emergency departments have seen a dramatic increase in their workload, triggering a consequent need to optimize resources, and this must necessarily include the decision to hospitalize only seriously ill patients in the ICU.
The utilization of biomarkers to quickly stratify risk in patients with pneumonia and other infections upon admission to the emergency department has been widely described in recent years [12,23,24]. In previous studies, we showed that MR-proADM is effective in risk stratification for patients affected by community-acquired pneumonia (CAP), as well as in promptly determining the appropriate level of care in the emergency department [11,25].
To our knowledge, this is the first study focused on the behavior of new biomarkers as MR-proADM in the clinical history of patients affected by COVID-19-related pneumonia with ARDS and admitted in ICU, paying special attention to their ability to stratify the risk in these patients. On the other hand, previous studies have already evaluated the role of CRP and PCT in patients with COVID-19-related SARS [26-28].
We have evaluated the predictive values of the biomarkers considered in this study in relation to the established outcome. The SOFA clinical score has also been included. While MR-proADM, CRP, and the SOFA score showed a good ability to stratify risk in our critical patients with COVID-19-related pneumonia, PCT and IL-6 seem to have a lower predictive power for death in these same patients. This is evident in the AUCs depicted in Figure 1 and in the survival analysis performed in Figure 2.
Our results are in line with previous studies in which the predictive value of biomarkers was tested in patients affected by CAP. Infact, while MR-proADM has been considered a useful tool for risk stratification in patients affected by bacterial pneumonia [9,11,12], PCT proved to be less effective in predicting death and was therefore instead considered as a useful diagnostic tool for tailoring antibiotic therapy [9,29,30].
CRP is usually considered as a non-specific marker of acute inflammation that may possibly be influenced by several other factors [9,31]. Conversely, IL-6 is often considered a useful predictor of mortality in patients affected by CAP [32], even though its widespread use is limited due to some clinical problems caused by its short plasma half-life and the presence of blocking factors [33].
In our study, the SOFA score proved to be a useful tool for predicting severity and mortality in patients affected by SARS-CoV-2; its usefulness has already been shown in patients affected by community-acquired and healthcare-associated pneumonia [34].
With regard to the biomarkers analyzed, MR-proADM shows, at least, the same efficacy as the SOFA score in predicting severity and mortality in patients affected by COVID-19-related pneumonia with ARDS. This is a relevant result because the measurement of MR-proADM levels is less time-consuming for emergency physicians, thus allowing for early risk stratification in severe patients in a setting like an emergency department, where time and defining the appropriate level of care are vital.
The results of this novel study emphasize the role of biomarkers as a useful tool for emergency physicians in the early risk stratification of severe patients, even in the age of COVID-19. Diagnostic and predictive value is likely to increase only after the most effective combination of scores and biomarkers has been established, or even by utilizing a panel of biomarkers, particularly in severely ill patients [35,36]. For these reasons, it is important to know how biomarkers behave in response to defined diseases such as SARS-CoV-2.
Even though this study has a limited sample size, we must consider that it is focused on very critical patients requiring ICU ad- mission and thus representing only a small fraction of the total. Therefore, the number of patients enrolled is not negligible.Fur- thermore, it is notable that even with limited sample size significant results were found for some of the analyzed variables, possibly suggesting their strong prognostic effect in the general population.
Patients were recruited in only one hospital. Therefore, it would be desirable to extend the study to multiple centers to increase the number of enrolled patients, in order to confirm our results.
Further studies would also be needed to investigate the possible stratification of patients by age group, comorbidities, and other variables, which was not possible in our study given the small sample size.
This study, which to our knowledge, is the first to evaluate the behavior of the MR-proADM in the clinical management of critical SARS-CoV-2 patients in the emergency department, shows that all the biomarkers utilized can help the physician make decisions regarding severely ill ICU patients. However, MR-proADM seems to represent the most powerful biomarker for predicting death in critical patients where the outcome can happen earlier, within one week, thus representing a good predictor for disposition of patients from emergency department to ICU. It seems particularly useful to predict who will die from COVID-19 instead of pa- tients that will die with COVID-19, meaning due to possible complications of the disease, such as co-infections, heart failure, etc.
It is evident, however, that biomarkers will always oversimplify the interpretation of important variables and they are therefore meant to complement, rather than supersede, a clinician's judgment and/or validated severity scores.
In conclusion, MR-proADM appears to be particularly effective, among other biomarkers, in the risk stratification for patients affected by viral sepsis (15), the new syndrome characterizing patients affected by SARS-CoV-2.
MR-proADM can contribute with other biomarkers to predict the mortality of critical COVID-19 patients affected by ARDS as soon as they are admitted to the emergency department.
Annex:The price of MR-proADM is around 15 Euros/test. The Kryptor instrument by ThermoFisher is on loan for use.
We declare no competing interests.
All the authors contributed to study conception and design, and analysis and interpretation of the data.
Not applicable
We thank Loreta D’Amico for her valuable technical assistance and all patients and their families involved in the study.
The study was approved by the Local Ethics Committee(approval number 87/20) and was performed in accordance with the Dec- laration of Helsinki.
Not applicable

![]()

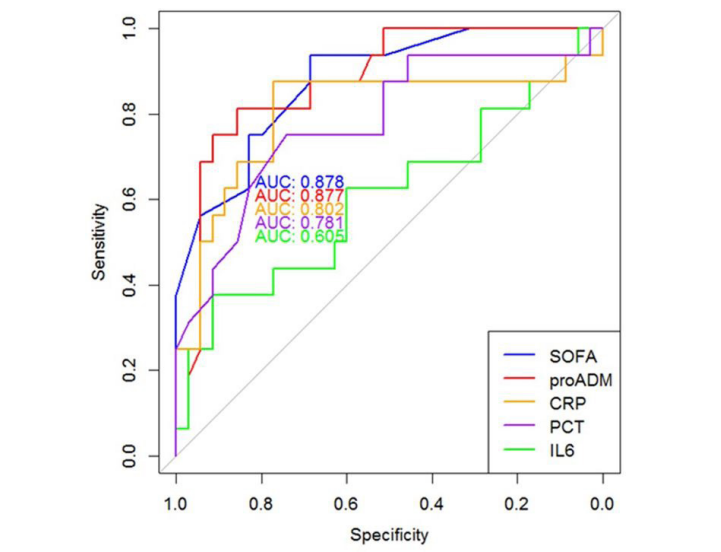 |
| Figure 1: Association of SOFA clinical score and candidate biomarkers with mortality: AUROC area under the receiver operating characteristic curve |
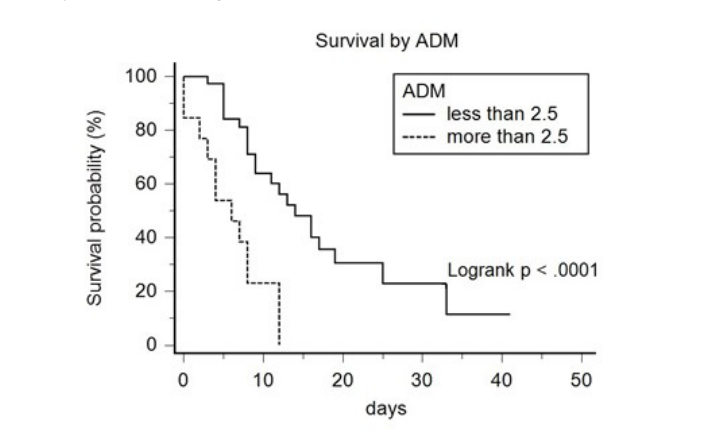 |
| Figure 2: Kaplan-Meier survival curve. Stratification of patients with mid-regional proadrenomedullin (MR-proADM) levels greater or less than 2,5nmol/L at ICU admission |
|
COVID-19 pneumonia |
|
N° (%) |
Age |
|
Total (median) |
69 yrs |
< 40 yrs |
1 (1.9) |
1-65 rs |
19 (37.3) |
66-80yrs |
25 (49) |
>80 yrs |
6 (11.8) |
Sex |
|
Male |
36 (70.5) |
Female |
15 (29.5) |
SOFA score (median) |
8 |
Comorbidities |
|
Any |
29 |
Hypertension |
17 |
Diabetes |
7 |
COPD |
1 |
Cancer |
4 |
Ischemic Heart Diseases |
8 |
Liver Diseases |
1 |
Obesity |
4 |
Mortality |
35/51 (68.6) |
Treatment in Hospital |
|
IMV |
36 (70.5) |
NIMV |
8 (15.7) |
Oxygen therapy |
2 (4) |
ICU LOS, days, median (range) |
8 (3-33) |
Days of Mortality,median (range) |
8 (3-33) |
|
Death in the |
Death after th |
Test for difference |
Age |
|
|
P=0.24 * |
< 40 yrs |
1 |
0 |
|
40-65 yrs |
0 |
9 |
|
66-80 yrs |
11 |
8 |
|
>80 yrs |
3 |
3 |
|
Comorbidities |
|
|
|
Any |
|
|
P=0.56 ** |
Hypertension |
3 |
14 |
|
Diabetes |
1 |
6 |
|
COPD |
0 |
1 |
|
Cancer |
1 |
1 |
|
IschemicHeart Diseases |
2 |
5 |
|
LiverDiseases |
0 |
1 |
|
Obesity |
0 |
1 |
|
≥2 comorbidities |
2 |
6 |
|
|
Survived |
Died |
OR (95% CI) |
P value |
AUC (P value) |
MR-proADM |
|
|
|
|
|
>2.5 |
0 |
13 |
* |
0.0006 |
0.88 (0.0001) |
<2.5 |
16 |
22 |
1 |
|
|
CRP |
|
|
|
|
|
>95 |
2 |
26 |
20.2 (4.5-146.2) |
0.0001 |
0.80 (0.0001) |
<95 |
9 |
14 |
1 |
|
|
PCT |
|
|
|
|
|
>2 |
1 |
8 |
4.4 (0.71 - 86.6) |
0.1196 |
0.78 (0.003 ) |
<2 |
15 |
27 |
1 |
|
|
IL-6 |
|
|
|
|
|
>20 |
10 |
32 |
6.4 (1.42 - 35.0) |
0.001 |
0.60 (0.575) |
<20 |
6 |
3 |
1 |
|
|
SOFA |
|
|
|
|
|
>8 |
1 |
24 |
32.7 (5.6 - 630.4) |
0.0001 |
0.88 (0.0001) |
<8 |
15 |
11 |
1 |
|
|
|
Overall mortality |
One-week mortality |
||
|
OR (95% CI) |
P value |
OR (95% CI) |
P value |
MR-proADM |
|
|
|
|
>2.5 |
* |
0.814 |
7.39 (1.4 – 48.4) |
0.027 |
<2.5 |
1 |
|
1 |
|
CRP |
|
|
|
|
>95 |
44.6 (3.8 –1715.5) |
0.009 |
1.48 (0.3 – 7.4) |
0.615 |
<95 |
1 |
|
1 |
|
PCT |
|
|
|
|
>2 |
0.7 (0.004– 169.7) |
0.891 |
0.3 (0.04 – 2.16) |
0.274 |
<2 |
1 |
|
1 |
|
IL-6 |
|
|
|
|
>20 |
2.09 (0.05– 104.6) |
0.682 |
2.7 (0.29– 62.9) |
0.427 |
<20 |
1 |
|
1 |
|
SOFA |
|
|
|
|
>8 |
95.3 (3.5 – 52045.9) |
0.04 |
0.68 (0.11 – 3.8) |
0.667 |
<8 |
1 |
|
1 |
|




































