Open Access
Research Article
Max Screen
ISSN: 2639-9253
Copyright: © 2021 Nielsen DL. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
The aim of this study is to describe clinical variables and comorbidities in patients with shock, at arrival to the emergency department, and evaluate the diagnostic validity for different shock etiologies.
This was a retrospective cohort study with tertiary analysis of data previously published in two other studies. The study population was all patients with shock, arriving to the emergency department at Odense University Hospital between 2000 and 2011. Shock was defined as systolic blood pressure ≤100mmHg and one or more organ failures. Patients were grouped according to discharge diagnoses and this method was manually validated through patient records. The diagnostic value of 26 clinical variables and 10 comorbidities were described and tested.
We included 1553 patients and found statistical significant differences in 17 clinical variables. The diagnostic validity of the variables was very low except for CRP, temperature and hemoglobin which had moderate diagnostic value. We also found significant differences in prevalence of comorbidities (liver disease, cardiovascular disease, and chronic obstructive pulmonary disease) between patients with septic, cardiogenic, and hemorrhagic shock.
We conclude that patients who arrived at the emergency department with septic, cardiogenic or hemorrhagic shock differed in some aspects, but even the strongest predictors could not discriminate completely between etiologies.
Keywords: Sepsis; Shock; Etiology; Comorbidity
List of abbreviations:ED: Emergency Department; SBP: Systolic Blood Pressure; CI: Confidence Interval; ICD: International Classification of Diseases; COPD: Chronic Obstructive Pulmonary Disease; IQR: Interquartile Range; ROC: Receiver Operating Characteristics; AUROC: Area under the Receiver Operating Characteristics Curve; PPV: Positive Predictive Value; NPV: Negative Predictive Value; LR+: Positive Likelihood Ratio; LR-: Negative Likelihood Ratio; CRP: C-Reactive Protein; ALAT: Alanine Transaminase; INR: International Normalized Ratio; S: Serum; P: Plasma; B: Blood
Shock is a common condition in the emergency department (ED) and has different etiologies. While the clinical presentation is circulatory collapse, the etiology is not always evident when the patient arrives to the ED [1,2]. The etiology may be obvious, e.g. major bleeding from a trauma. However, cardiogenic shock or distributive shock can be much less obvious, because the clinical picture is often obscured by altered mental status and comorbidities [2,3].
Most research currently available [3-7], regarding the diagnostics and identification of shock etiologies, focus on a single etiology. They are conducted in populations from intensive care or in populations identified in-hospital after the ED evaluation, and rarely in unselected patients [3-7].
Seen from an ED perspective these studies provide limited information. A key step is early identification of the etiology, so that it can be rapidly corrected (e.g. control of bleeding or administration of antibiotics) since targeted treatment improves prognosis [2-8].
Knowledge of the diagnostic validity of common clinical variables, which are available shortly after patient arrival, will allow the ED clinician to interpret the test results at an evidence-based basis and might prevent misinterpretation regarding their usefulness.
The aim of this study was to describe clinical characteristics of ED patients presenting with septic, cardiogenic or hemorrhagic shock, and evaluate the diagnostic validity for identification of these etiologies among unselected patients, who arrived to the ED with hypotension and one or more organ failures.
We conducted a retrospective cohort study of all patients with shock, who arrived at the ED at Odense University Hospital between 2000 and 2011 other aspects of the cohort have previously been described [1,9,10]. We identified clinical variables and comorbidities related to septic, cardiogenic and hemorrhagic shock, and evaluated their diagnostic validity among all adult patients, who arrived to ED with hypotension and one or more organ failures. Odense University Hospital is a 1,000-bed university teaching hospital. It serves both as a tertiary and primary hospital and has all specialties present. It is the only ED in this part of Denmark and provides 24-hour acute medical care. As primary hospital the ED serves a mixed rural-urban population of approximately 290,000 people and had 37.000 annual visits during the study period.
Eligible patients were aged ≥18 years presenting at the ED with a systolic blood pressure (SBP) ≤100mmHg and one or more organ failures [11-13]. SBP must have been measured within 3 hours upon arrival. Since laboratory analysis of biochemical variables could exceed 3 hours during busy hours, the variables defining organ failures were based on variables measured up to 24 hours upon arrival. SBP was extracted by electronic screening of free text in patient records [14]. This has previously been manually validated and has a sensitivity of 95% (95% Confidence interval (CI) 91.2-98.5) and a specificity of 100% (95% CI 99.0-100) for retrieving correct SBP [11]. The included organ failures were cardiovascular, renal, coagulation, and hepatic (Table 1).
Patients with prehospital evident acute myocardial infarction went directly to cardiological intervention, and were not included in the ED cohort. We excluded patients who were residing outside the hospital’s catchment area and patients without a valid Danish personal identification number, since this was needed to link data between the different sources. Patients who visited the ED between 1 of January 1998 and 1 of January 2000 with hypotension were also excluded. If a patient had multiple ED contacts with hypotension through the study period, only the initial contact was included. This was done to avoid that a single patient with multiple contacts could have a large impact on the laboratory data or the prevalence of shock etiologies.
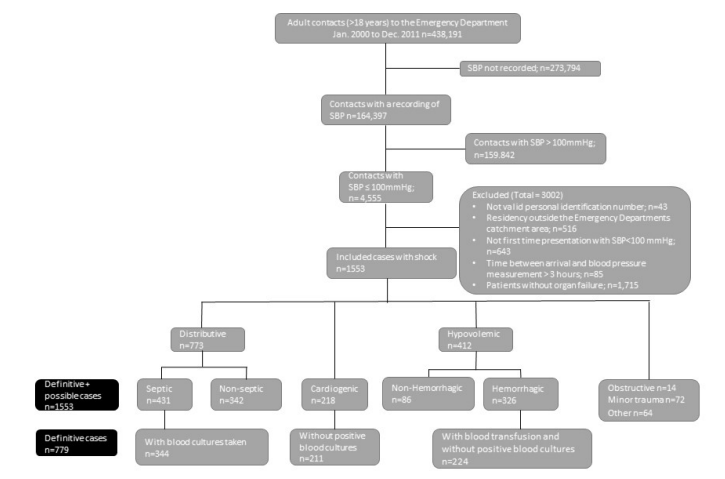
In the unselected cohort of patients, who arrived in the ED with hypotension and one or more organ failures, we identified the etiology based on their primary hospital discharge diagnosis (International Classification of Diseases (ICD) 10). We grouped the etiologies into either distributive (septic or non-septic), cardiogenic, hypovolemic (hemorrhagic or non-hemorrhagic), obstructive or other shock etiology (Figure 1).
Discharge diagnoses indicating an infectious pathophysiology were grouped as septic (e.g acute cystitis and pneumonia), while other causes of inflammation and vasodilation were grouped as non-septic distributive shock (e.g. poisoning). Cardiovascular diagnoses (e.g. heart failure and supraventricular tachycardia) were grouped as cardiogenic. Diagnoses suggesting hemorrhage (e.g. ruptured abdominal aortic aneurism and duodenal ulcer with hemorrhage) were grouped as hemorrhagic, and hypovolemic without bleeding were grouped as non-hemorrhagic (e.g. dehydration). The obstructive shock etiology included conditions causing increased afterload (e.g. pulmonary embolisms). Patients with discharge diagnoses not meeting any of the criteria were revised through patient records, and if they were not found suitable for an etiology they were grouped as other. All discharge diagnoses and their relation to etiologies has previously been published [9]. Based on a sufficient number of patients and a relatively homogenic patient population within the etiology groups, we were able to evaluate clinical characteristics and the diagnostic value of these, among patients with septic, cardiogenic or hemorrhagic etiologies.
In the identification of clinical characteristics of the patients, we aimed to ensure that only patients who were most likely to have a septic, cardiogenic or hemorrhagic etiology were included. To ensure this, additional criteria were used to define definitive cases. For the septic etiology, the patients must have had blood cultures obtained within 24 hours after arrival. For the hemorrhagic etiology, patients must have received a blood transfusion of ≥0.5L within 24hours after arrival. All patients with positive blood cultures obtained < 48 hours after arrival, who were initially treated as cardiogenic or hemorrhagic etiology, were moved to the septic etiology, suspecting an underlying infection.
The definitive cases definition was validated by chart review with a random sample of 100 cases from each etiology which were pooled together. The 300 patient records were then read and assigned to an etiology in a blinded manner. The validation of the definitive cases found an agreement in 93% (95% CI 86-97), 92% (95% CI 84-96) and 97% (95% CI 91-99) for septic, cardiogenic and hemorrhagic etiology respectively. The patients not meeting the criteria for the definitive cases were manually validated through patient records. Patients receiving ≥0.5L blood who were not in the hemorrhagic etiology were also manually validated.
Any patient who was in an incorrect group was relocated. Through chart reviews, we found some patients primarily categorized as hemorrhagic etiology, who only had a minor trauma and were unlikely to have hemorrhagic shock. We created a minor trauma category for these patients having minor and/or distal fractures and contusions. Femur, humerus and pelvic fractures were still defined as hemorrhagic etiology. All chart reviews were done by author DLN.
We included a total of 26 variables. All variables with data available for approximately 50% of patients in the cohort were included. For all variables the first measured value was used, and only measurements done < 24 hours after arrival were included. Heart rate and temperature were extracted by electronic free text search in the same patient record note as where the SBP were found. All other variables were extracted from the electronic patient file.
Comorbidities included were previous diagnosis of alcohol abuse, cardiovascular disease, immunosuppression, liver disease, neurological disease, renal disease, cancer, diabetes, gastrointestinal disease and chronic obstructive pulmonary disease (COPD). We used hospital discharge diagnoses and redeemed prescriptions from a period of 3650 – 7 days prior to the contact date [15]. The definitions are presented in Table 2. For recent surgery, we used a period of 180 – 1 day prior to contact date, and for surgical implants we used all time up to 1 day prior to contact date.
Continuous and categorical variables were described as medians (interquartile range (IQR)) and percentages (95% CI) respectively.
With the aim to identify clinical characteristics we compared all laboratory variables between the definitive cases using a k-sample equality-of-median test (Data non-normally distributed); patients with missing values were handled as such and were not included in the analysis of the particular variable. Variables which showed a difference in p-values < 0.05 were considered significant.
The diagnostic value of the identified statistically significant clinical characteristics was evaluated in the entire cohort of patients who arrived to the ED with hypotension and one or more organ failures. In this analysis the septic, cardiogenic and hemorrhagic etiologies were based on their ICD10 hospital discharge diagnoses only.
Evaluation of diagnostic validity was based at receiver operating characteristic (ROC) curves. The identified clinical characteristic was interpreted as having some diagnostic value if the area under the ROC curve (AUROC) was > 0.65. Clinical characteristics identified with some diagnostic value were evaluated further.
Cut-off values for these analysis were based on proposed cut-off values in previous studies, and our cut-off values with the highest accuracy (highest sum of true positive and true negative determined according to the ROC curve analysis). Aspects of their diagnostic value were calculated sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (LR+) and negative likelihood ratio (LR-) [4-6,16]. For each of the comorbidities, the proportion of patients were calculated and presented as percentage.
Statistical analyses were done using Stata 14.0 (Stata Corp LP, College Station, Texas)
In Denmark all people are assigned an unique personal registration number at birth, and all prehospital and hospital health care services are tax-funded and provided free of charge to all citizens [17]. The Danish personal registration number was used to link information from the Danish Civil Registration Register (Age, sex and demographics), the Danish National Patient Register (Discharge diagnoses), and local biochemical, microbiological, and blood transfusion data [15,17]. Data regarding previously redeemed prescriptions were extracted from the Odense Pharmaco-epidemiological Database (comorbidity) [18].
Of 438,191 adult ED contacts, 1553 met the criteria for shock and were included in the study (Figure 1). The most common etiology was septic (28%) followed by non-Septic (22%), hemorrhagic (21%), cardiogenic (14%), non-hemorrhagic (6%), minor trauma (5%), obstructive (1%), and 4% were grouped as other. We were not able to perform an analysis of patients in the non-septic distributive, non-hemorrhagic or minor trauma etiology due to a large variety of underlying diseases, resulting in heterogenic groups. The obstructive etiology was excluded do to the few number of patients.
In the 779 cases with definitive septic, cardiogenic or hemorrhagic etiology we analyzed 26 clinical variables, of which 17 showed a significant difference on a 95% confidence level. The results are presented in Table 3.
Two comorbidities were significantly more prevalent in one etiology compared to the two others. This was cardiovascular disease for the cardiogenic etiology, and liver disease for the hemorrhagic etiology. Neurological comorbidity was significantly less prevalent in the hemorrhagic etiology (Figure 2).
Following identification of 17 variables which differed significantly between the patients with definitive septic, cardiogenic or hemorrhagic etiology, we evaluated the diagnostic validity in the complete shock cohort (1553 patients). Based on ROC curves we found that 5 variables showed an AUROC > 0.65. For septic shock this was C-reactive protein (CRP), lymphocytes, and temperature with an AUROC of 0.83 (95% CI 0.81-0.85), 0.70 (95% CI 0.67-0.73), and 0.68 (95% CI 0.65-0.71) respectively. For hemorrhagic shock it was hemoglobin and troponin-t with an AUROC of 0.79 (95% CI 0.76-0.81) and 0.65 (95% CI 0.60-0.70) respectively. No variable showed and AUROC > 0.65 for the cardiogenic etiology.
ROC curves for CRP, temperature, and lymphocytes for the septic etiology, and hemoglobin and troponin-t for the hemorrhagic etiology, are presented in Figures 3 and 4 respectively. The ROC curves are based on calculations from all cases (definitive and possible). We found that the cut-off values with the highest accuracy were 92mg/L for CRP (78% correctly classified (True positives and true negatives)), 38° for TP (75% correctly classified), 0.2×109/L for lymphocytes (67% correctly classified), 7.7 g/dl for hemoglobin (82% correctly classified), and 0.01μg/L for troponin-t (87% correctly classified).
Table 4 summarizes for each etiology sensitivity, specificity, predictive values, and likelihood ratios at different thresholds for CRP, temperature, hemoglobin and for the 3 comorbidities which showed a significant difference in prevalence.
Using the highest accuracy cut-off value for CRP resulted in a sensitivity of 65.5% (95% CI 60.7-70.1) and a specificity of 84.9% (95% CI 82.3-87.3) When combining CRP>100mg/L and TP>38° it results in a sensitivity of 70.2% (95% CI 65.5-74.5) and a specificity of 83.7% (95 CI 81.0-86.1) for diagnosing septic etiology, compared to a sensitivity of 62.6% (95% CI 57.8-67.3) and a specificity of 85.9% (95% CI 83.3-88.2) of CRP>100mg/L alone. The highest accuracy cut-off value for hemoglobin resulted in a sensitivity of 34.3% (95% CI 29.0-40.0) and specificity of 95.7% (95% CI 94.3-96.9).
In this tertiary analysis we found that among patients who arrived in the ED with hypotension and one or more organ failures, most laboratory tests did not provide information for discrimination between septic, cardiogenic or hemorrhagic shock etiology; CRP, temperature, lymphocytes, troponin-t and hemoglobin provide a moderate diagnostic validity. Furthermore we found that the septic etiology was the most common shock etiology which correlates with other studies [2,3,9,19].
We tested several clinical characteristics and found that none of these alone had enough diagnostic value to completely discriminate between shock etiologies. Our results illustrate the difficulty of diagnosing patients with circulatory collapse in the ED, and the importance of not focusing on a single test. We found that predictors like CRP, temperature and hemoglobin leave diagnostic uncertainty. This illustrate the challenge of discrimination between shock etiologies in the ED, in the absence of obvious indicators such as e.g. traumatic bleeding.
As in previous studies we found that a high CRP and high temperature was related to septic etiology [4,5,20]. Simultaneously we also found that about one out of eight patients discharged by a sepsis related diagnosis had a low CRP at arrival to the ED, as well as about one third of the patients with elevated CRP were discharged by a non-sepsis diagnosis. The results are in accordance with other studies and illustrate that the false positive and false negative test results are important for the clinician to be aware of [3- 5,21].
For the hemorrhagic etiology we found that hemoglobin had poor diagnostic value in identifying patients with hemorrhagic shock, with a considerably amount of false negative test results. This could be explained by the delay in hemoglobin drop after trauma, however the diagnostic value of hemoglobin in acute bleeding remains controversial [22].
For the cardiogenic etiology no laboratory test showed an AUROC >0.65, and only cardiovascular comorbidity differed from the other etiologies. Known comorbidity has been shown useful in diagnostics, but only in combination with other clinical parameters [7]. We also found that liver disease was more prevalent in the hemorrhagic etiology. Both liver disease and cardiogenic comorbidity had a low PPV of 36% and 24% respectively.
Some of the tested variables showed a statistically significant association to a specific etiology but did not provide any diagnostic value. This illustrate the general need for evaluation of the usefulness of a clinical variable.
We were able to obtain and compare a large sample size of unselected ED patients, removing the confounding factor of patients surviving to the ICU, where most other studies have their focus. The unique Danish personal registration number made it possible to follow all patients in the population-based registries, accurately link information between healthcare registries and ensured complete follow up. We have previously found that discharge diagnosis have reasonable value in identifying patients with infection [23].
The data used for this study was not collected for research purposes, and not all patients had measurements of all variables. The available data were limited to the variables that the clinician found relevant for each patient. The missing values were thus not considered relevant for the individual patient by the treating clinician, and may well be in the normal range. This is however uncertain and the missing values must be considered as a limitation in this study. We used all organ failures possible by data availability. We were not able to include arterial punctures, lactate, respiratory frequencies and Glasgow Coma Scale values since they were not systematically collected. This means metabolic failure and organ failures related to the respiratory system and failure of the central nervous system could not be included in the study. We used previous discharge diagnoses to define comorbidity and calculate the Charlson Comorbidity Index, which means only comorbidities requiring hospitalization were included. This might result in comorbidities such as diabetes and hypertension being under reported in this study.The data used for this study was not collected for research purposes, and not all patients had measurements of all variables. The available data were limited to the variables that the clinician found relevant for each patient. The missing values were thus not considered relevant for the individual patient by the treating clinician, and may well be in the normal range. This is however uncertain and the missing values must be considered as a limitation in this study. We used all organ failures possible by data availability. We were not able to include arterial punctures, lactate, respiratory frequencies and Glasgow Coma Scale values since they were not systematically collected. This means metabolic failure and organ failures related to the respiratory system and failure of the central nervous system could not be included in the study. We used previous discharge diagnoses to define comorbidity and calculate the Charlson Comorbidity Index, which means only comorbidities requiring hospitalization were included. This might result in comorbidities such as diabetes and hypertension being under reported in this study.
Patients with prehospital evident acute myocardial infarction were not included in the study. This affects the prevalence of cardiogenic shock in our study and possibly the diagnostic value of troponin-t. Troponin-t did not differ between the cardiogenic and septic etiology. This could be explained by severe sepsis and septic shock commonly being complicated by myocardial dysfunction [24]. We were not able to include electrocardiography and echocardiography which is a limitation.
Patients in the non-septic distributive and non-hemorrhagic etiologies had a large variety of underlying diseases, resulting in heterogenic groups, therefore it was not meaningful to make a description of their clinical characteristics as a group. The minor trauma patients were generally mistakenly included do to shock index ≥ 1. To avoid including the patients in the hemorrhagic etiology we categorized them as a minor trauma by manually reviewing the medical journals. By moving these patients, it does not influence our data in the hemorrhagic etiology.
This was a single-center study and the results may not necessarily be generalized to other hospitals in Denmark or other countries. This ED is the only one serving this part of Denmark, and patients living outside our catchment area were excluded (n=516.) This was done to minimize bias from receiving critically ill patients from other hospitals. Our biggest exclusion of patients was no measurement of SBP upon arrival (n=273,774). This was due to triaging nurses’ clinical judgement that these patients suffered minor complaints, and therefore did not need SBP measurements.
We conclude that among patients who arrived to ED with hypotension and organ failure, most laboratory tests do not provide information for identification of septic, cardiogenic or hemorrhagic etiology. CRP, temperature, lymphocytes, troponin-t and he- moglobin provide a moderate diagnostic validity. This study underlines that diagnostic workup for shock is complex and that no single test provides sufficient diagnostic validity to discriminate between etiologies.
The study was approved by the Danish Data Protection Agency (J.nr 2008-58-0035) and the Danish Health and Medicines Authority (j.nr. 3-3013-205/1). In accordance with Danish law, observational studies performed in Denmark do not need approval from the Medical Ethics Committee.
The datasets generated and analyzed during the current study are not publicly available due to laws from the Danish Data Protec- tion Agency. The data are available from the corresponding author on reasonable request.
We would like to thank Niels Ibsgaard Agerbek for professional help with data extraction.
DLN conceived the study, analyzed and interpreted the data, and drafted the manuscript. JGH contributed to the study design, an- alyzed and interpreted the data. ATL conceived and coordinated the study as well as performed critical appraisal of the manuscript. DPH, LMR, TGJ and KT contributed with data collection and interpretation of the data. All authors critically reviewed drafts of the manuscript and approved the final paper.
DLN is supported by an unrestricted grant from the private foundation Fonden af 17-12-1981. ATL is supported by an unrestricted grant provided from the philanthropic foundation TrygFonden. None of the authors have financial interests in the project.

![]()

 |
| Figure 1: Flowchart of included patients and their etiology |
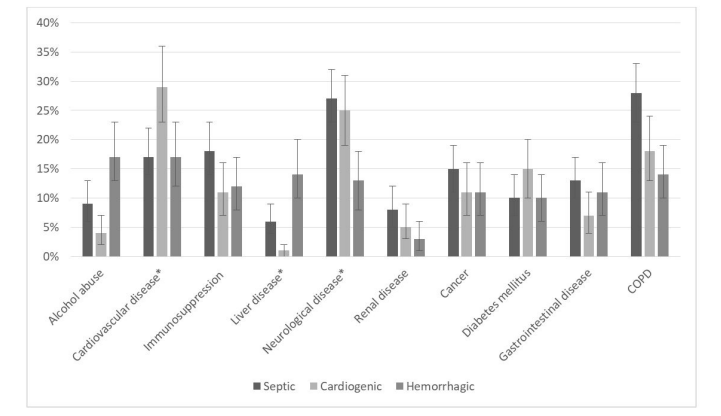 |
| Figure 2: Proportion of patients with a definitive septic, cardiogenic or hemorrhagic shock, suffering from different comorbidities |
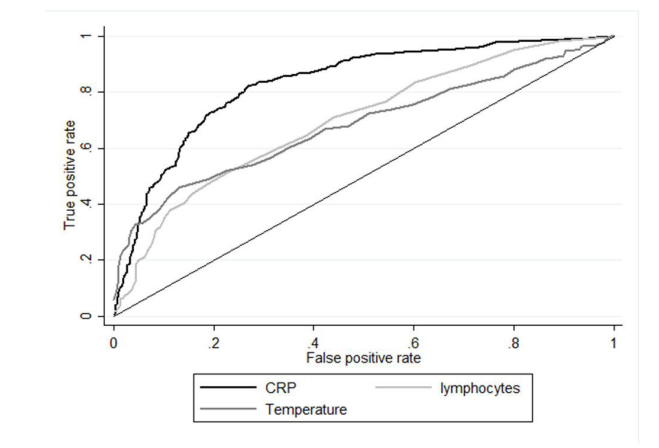 |
| Figure 3: Receiver operating characteristic curve of C-reactive protein, temperature and lymphocytes to identify patients with septic shock etiology |
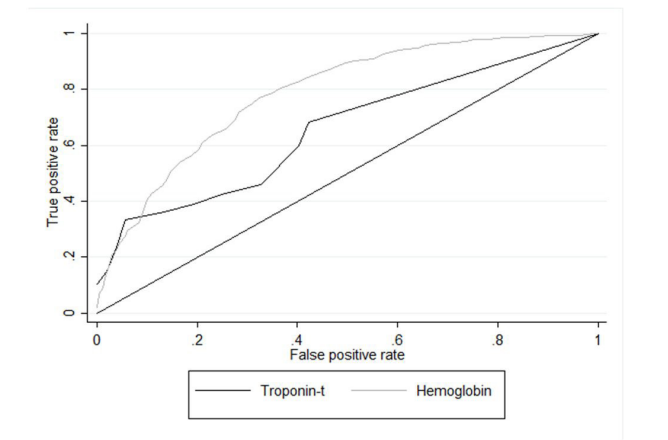 |
| Figure 4: Receiver operating characteristic curve of troponin-t and hemoglobin to identify patients with hemorrhagic shock etiology |
Variable |
Definition |
Time period |
Hypotension [11-13] |
SBP ≤ 100mmHg |
Registered ≤ 3 hours after arrival |
Cardiovascular [15] |
Shock index* ≥ 1 |
Registered ≤ 3 hours after arrival |
Renal [16] |
S-creatinine > 177 µmol/L and > 100 µmol/L increase from earlier S-creatinine |
180 days before and 1 day after the index date |
Coagulation [16] |
Platelet count <101x109/L and earlier platelet count > 159x109/L or never previously registered OR |
180 days before and 1 day after the index date |
Hepatic [9] |
S-bilirubin >42 µmol/L and earlier S-bilirubin |
180 days before and 1 day after |
Variable |
Source |
Definition (In the period 3650 – 7 days prior to admission) |
Alcohol |
OPED |
A redeemed prescription of disulfiram from 2007 and onwards. |
|
LPR |
≥ 2 admissions with a discharge diagnosis of an acute alcohol episode |
Cancer |
LPR |
Any cancer diagnosis |
Cardiovascular |
LPR |
Myocardial infarction, congestive heart failure, peripheral vascular disease. |
Diabetes |
LPR |
Diabetes mellitus with- or without chronic complications |
Gastrointestinal |
LPR |
Gastrointestinal disease, Ulcer disease |
Immunosuppression |
OPED |
Glucocorticoids, cumulative defined as daily dose >= 120mg in the preceding 120 days |
|
LPR |
Primary immunodeficiency diseases, acquired immune deficiency, syndrome defining |
COPD |
LPR |
Chronic pulmonary disease |
Liver disease |
LPR |
Mild liver disease, moderate/severe liver disease |
Neurological |
LPR |
Cerebrovascular disease, dementia, hemiplegia |
Renal |
LPR |
Moderate/severe renal disease |
Variable (N with missing data) |
Septic |
Cardiogenic |
Hemorrhagic |
P-value |
Male (0) |
55% |
53% |
63% |
0.359 |
Age [years] (0) |
74 (64-83) |
76 (65-83) |
68 (57-79) |
<0.001 |
Heart rate [bpm] (24) |
103 (88-118) |
104 (88-130) |
100 (84-112) |
0.050 |
Systolic blood pressure [mmHg] (0) |
88 (79-94) |
89 (78-93) |
86 (79-93) |
0.053 |
Diastolic blood pressure [mmHg] (0) |
50 (42-59) |
52 (43-63) |
50 (44-59) |
0.061 |
Temperature [ºC] (197) |
37.4 (36.2-38.4) |
36.6 (36.0-37.1) |
36.1 (35.5-36.8) |
<0.001 |
Charlson Comorbidity index (0) |
2 (1-3) |
2 (0-3) |
1 (0-3) |
0.001 |
P-Sodium [mmol/L] (51) |
137 (133-141) |
138 (133-141) |
137 (133-140) |
0.329 |
P-Potassium [mmol/L] (59) |
4 (2.5-4.6) |
4.1 (3.7-4.7) |
4.1 (3.7-4.7) |
0.090 |
P-C-reactive protein [mg/L] (86) |
137.5 (69.9-235.5) |
18.5 (8-73) |
13 (6-40) |
<0.001 |
B-Hemoglobin [g/dL] (59) |
11.76 (10.07-13.37) |
12.49 (10.8-13.86) |
8.06 (6.61-10.15) |
<0.001 |
P-Creatinine [µmol/L] (31) |
154 (104-242) |
131.5 (103-188) |
108 (85-148) |
<0.001 |
P-Bilirubin [µmol/L] (216) |
11 (7-20) |
11 (7-21) |
7 (4-17) |
<0.001 |
P-Albumin [g/L] (90) |
31 (26-36) |
35 (31-39) |
29 (24-34) |
<0.001 |
P-ALAT [U/L] (190) |
25 (15-57) |
25 (17-53) |
17 (12-37) |
0.001 |
P-Carbamide [mmol/L] (54) |
12.9 (8.5-19.9) |
10.5 (7-18) |
10.8 (6.9-17) |
0.004 |
P-Troponin-T [μg/L] (498) |
0.06 (0.02-0.15) |
0.04 (0.01-0.18) |
0.01 (0.01-0.05) |
0.003 |
B-Platelets [×109/L] (97) |
221 (149-323) |
242 (184-307) |
212 (142-277) |
0.146 |
INR (306) |
1.2 (1.1-1.5) |
1.1 (1.0-1.3) |
1.3 (1.1-1.7) |
<0.001 |
P-Coagulation factors (201) |
0.67 (0.5-0.89) |
0.75 (0.57-1.02) |
0.6 (0.39-0.78) |
0.010 |
B-Leucocytes [×109/L] (51) |
14.3 (9.4-19.3) |
11.2 (8.4-14.5) |
11.65 (8.7-15.3) |
<0.001 |
B-Neutrophils [×109/L] (220) |
8.6 (7.9-9.2) |
7.8 (6.8-8.7) |
8.2 (7.5-8.8) |
<0.001 |
B-Lymphocytes [×109/L] (233) |
0.6 (0.3-1.0) |
1.2 (0.7-2.0) |
1.1 (0.7-1.8) |
<0.001 |
B-Eosinophils [×109/L] (320) |
0 (0-0) |
0.01 (0-0.02) |
0 (0-0.1) |
0.002 |
B-Basophils (322) |
0 (0-0) |
0 (0-0) |
0 (0-0) |
0.213 |
B-Monocytes (237) |
0.04 (0.02-0.07) |
0.065 (0.04-0.08) |
0.05 (0-03-0.07 |
0.001 |
Variable |
Sensitivity |
Specificity |
PPV |
NPV |
+LR |
-LR |
For septic etiology |
|
|
|
|
|
|
C-reactive protein >50 mmol/L |
80.1% |
74.2% |
60.9% |
88.1% |
3.1 (2.7-3.5) |
0.27 |
C-reactive protein >80 mmol/L |
68.9% |
82.5% |
66.4% |
84.1% |
3.9 (3.3-4.6) |
0.38 |
C-reactive protein >100 mmol/L |
6 2 . 6 % |
8 5 . 9 % |
6 9 . 0 % |
8 2 . 1 % |
4.4 (3.7-5.3) |
0.44 |
Temperature >38°C |
30.7% |
96.4% |
80.4% |
74.4% |
8.6 (5.8-12.9) |
0.72 |
Lymphocytes ≤0,2x109/L |
93.2% |
23.7% |
40.0% |
86.5% |
1.2 (1.2-1.3) |
0.29 |
For cardiogenic etiology |
|
|
|
|
|
|
Cardiogenic comorbidity |
29.4% |
84.5% |
23.6% |
88.0% |
1.9 (1.5-2.4) |
0.84 |
For hemorrhagic etiology |
|
|
|
|
|
|
Hemoglobin <6.45 g/dL |
18.0% |
98.8% |
81.8% |
80.1% |
15.0 |
0.83 |
Hemoglobin <8.06 g/dL |
38.3% |
94.4% |
67.3% |
83.7% |
6.9 (5.1-9.2) |
0.65 |
Hemoglobin <9.67 g/dL |
58.0% |
84.3% |
52.4% |
87.2% |
3.7 (3.1-4.4) |
0.50 |
Troponin-t ≤ 0.01μg/L |
57.7% |
68.2% |
21.0% |
91.7% |
1.8 (1.4-2.4) |
0.62 |
Liver disease |
12.3% |
94.2% |
36.0% |
80.2% |
2.1 (1.5-3.1) |
0.93 |
No neurological comorbidity |
84.7% |
23.2% |
22.7% |
85.3% |
1.1 (1.1-1.2) |
0.65 |




































