Open Access
Research Article
Max Screen
ISSN: 2639-9253
Copyright: © 2020 Barnett R. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
This research investigated the physiological and psychological impact of supine and side lying physical restraint (PR) positions which have been suggested as safer alternatives to prone restraint positions. Twenty adults participated. From baseline Forced Vital Capacity (FVC) reduced by 10.4%, 10.4% and 14.6%, and FEV1 reduced by 7%, 7%, and 12% for supine arms low (SPR-AL), supine arms high (SPR-AH), and Side Lying restraint (SLR) respectively. SLR imposed the greatest Thoracic Weight bearing Pressure (TWP) at 116.1 (±17.5) mmHg, which was ~17% more than SPR-AH, and ~23% more than SPR-AL. HR was unaffected. Comfort was perceived to be greatest for SPR-AL, with SPR-AH being 6.7% less comfortable and SLR being 45% less comfortable. Anxiety was greatest in SLR, with SPR-HL and SPR-AL being 36.5% and 48.1% less anxiety inducing respectively. Breathing limitation was greatest in SLR, with SPR-AH and SPR-AL being 44.4% and 46.3% less limiting respectively. Compared to baseline all three restraint positions reduced respiratory measures (p = 0.001), with SPR-AL and SPR-AH being similar but differing from SLR (p = 0.001), and resulted in perceptions of discomfort, anxiety, and breathing limitation, with SLR being the most negatively impactful position tested. These findings are in keeping with our previous research which showed variance in the physiological and psychological impact of different restraint positions. All restraint positions possess the ability to negatively impact an individual both physiologically and psychologically but that impact is not homogenous, with some positions clearly possessing a lower level of risk than others.
Keywords: Physical Restraint; Supine; Side Lying; Physiology; Psychology
This research will be of interest to those who work in, commission or regulate settings where staff are trained to use restrictive physical interventions (manual restraint). Physical Restraint (PR) is a manual, hands-on method of containing or immobilising individuals by limiting their freedom to move to prevent or reduce their ability to harm themselves or others [1,2]. PR remains contentious, not only because of the potential breaches in human rights if misused or abused, but also due to its ability to cause anatomical, physiological and psychological harm including death [3].
The Human Rights Act 1998 [4] created legal obligations for the protection of rights and applies to all public authorities, determining the legal duties of staff to respect and protect everyone’s human rights. As such the use of restraint must be lawful and rightsrespecting. Article 2 requires ‘all reasonable steps to be taken to protect a person's right to life’ and therefore can include intervening with PR to protect a person from harming themselves or others; as well as stopping the use of PR if it is likely to result in harm. Article 3 prohibits ‘torture, and inhuman and degrading treatment or punishment’ which may include different types of assault on human dignity and physical integrity, including acts of unjustified suffering and acts which inflict sufficient severity of pain especially if undertaken deliberately. Therefore, the use of any PR must not cause unnecessary or intended harm (including negligent acts or failures to protect) which amounts to degrading or ill-treatment. When deciding if any intervention is a breach of Article 3, consideration should be given to the severity and intensity of suffering inflicted to an individual based on an assessment of factors including duration, physical and psychological effects, sex, age, gender and health of the person, as well as the manner and execution of the intervention. Furthermore, Article 8 protects a person’s right to be consulted and involved in decision making. With respect to the use of PR, staff should ensure that the use of any restrictive practice is transparent and part of a recovery-based, person-centred plan which fully involves the individual.
Our previous research [5,6] quantified the pressures imposed on the anterior chest wall, the concomitant reduction in ventilatory capacity and the psychological impact of prone restraint. Although research is lacking into the physiological and psychological impact of alternatives to the prone restraint position recent standards to improve training to eliminate or minimise use of PR and make practice safer have recently become law [7,8]. This recent change in legislation follows on-going social, professional and political campaigns in which seated, supine and side lying restraint has been advocated as “safer” alternatives, with a common perception that restraint-related adverse events arise solely from the use of the prone restraint position [1,2,7-13]. This current study investigated the physiological and psychological effects of three floor positions which may be used as alternatives to prone PR; they were two positions of supine PR, where individual’s arms were either held close to the body at 60° of shoulder abduction (Supine Restraint arms low - SPR-AL) or held further from the body at 100° of shoulder abduction (Supine Restraint arms high – SPR-AH). The third position was right side lying (Side lying restraint -SLR). By increasing our understanding of the impact of PR positions current practice can be improved by advocating which positions create the least adverse impact and therefore maximise the level of safety and minimise the level of harm to those subject to PR. The null hypothesis was stated as there would be no difference in physiological or psychological measures between any of the physical restraint positions tested.
Ethical approval was granted by the School of Health and Rehabilitation Ethics Committee (Keele University, Newcastle-underLyme, United Kingdom). Prior to data collection participants were reminded of their right to withdraw from the study, and signed consent and health screening questionnaires. No incentives were offered or given to participants.
Twenty adults (Male = 10, Female = 10) with no known health problems were recruited and none were excluded. All participants were free from current neuro-musculo-skeletal injuries and cardio-vascular-respiratory risk factors. Age ranged from 18-23 years, mean 20 years (± 1.3). Height ranged from 158.6-197.1 cm, mean 176.1 cm (± 11.2). Weight ranged from 53.4-102.8 Kg, mean 73.8 Kg (± 13.5). BMI (kg/m2) ranged from 19.3-27.8, mean 23.6 (± 2.5).
HP Cosmos Pulsar treadmill; 4 Carefusion MicroLab Spirometer; Disposable Spirometry Mouthpieces; Polar H10 heart rate monitor; Stabilizer™ Pressure Biofeedback unit (Figure 2); Seca 761 weighing scales and 220 Standiometer; Goniometer; Alcohol wipes, 10cm Visual Analogue Scale, and a metric ruler. Equipment was freely available from the school of Health and Rehabilitation, Keele University, UK.
All participants were tested individually. Before each data collection all equipment was calibrated and cleaned. Before sitting for five minutes participants’ height (cm) and weight (Kg) were measured. Whilst sitting the experimental procedures, spirometry technique (without nose clips) and visual analogue scale were explained to each participant after which resting heart rate was measured. Estimated heart rate maximum (HRM) (220 – age) and resting HR were then used to calculate 90% of Heart Rate Reserve (HRRes) (HRM – HR rest x 0.9). Baseline spirometry measures were then taken including Forced Vital Capacity (FVC) and Forced Expiratory Volume in one second (FEV1) (best of three). Next, participants mounted the treadmill and commenced a ramped treadmill protocol which aimed to raise HR to 90% HRRes within five minutes. Once target HR was achieved participants dismounted the treadmill and were restrained by professional instructors in the Management of Actual or Potential Aggression (MAPA) (Figure 1) in the allocated position determined by Triple Latin Square randomisation.
After one minute of PR spirometry measurements (FVC, FEV1) were taken, and after the PR position had been held for a total of five minutes PR was stopped. Before participants commenced their five minute self-paced recovery walk thoracic weight bearing pressure (TWP) was measured (Figure 2) at the posterior chest wall for SPR-AL and SPR-AH, and at the lateral chest wall for SLR using a pressure biofeedback unit.
Recovery between testing in the second restraint position was 45 minutes in duration, as supported by Winter et al. [14]. The third position was tested seven days later as three tests in one day was deemed excessive. Finally, participants completed 10cm Visual Analogue Scales (VAS) that explored their experiences of each position in relation to comfort, anxiety, and breathing limitation. Participants also gave free text responses in relation to their experiences of PR.
The data collected was analysed using Statistical Packages for the Social Sciences Statistics (IBM Corp. version 24.0, Chicago, Illinois, USA). Normal distribution of data was confirmed (Shapiro-Wilk test) and subsequently descriptive and inferential (Paired Sample t-test) statistical analysis was undertaken, with significance set at p < 0.02 following Bonferroni correction to reduce the chance of type 1 error as multiple t-tests were performed.
Results of the physiological and psychological measures taken can be seen in Table 1.
FVC was recorded as 4.8 (±1.1), 4.3 (±0.99), 4.3 (±1.04), and 4.1 (±1.05) litres for baseline, SPR-AL, SPR-AH, and SLR respectively, with SPR-AL and SPR-AH showing a 10.4% reduction from baseline and SLR a 14.6% reduction. FEV1 was recorded as 4.2 litres (±0.8), 3.9 (±0.78), 3.9 (±0.81), and 3.7(±0.85) litres for baseline, SPR-AL, SPR-AH, and SLR respectively, with SPR-AL and SPRAH showing a 7% reduction from baseline and SLR a 12% reduction. The results of this study demonstrate that ventilatory capacity as measured by spirometry was reduced in all restraint positions tested compared to baseline (p = 0.001) with the greatest reduction seen in SLR which was statistically significantly different (p < 0.02) to both SPR-AL and SPR-AH. HR did not differ between the positions tested. SLR imposed the greatest TWP at 116.1 (±17.5) mmHg and was statistically different to both SPR-AL and SRP-AH (p< 0.000). Pressure exerted in SPR-AH was 96.1 (±13.0) mmHg, which was ~17% less than SLR, and SPR-AL pressure was 89.1 (±14.1) mmHg, which was ~23% less than SLR. In relation to psychological measurements the SPR-AL position was the most comfortable with a VAS score of 6.0 (±2.06), followed by SPR-AH VAS 5.6 (±1.57) which was a 6.7% reduction in comfort, and SLR being the least comfortable VAS 3.3 (±1.25) a comfort reduction of 45% compared to SPR-AL. Ratings for perceived Anxiety were 2.7 (±1.30), 3.3 (±1.92), and 5.2 (±1.79) for SPR-AL, SPR-AH and SLR respectively showing SLR to be the most anxiety inducing with SPR-AH and SPR-AL being 36.5% and 48.1% less anxiety inducing respectively. Ratings for perceived Breathing Limitation were 2.9 (±0.92), 3.0 (±1.37), and 5.4 (±1.51) for SPR-AL, SPR-AH and SLR respectively showing SLR imposed the greatest breathing limitation with SPR-AH and SPR-AL being 44.4% and 46.3% respectively less inducing of breathing limitation perception. Free text responses revealed several themes relating to decreased blood flow to the upper limbs with participants complaining of pins and needles, numbness, “dead arm”, and “blood supply felt cut off ” (SLR = 8, SPR-AH = 7, SPR-AL = 5). Limitation in breathing described using words such as feeling “squished”, “trapped”, “suffocated”, and “it was harder to breathe” were most frequently reported in SLR (n=8), then SPR-AH (n=2), and least reported in SPR-AL (n=1).
Our findings were in keeping with our previous work [3,5,6] in that the effect of the PR positions tested were non-homogenous, and that all PR positions tested reduced ventilatory capacity and resulted in negative psychological perceptions for comfort, anxiety, and breathing limitation. The SLR position was found to impose the greatest pressure to the thorax, the greatest ventilatory restriction, and was perceived to be the most anxiety inducing, the least comfortable and the most limiting to breathing when compared to the two supine positions. Barnett et al. [5] reported pressure exerted on the anterior chest wall during unsupported prone restraint (arms abducted) at 102.56 (+24.29) mmHg resulting in a 16% reduction in FVC from baseline, which when in supported prone (arms supporting anterior chest) reduced pressure to 72.74 (+16.9) mmHg, with FVC dropping 11% from baseline. In this current study SLR exerted greater pressure on the thorax (116.1 ±17.5) than did unsupported or supported prone restraint, and reduced FVC by 14.6% compared to 16% for unsupported prone, and 11% for supported prone, therefore the recommendation for the use of SLR as a safer alternative to both prone and supine restraint to minimise the risk of adverse restraint-related outcomes [14] should be challenged.
The reductions in ventilatory capacity seen in the current study were proportional to the extent of the restriction imposed by the restraint position, but did not reach clinical significance, and the perceptions of anxiety, discomfort, and breathing limitation were experienced in an experimental setting. However, PR adverse events occur due to sequelae of cumulative risk factors and it is not known to what extent the ventilatory reductions seen may prove harmful and in what confluence of circumstances risks may occur in a ‘perfect storm’ scenario [3,16] resulting in adverse outcomes. That said, best practice in PR should seek to risk assess each technique / position used so that the safety of the individual is maximised and any potential harm is minimised by seeking to ameliorate as many risks as possible.
This study has shown that the SLR position was perceived to be more psychologically stressful and imposed more pressure on the thorax than both the supine restraint positions investigated. The negative and potentially adverse psychological and physiological effects observed were similar to those induced by unsupported prone restraint [5,6] and support the findings of Parkes et al. [17] suggesting it is erroneous to assume alternatives to prone restraint are homogeneously safer. All restraint positions have the potential for adverse consequences meaning that, regardless of position, PR should always be considered an emergency with the potential for physiological and psychological complications including psychological distress, anatomical injury, physiological compromise and even death.
Methodological strengths of this study included the use of four professional restraint trainers to consistently apply the restraint techniques, and the use of a stringent protocol that covered the procedure of testing and data collection using the same researchers throughout. The use of goniometry and spirometry followed routine clinical practice guidelines, and the construction and use of VAS scales to determine participant perceptions was as suggested by Scott and Huskisson [18] and McCormack et al. [19]. Furthermore, all participants achieved 90% of HRRes by running on the treadmill before being restrained to simulate the exertion of PR. Limitations of this study would be that participants did not struggle against their restraint once restrained, due to ethical considerations, and neither did they possess known risk factors for adverse events occurring during PR.
Our on-going research has demonstrated the potential for negative anatomical, physiological and psychological consequences of several PR positions, by investigating the physiological and psychological impact of supine and side lying PR positions which are often perceived to be safer alternatives to prone PR. All PR positions tested reduced respiratory capacity and resulted in perceptions of discomfort, anxiety, and breathing limitation compared to baseline. SLR was found to possess a significantly greater degree of negative physiological and psychological impact than supine restraint positions. Current guidance suggests avoiding prone restraint where possible however the alternatives are not free from negative physiological and psychological perceptions and as such supine and side lying alternatives should be selected carefully, monitored continuously, and regularly reviewed, with all applications of PR being considered as potential medical emergencies. Further research is required to identify and rank other PR positions and techniques in terms of risk so that staff is better able to make informed decisions during the use of PR in order to maximise safety and minimise harm.

![]()

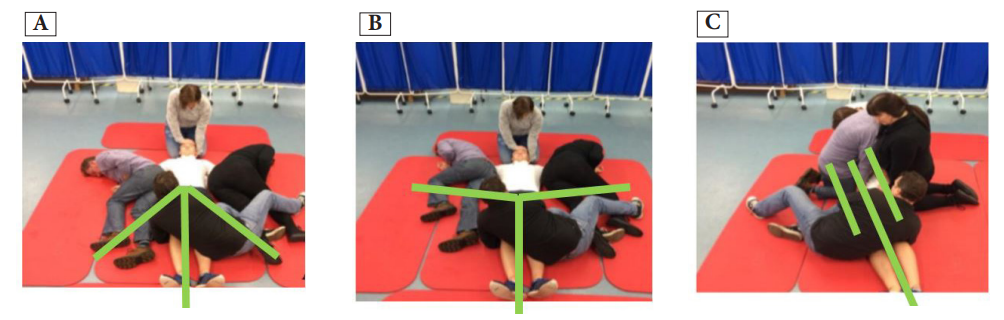 |
| Figure 1: Physical Restraint Positions Investigated (A) Supine arms below 900 (SPR-AL); (B) Supine arms above 900 (SPR-AH); (C) Side Lying on the right (SLR) (Green lines indicate position/angle of arms relative to the body) |
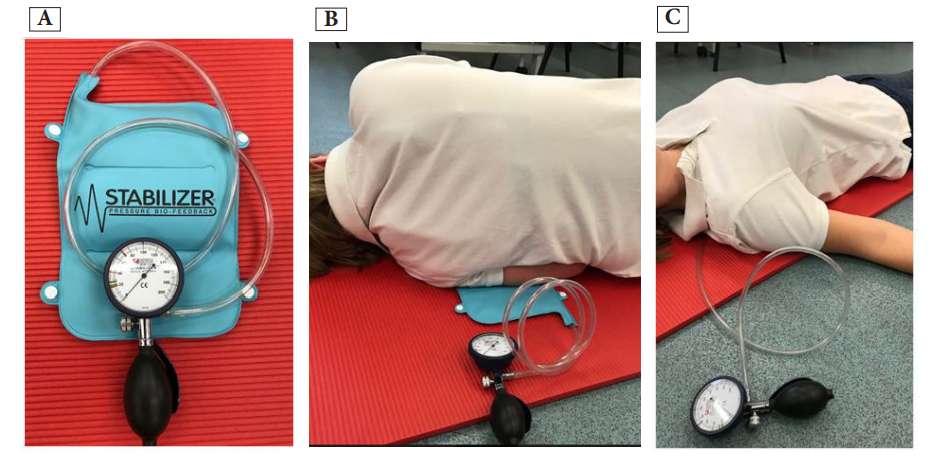 |
| Figure 2: Measurement of Thoracic Weighbearing Pressure: (A) Pressure Biofeedback unit; (B) Measuring Thoracic weight bearing pressure in side lying; (C) Measuring Thoracic weight bearing pressure in supine |
Position |
FVC |
FEV1 |
Heart Rate (bpm) Mean (SD) |
TWP |
Comfort (scale 0-10) Mean (SD) |
Anxiety (scale 0-10) Mean (SD) |
Breathing Limitation (scale 0-10) Mean (SD) |
Baseline |
4.8 |
4.2 |
66 |
NA |
NA |
NA |
NA |
SPR-AL |
4.3 |
3.9 |
137 |
89.1 |
6.0 |
2.7 |
2.9 |
SPR-AH |
4.3 |
3.9 |
136 |
96.1 |
5.6 |
3.3 |
3.0 |
SLR |
4.1 |
3.7 |
136 |
116.1 |
3.3 |
5.2 |
5.4 |




































