Open Access
Research Article
Max Screen
ISSN: 2639-9253
Copyright: © 2020 Kostidou E. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
This article describes the procedure we followed in a small rural medical capacity in Greece, to improve a crucial aspect of the everyday clinical practice and adopt a culture of auto-regulation through the procedure of Audit. As Doctors of the Amfiklia Health Center we are often called to leave the office and deal with emergency cases out of the Health Center. It was common ground that the maintenance of the Emergency Bag we use in these cases is neglected. We audited our practice using certain standards, analyzed the findings, recommended regulations, implemented the changes and re-audited our practice. At the end of this project we managed to ensure that the Emergency Bag has almost all of the necessary drugs and consumables which will be in-date. We also managed to improve our practice with regards to the appropriate recording of the Controlled Drugs used during such cases.
Keywords: Emergency Bag; Audit; Qip; Primary Care; Health Center
Working in Rural Health Centers in Greece often involves provision of services out of the Medical Capacity. This happens in cases where the transfer of the patient is not safe or will take longer for than the Doctor to visit the patient. Occasionally the Doctor will be the only person to assess the patient but sometimes there may be a Paramedic assisting the Doctor. In these cases, the Doctor has to act on the field and possibly be responsible for the transfer of the patient to the nearest appropriate medical capacity. The cases that the Doctor will face range from common Medical and Surgical Emergencies to area-specific cases like agricultural accidents, wildlife-vehicle collisions, road-traffic accidents etc. So far in Greece, there is no strict regulation for the contents of the Emergency Bag that the Doctors carry with them. In the Health Center it has been noticed that many times these bags do not contain basic drugs or equipment. It is well known that this is a fact in other Medical Capacities especially where the staff changes frequently and there is no continuity in the maintenance of the medical supplies. This results in inappropriate treatment with possibly fatal consequences.
To control the compliance of the emergency bag contents with certain guidance we produced.
To introduce regulations regarding the process of checking and restocking the emergency bag contents as well as the registration of the Controlled Drugs (CDs).
This particular QIP took place in the Amfiklia Health Center. This is a Public Primary Care capacity providing service to approximately 6.500 people. We created a Study Group consisted of one General Practitioner, four Rural Doctors, two Nurses and 1 Ambulance Driver. We considered the special emergency cases we come across in Amfiklia. Apart from common medical and surgical emergencies, we are also called to treat snake bites, pesticides poisoning, allergies from local flora/fauna and livestock caused accidents. We also studied the content of an emergency bag as this is suggested by the following resources:
1) Patient Plus; Doctor’s bag contents [1].
2) Primary Care Quality Service Advisory Group; Drugs and Therapeutics Bulletin Drugs for the Doctors Bag: 1 Adults Volume 53 Issue 51 [2].
3) Care Quality Commission; Emergency medicines for GP practices [3].
The Study Group finally came up with a list of 42 items (Appendix 1), based both on the aforementioned resources and the special features of the area we work in. Having created the list with the necessary 42 items for the emergency bag, we then proceeded to an audit and re-audit of our practice. In particular, we controlled our compliance with the following standards:
1) The Emergency bag should contain the drugs/consumables from the list (Appendix 1).
2) The Emergency bag should contain in-date drugs/consumables.
3) The Controlled Drugs (CDs) that are missing should be documented appropriately in the “Used Controlled Drugs” Lists that have been provided by the Local Hospital.
The first random check of the emergency bag was done on 15/07/2017. The results were discussed and analyzed in a Study Group meeting. The Study Group came up with certain recommendations that were implemented and a re-audit was done 11 months later, on 15/06/2018.
The bag contained only 70.0% of the necessary drugs and consumables agreed by the Study Group (Table 1). These drugs and consumables are listed in Appendix 1.
Among the contents of the bag 92.86% were in-date (Table 2).
Among the CDs missing from the Emergency Bag, only 85.37% were recorded appropriately in lists provided by the Local Hospital (Table 3).
Recommendations - Changes in Practice:Upon collection of the data, we concluded that a standardized methodology for the checking and restocking of the emergency bag is of great importance. We introduced certain regulations on that purpose and arranged a meeting of the Staff of the Medical Centre. The Staff members were informed on the situation and the new regulations we introduced. The regulations are the following:
1. Name a responsible staff member for each month;
2. The responsible staff member must check the emergency bags every 15th of the month;
3. A check list must be filled and signed by the responsible staff member after every check (Appendix 3);
4. Copy of the Table with the contents of the Emergency Bag must be kept in the Emergency Bag;
5. The signed check lists of every monthly check should be kept in the doctor’s office;
6. The responsible staff member should follow the following steps for the monthly check;
7. Check the contents of the emergency bag based on the suggested list (Appendix 1);
8. Check the expiry dates of the emergency bag drugs;
9. Restock absent/expired drugs;
10. Ensure the correct documentation of the used CDs by completing the appropriate CDs list (Appendix 2)
The bag contained 95.0% of the necessary medicines and equipment agreed by the Study Group (Table 4, Figure 1).
Among the contents of the bag 100% were in-date (Table 5, Figure 2).
Among the CDs drugs 96.49% were recorded (Table 6, Figure 3).
The results of the first check show that we were failing to have all the necessary supplies in the Emergency Bag. They also show that there were a few expired drugs in the Emergency Bag and that the Controlled Drugs that were missing from the Emergency Bag were not documented appropriately. The findings of the re-audit revealed an improvement in all aspects of our practice. The Emergency Bag contained almost all the necessary supplies (70% to 95% of the suggested drugs and consumables) and there were no expired drugs in it (100% of the drugs and consumables were in-date during the 2nd check). Most importantly, the percentage of the documented used Controlled Drugs increased (85% to 96%).
We were satisfied by the significant improvement in every aspect of our practice, but we discussed the reasons of not achieving 100% compliance in all three standards. We appreciate that the workload and the stress of our job can affect the jobs that are not clearly clinical and involve administration and paperwork. Especially when a Doctor returns from a call back to the Health Center, documenting the Controlled Drugs they used is rarely their priority. However, the prompt restocking of the Emergency Bag and the documentation of the CDs has to be considered as important as the clinical management of a patient. Moreover, the neglected documentation of the used CDs raises legal concerns on whether the missing CDs are not documented on purpose and are used illegally by Staff members who have access to them.
Considering the long-term application of our standardized practice referring to the Emergency Bag, we had to ensure that the methodology and the regulations defined by our team would be imparted to the future personnel of the Health Center. Furthermore, because of our limited financial resources, we had to contact the mayor of the town, explain our purposes and the potential benefit of our practice in order to convince him to dedicate a specific amount of money to our Health Center every month henceforward. These resources would be exploited in buying all drugs and consumables needed so that the Emergency Bag will always contain the necessary in-date stuff.
The prompt restocking of the Emergency Bag and the appropriate recording of the used Controlled Drugs are very important for the best possible treatment of a patient seeking urgent help on the field. Definitely, frequent re-auditing of our practice is necessary to ensure that the standards will remain high. However, this Project has to do with just one of the aspects of our practice. Thus, we consider the familiarization of our Team with the Audit procedure itself as the greatest benefit of this Project. Audit is actually a continuous process of “observe-record-analyze-intervene-evaluate”. Unfortunately, it is not a common process in the Greek Health System. Although it adds workload to the staff, it is the most efficient way to tell whether the things you do every day are correct or not and it is important to be done by the members of the Team who are involved in the audited practice and not by an external observer.
The QIP we described above included an Audit and it was done through active involvement of the Team members. Adopting a non-blame culture, through an established procedure, we raised the awareness of the Staff Members on a very important issue of the everyday practice. Upon completion of this project where auditing of our practice led to proven improvement, we encourage the Audit practice in all fields of clinical practice as a simple and efficient way to maintain and improve the quality of the provided patient care.

![]()

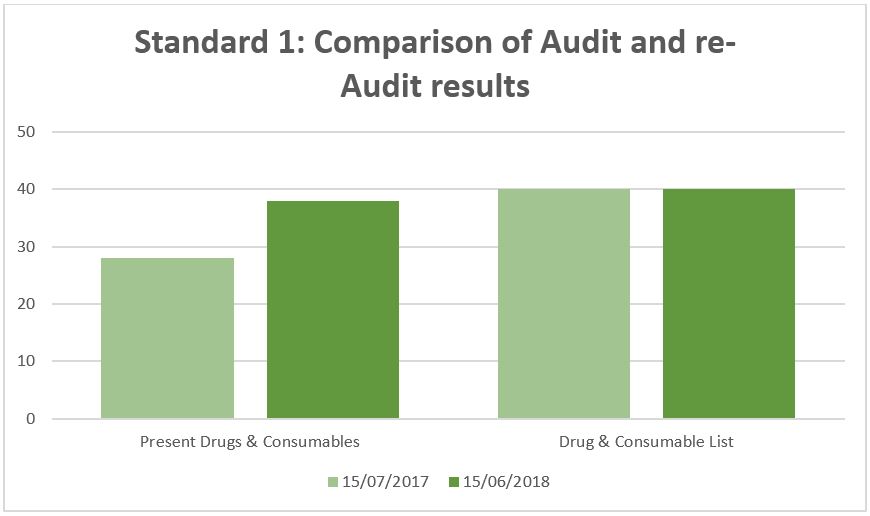 |
| Figure 1: Standard 1: Comparison of Audit and Re-Audit Results |
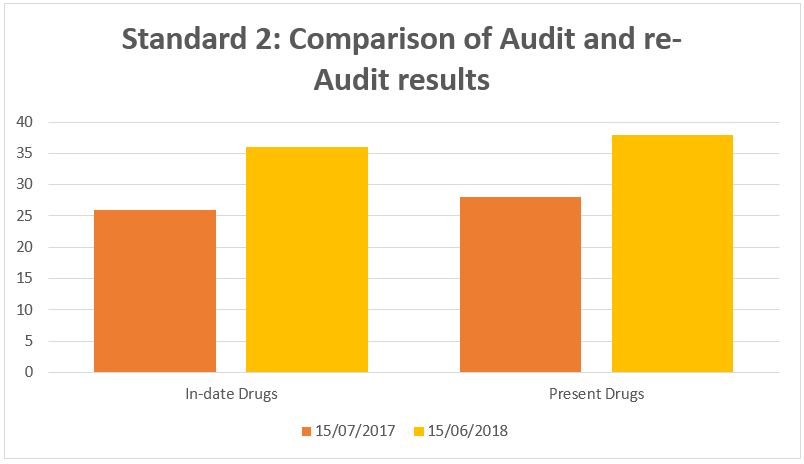 |
| Figure 2: Standard 2: Comparison of Audit and Re-Audit Results |
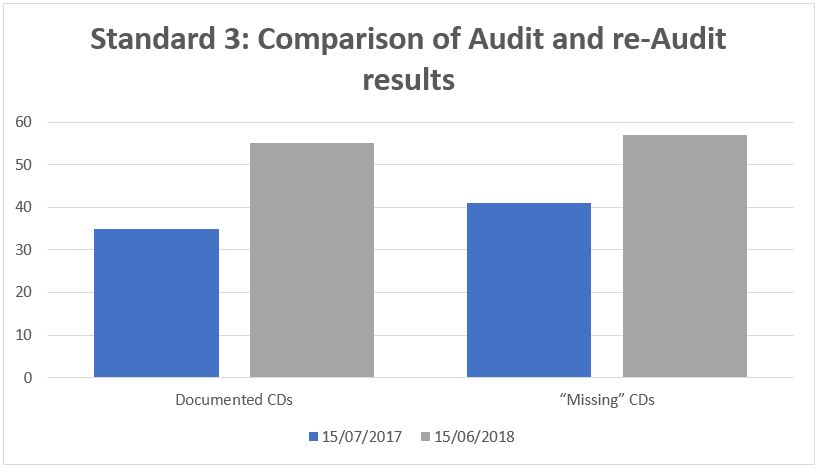 |
| Figure 3: Standard 3: Comparison of Audit and Re-Audit Results |
Total of suggested Drugs/Consumables |
Present in our Emergency Bag |
40 |
28 |
100% |
70% |
Contents of the Emergency Bag |
In-Date |
28 |
26 |
100% |
92,86% |
“Missing” CDs |
Recorded |
41 |
35 |
100 |
85,37% |
|
||
|
Total of suggested Drugs/Consumables |
Present in our Emergency Bag |
1st Data Collection |
40 |
28 |
|
100% |
70% |
2nd Data Collection |
40 |
38 |
|
100% |
95% |
|
|||
|
Contents of the Emergency Bag |
In-Date |
|
1st Data Collection |
28 |
26 |
|
|
100% |
92,86% |
|
2nd Data Collection |
38 |
38 |
|
|
100% |
100% |
|
|
|||
|
“Missing CDs” |
Recorded |
|
1st Data Collection |
41 |
35 |
|
|
100% |
85.37% |
|
2nd Data Collection |
57 |
55 |
|
|
100% |
96.49% |
|




































